Download as pdf or txt
You might also like
- Acute Effects of The Voodoo Flossing Band On Ankle Range of Motion - Philip Stevenson 2019Document10 pagesAcute Effects of The Voodoo Flossing Band On Ankle Range of Motion - Philip Stevenson 2019YngaMarquezJairNo ratings yet
- ACL Tibial Fixation MedthodsDocument8 pagesACL Tibial Fixation MedthodsCleff FlowersNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- A Systematic Review of Outcomes Reporting For Brachial Plexus ReconstructionDocument6 pagesA Systematic Review of Outcomes Reporting For Brachial Plexus ReconstructionAndrés Urrego NietoNo ratings yet
- Grieve Et Al - LMF, Tornozelo - 2022Document7 pagesGrieve Et Al - LMF, Tornozelo - 2022felipe alvesNo ratings yet
- Effect of Spinal Fusion On Joint Space Narrowing of The Hip: Comparison Among Non-Fusion, Short Fusion, and Middle or Long FusionDocument8 pagesEffect of Spinal Fusion On Joint Space Narrowing of The Hip: Comparison Among Non-Fusion, Short Fusion, and Middle or Long FusionMaximilian SNo ratings yet
- GWTDocument7 pagesGWTBagus Yudha PratamaNo ratings yet
- Comparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementDocument15 pagesComparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementIJAR JOURNALNo ratings yet
- OUtcome After Limted or Extensive BursectomyDocument8 pagesOUtcome After Limted or Extensive BursectomySeno adipNo ratings yet
- The Effectiveness of Shoulder Stretching and Joint Mobilizations On Posterior Shoulder TightnessDocument8 pagesThe Effectiveness of Shoulder Stretching and Joint Mobilizations On Posterior Shoulder TightnessKlgo. Fernando HuertaNo ratings yet
- Adductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionDocument9 pagesAdductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionElaine CspNo ratings yet
- 1 s2.0 S0020138323006873 MainDocument6 pages1 s2.0 S0020138323006873 MainAliif MaulanaNo ratings yet
- Evaluation Kinaesthetic Proprioceptive Deficit After Knee Anterior Cruciate Ligament (ACL) Reconstruction in AthletesDocument7 pagesEvaluation Kinaesthetic Proprioceptive Deficit After Knee Anterior Cruciate Ligament (ACL) Reconstruction in AthletesAndy Delos ReyesNo ratings yet
- Global Sagittal Alignment of The Spine, Pelvis, Lower Limb After Vertebral Compression Fracture and Its Effect On Quality of LifeDocument7 pagesGlobal Sagittal Alignment of The Spine, Pelvis, Lower Limb After Vertebral Compression Fracture and Its Effect On Quality of Lifelauchunman1No ratings yet
- 2018-1 - Classifications in Brief Tonnis Classification of Hip OsteoarthritisDocument5 pages2018-1 - Classifications in Brief Tonnis Classification of Hip OsteoarthritisjosedgalvismdNo ratings yet
- Quant - MyotonDocument29 pagesQuant - Myotonachsahjames04No ratings yet
- 10.1186/s12891 023 06805 ZDocument7 pages10.1186/s12891 023 06805 Zrenatoed.gomezNo ratings yet
- A Systematic Review of Bracing Following Reconstruction of The ACLDocument10 pagesA Systematic Review of Bracing Following Reconstruction of The ACLDanar AdhimuktiNo ratings yet
- Imaging in Osteoarthritis 2021 YjocaDocument22 pagesImaging in Osteoarthritis 2021 Yjocaal malikNo ratings yet
- 2023 Article 4357Document8 pages2023 Article 43576130019037 FATCHUR RIZQI HAMZAHNo ratings yet
- Kinematic Gait Analysis of Workers Exposed To KneeDocument7 pagesKinematic Gait Analysis of Workers Exposed To KneeSamNo ratings yet
- Hips Ambulatory Function 3 Months 2023Document7 pagesHips Ambulatory Function 3 Months 2023dr.sbarrosoNo ratings yet
- Physiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesDocument10 pagesPhysiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesLindapratama SaifuddinNo ratings yet
- Función Muscular y MaloclusiónDocument10 pagesFunción Muscular y MaloclusiónManuela Morales QuinteroNo ratings yet
- The New in Sport Medicine 2011Document10 pagesThe New in Sport Medicine 2011Daniel G. A. C.No ratings yet
- Systematic ReviewDocument7 pagesSystematic ReviewErwin WibowoNo ratings yet
- 2023 Plotkin Hip Thrust and Back Squat Training Elicit Similar GluteusDocument13 pages2023 Plotkin Hip Thrust and Back Squat Training Elicit Similar GluteusalexandremagnopersonalNo ratings yet
- Partial-Thickness Articular Surface Rotator Cuff Tears: An All-Inside Repair TechniqueDocument7 pagesPartial-Thickness Articular Surface Rotator Cuff Tears: An All-Inside Repair TechniqueCsiszar AporNo ratings yet
- Does Standing Protect Bone Density in Patients WithDocument5 pagesDoes Standing Protect Bone Density in Patients WithManos AndriolasNo ratings yet
