Download as pdf or txt
You might also like
- ICO Advanced 115 MCQs 2015-2019Document69 pagesICO Advanced 115 MCQs 2015-2019mrs eleven100% (1)
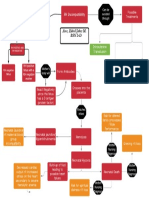
- Basic Concept Map - RH IncompatibilityDocument1 pageBasic Concept Map - RH IncompatibilityTechnoShindoNo ratings yet
- Health Teaching PlanDocument3 pagesHealth Teaching PlanditamandaNo ratings yet
- Cardiac Markers: Presented: by Rubaina Ali Presented To: Dr. Blessy K George, Department of Pharmacy PracticeDocument64 pagesCardiac Markers: Presented: by Rubaina Ali Presented To: Dr. Blessy K George, Department of Pharmacy Practicepavani valluriNo ratings yet
- 13 FullDocument16 pages13 FullGyse LemaNo ratings yet
- Advanced Cholesterol TestingDocument36 pagesAdvanced Cholesterol TestingJarri NajamNo ratings yet
- Dyslipidemia MXDocument72 pagesDyslipidemia MXsruthimeena6891No ratings yet
- 23 Preventive Heart Disease, Dyslipidemia and HTNDocument13 pages23 Preventive Heart Disease, Dyslipidemia and HTNVictor PazNo ratings yet
- DyslipidemiaDocument30 pagesDyslipidemiaNour Sa'eedNo ratings yet
- Triglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusDocument4 pagesTriglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusTanveerNo ratings yet
- Lipid, Lipoprotein and Coronary Artery DiseaseDocument49 pagesLipid, Lipoprotein and Coronary Artery DiseaseMuhammad DaviqNo ratings yet
- K 30 - Kuliah Dislipidemia Update (Desktop-Doosshg's Conflicted Copy 2018-06-12)Document45 pagesK 30 - Kuliah Dislipidemia Update (Desktop-Doosshg's Conflicted Copy 2018-06-12)Reina TarihoranNo ratings yet
- Cardiovascular Disease: Interpretation of Clinical DataDocument39 pagesCardiovascular Disease: Interpretation of Clinical DataSapta DenyNo ratings yet
- DyslipidemiaDocument53 pagesDyslipidemiaRey AlwiwikhNo ratings yet
- Kuliah DislipidemiaDocument45 pagesKuliah DislipidemiaPaul Behring ManurungNo ratings yet
- Medical Nutrition Therapy For Cardiovascular DiseaseDocument210 pagesMedical Nutrition Therapy For Cardiovascular DiseaseBok MatthewNo ratings yet
- Midterms CBLDocument11 pagesMidterms CBLstar220498No ratings yet
- HDL Muy Alto 2019Document10 pagesHDL Muy Alto 2019Luis C Ribon VNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliNo ratings yet
- Inborn Errors of Lipid MetabolismDocument41 pagesInborn Errors of Lipid MetabolismWalterNo ratings yet
- Chapter 24 - DylipidaemiaDocument7 pagesChapter 24 - DylipidaemiaMark Harold GonzalesNo ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Etiology and Management of Dyslipidemia in ChildrenDocument12 pagesEtiology and Management of Dyslipidemia in ChildrenAmallia Nuggetsiana SetyawatiNo ratings yet
- A Modern Approach To Dyslipidemia: ReviewDocument43 pagesA Modern Approach To Dyslipidemia: ReviewElberNo ratings yet
- Familial Hyperlipidemia Type 2a - StatPearls - NCBI BookshelfDocument6 pagesFamilial Hyperlipidemia Type 2a - StatPearls - NCBI BookshelfMohammed shamiul ShahidNo ratings yet
- PHAR 233 - Pathophysiology of CVS DisordersDocument116 pagesPHAR 233 - Pathophysiology of CVS DisordersLina RamojNo ratings yet
- TX LipidosDocument14 pagesTX Lipidosxander trujilloNo ratings yet
- Study-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsDocument17 pagesStudy-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsDan Dan ManaoisNo ratings yet
- 1 HipercolesterolemiaDocument6 pages1 HipercolesterolemiaJesús Mtz Del CastilloNo ratings yet
- Hypercholesterolaemia and Its Management: Clinical ReviewDocument6 pagesHypercholesterolaemia and Its Management: Clinical ReviewAchmad Faiz SulaimanNo ratings yet
- Case 260Document6 pagesCase 260Spencer KrollNo ratings yet
- LipidDocument31 pagesLipidahmed abd elazizNo ratings yet
- 8E - Lipid Sirt Study JANA 2010Document6 pages8E - Lipid Sirt Study JANA 2010alonso martinNo ratings yet
- Dyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesDocument7 pagesDyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesAmelie AnsonNo ratings yet
- Journal Article-Advances - in - Treatment - of - DyslipidemiaDocument19 pagesJournal Article-Advances - in - Treatment - of - DyslipidemiaLauv LoveNo ratings yet
- Pr2 Chapter 1 3 Peta Icamina 2Document21 pagesPr2 Chapter 1 3 Peta Icamina 2JOHN ICAMINANo ratings yet
- Familial HyperlipidemiaDocument3 pagesFamilial Hyperlipidemiaalex.ttkNo ratings yet
- Diretriz - Dislipidemia EndocrinologiaDocument70 pagesDiretriz - Dislipidemia EndocrinologiaSamara QueirozNo ratings yet
- Familial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Document43 pagesFamilial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Gourav Kumar SinhaNo ratings yet
- Notes Chapter 35Document16 pagesNotes Chapter 35Christene GVNo ratings yet
- Cerebral Blood Flow StrokeDocument122 pagesCerebral Blood Flow Strokeapi-3748748No ratings yet
- ApoB 2Document7 pagesApoB 2Alex AlexNo ratings yet
- Pattern of Dyslipidemia in Type Diabetic Subjects in Eastern NepalDocument3 pagesPattern of Dyslipidemia in Type Diabetic Subjects in Eastern NepalDR VENKATARAMANA MurthyNo ratings yet
- Penyakit Jantung Koroner (Coronary Heart Disease)Document57 pagesPenyakit Jantung Koroner (Coronary Heart Disease)Wina DeskyNo ratings yet
- Desirable - Less Than 200 MG/DL Borderline High Risk - 200-239 MG/DL High Risk - 240 MG/DL and OverDocument62 pagesDesirable - Less Than 200 MG/DL Borderline High Risk - 200-239 MG/DL High Risk - 240 MG/DL and OverAdib RahmanNo ratings yet
- Lipid Management in Patients With Endocrine Disorders An EndocrineDocument70 pagesLipid Management in Patients With Endocrine Disorders An Endocrinealialison7666No ratings yet
- Clinical Science High Ratio of Triglycerides To Hdl-Cholesterol Predicts Extensive Coronary DiseaseDocument6 pagesClinical Science High Ratio of Triglycerides To Hdl-Cholesterol Predicts Extensive Coronary DiseaseMarj MendezNo ratings yet
- Mbs127 Slide DislipidemiaDocument45 pagesMbs127 Slide DislipidemiaDaru KristiyonoNo ratings yet
- AtherosclerosisDocument29 pagesAtherosclerosisneeraj banaNo ratings yet
- S 21 Trejtnar AntidyslipidemicsDocument47 pagesS 21 Trejtnar AntidyslipidemicsCarlo MaxiaNo ratings yet
- Emerging Risk Factors For CAD - PDFDocument35 pagesEmerging Risk Factors For CAD - PDFdinnhanifahNo ratings yet
- Methods For Measuremnent of LDL CholesterolDocument19 pagesMethods For Measuremnent of LDL Cholesterolmaheren tubeNo ratings yet
- Samuel VinhoDocument5 pagesSamuel Vinhosamuel rangelNo ratings yet
- Glass Witztum2001Document14 pagesGlass Witztum2001NicoNo ratings yet
- Atherosclerosis and Ischemic Heart Disease: UtlineDocument8 pagesAtherosclerosis and Ischemic Heart Disease: UtlinevmdcabanillaNo ratings yet
- Cerebral Blood Flow and Ischemic Brain Disease: Bernardo L. Conde, M.DDocument70 pagesCerebral Blood Flow and Ischemic Brain Disease: Bernardo L. Conde, M.DIon UrsuNo ratings yet