- Determining The Stabilizing Role of Individual Torso Muscles During Rehabilitation ExercisesDocument13 pagesDetermining The Stabilizing Role of Individual Torso Muscles During Rehabilitation Exercisesx-ray7No ratings yet
- Quadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateDocument21 pagesQuadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateAthenaeum Scientific PublishersNo ratings yet
- Two Years Outcome of Cemented Austin Moore HemiartDocument7 pagesTwo Years Outcome of Cemented Austin Moore HemiartIkram HussainNo ratings yet
- Slight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative StudyDocument8 pagesSlight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative Studyfebyan yohanesNo ratings yet
- The Influence of Menstrual Cycle On The Efficiency of StretchingDocument7 pagesThe Influence of Menstrual Cycle On The Efficiency of StretchingAlejandra GutierrezNo ratings yet
- Ergonomics in MicrosurgeryDocument5 pagesErgonomics in MicrosurgerylenoNo ratings yet
- Physical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookDocument9 pagesPhysical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookLing Pong HungNo ratings yet
- Tendon 2Document10 pagesTendon 2Verónica Téllez ArriagaNo ratings yet
- A Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryDocument10 pagesA Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryRini MaghfirahNo ratings yet
- Clinically Significant Outcomes After Meniscectomy 2019Document12 pagesClinically Significant Outcomes After Meniscectomy 2019asmaNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- Arthroplasty TodayDocument5 pagesArthroplasty TodayTya VenyNo ratings yet
- Clinical Practice and Effectiveness of Kinesio Taping For Lower Limb Musculoskeletal Disorder: A Systematic AppraisalDocument15 pagesClinical Practice and Effectiveness of Kinesio Taping For Lower Limb Musculoskeletal Disorder: A Systematic Appraisalد.موسى التويتيNo ratings yet
- Hip Muscle Atrophy and Hip Osteoarthritis Evidence and Continuing ChallengesDocument9 pagesHip Muscle Atrophy and Hip Osteoarthritis Evidence and Continuing ChallengesAthenaeum Scientific PublishersNo ratings yet
- FulltextDocument6 pagesFulltextdespNo ratings yet
- (2023) Effects of Running On The Development of Knee OsteoarthritisDocument6 pages(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995No ratings yet
- Review Article: Systematic Exposure in Revision Total Hip Arthroplasty: The Posterior ApproachDocument10 pagesReview Article: Systematic Exposure in Revision Total Hip Arthroplasty: The Posterior ApproachJanethNo ratings yet
- Gait & Posture: ReviewDocument14 pagesGait & Posture: ReviewNicolásCuartasVerjelNo ratings yet
- 1 s2.0 S106345842200838X MainDocument12 pages1 s2.0 S106345842200838X Maingck85fj8pnNo ratings yet
- Efcacy of Acupuncture CombinedDocument21 pagesEfcacy of Acupuncture Combined4evertigerNo ratings yet
- Test-Re-Test Reliability and Inter-Rater Reliability of A Digital Pelvic Inclinometer in Young, Healthy Males and FemalesDocument15 pagesTest-Re-Test Reliability and Inter-Rater Reliability of A Digital Pelvic Inclinometer in Young, Healthy Males and FemalesfilorpgNo ratings yet
- Total Hip Arthroplasty After Rotational AcetabularDocument9 pagesTotal Hip Arthroplasty After Rotational AcetabularluisNo ratings yet
- Computational Biomechanics of Knee Joint in Open KDocument9 pagesComputational Biomechanics of Knee Joint in Open KLma OmranNo ratings yet
- Fatty Infiltration and Atrophy of The Rotator Cuff Do Not Improve After Rotator Cuff Repair and Correlate With Poor Functional Outcome PDFDocument10 pagesFatty Infiltration and Atrophy of The Rotator Cuff Do Not Improve After Rotator Cuff Repair and Correlate With Poor Functional Outcome PDFEllan Giulianno FerreiraNo ratings yet
- MRI, Força de ExtensoresDocument16 pagesMRI, Força de ExtensoresRosaneLacerdaNo ratings yet
- Esska Knee Munich Doc 18Document16 pagesEsska Knee Munich Doc 18Avram GeorgievNo ratings yet
- Estimation of Two Wear Factors For Total Hip ArthrDocument8 pagesEstimation of Two Wear Factors For Total Hip ArthrMauricio MoncadaNo ratings yet
- Avaliação Ultrassonográfica Do Músculo Genio-Hióideo e Osso Hióide Durante A Deglutição em Adultos Jovens PDFDocument6 pagesAvaliação Ultrassonográfica Do Músculo Genio-Hióideo e Osso Hióide Durante A Deglutição em Adultos Jovens PDFGiovanna MartinsNo ratings yet
- Compositional MRI Techniques For Evaluation of Cartilage DegenerationDocument15 pagesCompositional MRI Techniques For Evaluation of Cartilage DegenerationAnonymous ZSmSZErTqtNo ratings yet
- Sports - A Multi-Experiment Investigation of The Effects Stance Width On The Biomechanics of The Barbell SquatDocument15 pagesSports - A Multi-Experiment Investigation of The Effects Stance Width On The Biomechanics of The Barbell SquatmauricioNo ratings yet
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentFrom EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchNo ratings yet
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDocument7 pagesOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040No ratings yet
- Humerus Fractures (Proximal & Shaft)Document47 pagesHumerus Fractures (Proximal & Shaft)Malueth AnguiNo ratings yet
- Int Obs PDFDocument37 pagesInt Obs PDFsurgeon77No ratings yet
- Journal of Orthopaedic Science: Chin-Kai Huang, Chih-Kai Hong, Fa-Chuan Kuan, Wei-Ren Su, Kai-Lan HsuDocument4 pagesJournal of Orthopaedic Science: Chin-Kai Huang, Chih-Kai Hong, Fa-Chuan Kuan, Wei-Ren Su, Kai-Lan Hsuanasofia.vargas22No ratings yet
- Technique of Internal Fixation of Fractures 1st 1965Document280 pagesTechnique of Internal Fixation of Fractures 1st 1965nguyen namNo ratings yet
- YoDocument9 pagesYoRadyusman RajagukgukNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- Oral Implants: The Paradigm Shift in Restorative Dentistry: JDR Centennial SeriesDocument7 pagesOral Implants: The Paradigm Shift in Restorative Dentistry: JDR Centennial SeriesShirmayne TangNo ratings yet
- Sutural Cataract Ophthalmic ImagesDocument1 pageSutural Cataract Ophthalmic ImagesLorenaNo ratings yet
- Hip SolutionsDocument4 pagesHip Solutionsapi-19808945No ratings yet
- Abdominal Aortic Aneurysm: AetiologyDocument7 pagesAbdominal Aortic Aneurysm: AetiologyKelvin MaikanaNo ratings yet
- MastelDocument13 pagesMastelCharles TitoneNo ratings yet
- West Middlesex University Hospital Site MapDocument1 pageWest Middlesex University Hospital Site Mapin12kamal123No ratings yet
- EN IV Torso BrochureDocument2 pagesEN IV Torso BrochureVJNo ratings yet
- AORN Guideline For Electrosurgical Safety Evidence TableDocument20 pagesAORN Guideline For Electrosurgical Safety Evidence Tablewaldemar russellNo ratings yet
- Views Catheters and Wires PDFDocument47 pagesViews Catheters and Wires PDFRedhwan Abdullah qaid AlshubiNo ratings yet
- Accumbens Connectivity During Deep-Brain Stimulation Differentiates Loss of Control From Physiologic Behavioral StatesDocument8 pagesAccumbens Connectivity During Deep-Brain Stimulation Differentiates Loss of Control From Physiologic Behavioral States焦扬No ratings yet
- Surgical Approaches To The Facial Skeleton 3rd Edition Ebook PDFDocument47 pagesSurgical Approaches To The Facial Skeleton 3rd Edition Ebook PDFmary.burklow183100% (50)
- Hirschsprung Disease Managed With One-Stage TransaDocument6 pagesHirschsprung Disease Managed With One-Stage TransaTetra JRNo ratings yet
- Soft Versus Hard Occlusal Splint Therapy in The Management of Temporomandibular Disorders (TMDS)Document7 pagesSoft Versus Hard Occlusal Splint Therapy in The Management of Temporomandibular Disorders (TMDS)botak berjamaahNo ratings yet
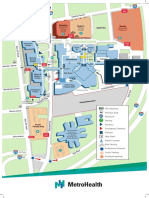
- Main Campus Map Version March 2021Document2 pagesMain Campus Map Version March 2021cjarcher1677No ratings yet
- STRATEGIC-MANAGEMENT-PAPER - Lung Center PhilippinesDocument48 pagesSTRATEGIC-MANAGEMENT-PAPER - Lung Center PhilippinesDave VillasantaNo ratings yet
- DNB Thesis Topics in RadiodiagnosisDocument5 pagesDNB Thesis Topics in Radiodiagnosisgjaj8vvw100% (2)
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- Self ReflectionDocument2 pagesSelf ReflectionUdayana0% (1)
- FIX - Fracture and DislocationDocument80 pagesFIX - Fracture and DislocationWildan Hilmi AnsoriNo ratings yet
- Current Advances in Surgical Management of Ruminal Disorders of BovineDocument7 pagesCurrent Advances in Surgical Management of Ruminal Disorders of BovineKazi Zihadul AlamNo ratings yet
- Malrotation of Gut: Pravin NarkhedeDocument44 pagesMalrotation of Gut: Pravin Narkhedepravin narkhede0% (1)
- Benign Breast Papilloma: Is Surgical Excision Necessary?: Original ArticleDocument6 pagesBenign Breast Papilloma: Is Surgical Excision Necessary?: Original Articleyongky sugandaNo ratings yet
- Ogilvie SyndromeDocument8 pagesOgilvie SyndromeMuhammad FaisalNo ratings yet