- LDL InggDocument7 pagesLDL InggDuti AprilniNo ratings yet
- Cardiovascular Diseases and Hyperlipidemias: Continuing.Document19 pagesCardiovascular Diseases and Hyperlipidemias: Continuing.Zai ZaiNo ratings yet
- Cardiovascular Disorders: Annette HaynesDocument69 pagesCardiovascular Disorders: Annette HaynesBinh Yen Quach TranNo ratings yet
- Medical Nutrition Therapy in Cardiovascular DiseaseDocument93 pagesMedical Nutrition Therapy in Cardiovascular DiseasesariNo ratings yet
- Tu Lenko 2002Document12 pagesTu Lenko 2002catalina infanteNo ratings yet
- rối loạn lipid máu PDFDocument107 pagesrối loạn lipid máu PDFNguyễn MaiNo ratings yet
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Template List Mapping Obat AfiDocument242 pagesTemplate List Mapping Obat AfiZurlin DwirostantinNo ratings yet
- List Nama Anafilaktik & Emergency KitDocument7 pagesList Nama Anafilaktik & Emergency KitZurlin DwirostantinNo ratings yet
- Daftar List TEDocument6 pagesDaftar List TEZurlin DwirostantinNo ratings yet
- Updates On Pulmonary HypertensionDocument39 pagesUpdates On Pulmonary HypertensionZurlin DwirostantinNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- P.R.I.IN. People Readiness in (First Aid) Intervention: - Bone and Joint InjuriesDocument35 pagesP.R.I.IN. People Readiness in (First Aid) Intervention: - Bone and Joint InjurieschristopherNo ratings yet
- Final Concept MapDocument7 pagesFinal Concept Mapapi-405374041No ratings yet
- PA - Coursepack DAY 1Document352 pagesPA - Coursepack DAY 1Elly NuñezNo ratings yet
- Tonsillitis & TonsillectomyDocument18 pagesTonsillitis & TonsillectomyLuqman HakimNo ratings yet
- Levofloxacin 500mg Film-Coated Tablets - Summary of Product Characteristics (SMPC)Document10 pagesLevofloxacin 500mg Film-Coated Tablets - Summary of Product Characteristics (SMPC)OdunlamiNo ratings yet
- Respiratory Disorder - NclexDocument27 pagesRespiratory Disorder - NclexDefensor Pison GringgoNo ratings yet
- Department of Internal Medicine,: Prof WBP Matuja Muhas/MnhDocument31 pagesDepartment of Internal Medicine,: Prof WBP Matuja Muhas/MnhDanyu KibuguluNo ratings yet
- Case ReportDocument13 pagesCase Reportfall autumnNo ratings yet
- A Position Paper On The Cause of DengvaxiaDocument3 pagesA Position Paper On The Cause of DengvaxiaCristine Joy Remerata Villarosa50% (10)
- Giant-Cell Tumor of Bone (GCT) Is Bone Primary Tumor That Usually Happen in Young Adult Between 20-40 Years OldDocument6 pagesGiant-Cell Tumor of Bone (GCT) Is Bone Primary Tumor That Usually Happen in Young Adult Between 20-40 Years OldIbm IbamNo ratings yet
- Daftar Pustaka KtiDocument6 pagesDaftar Pustaka KtiayuNo ratings yet
- Cerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019Document38 pagesCerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019Anjali GuptaNo ratings yet
- RT PCR Test ReportDocument2 pagesRT PCR Test ReportMoumita MandalNo ratings yet
- 4th Quarter Pre Test in Con ChemDocument4 pages4th Quarter Pre Test in Con ChemEzzy SantosNo ratings yet
- OSCE Checklists (History and Examination)Document33 pagesOSCE Checklists (History and Examination)Waleed MohmmedNo ratings yet
- Sts Gene TherapyDocument2 pagesSts Gene TherapyDuane OrejolaNo ratings yet
- Tarea 2 de Ingles 2Document6 pagesTarea 2 de Ingles 2Rosa RamosNo ratings yet
- BCG Vaccine EDocument17 pagesBCG Vaccine Edr.kendrickNo ratings yet
- Dr. Kobal Low CarbDocument42 pagesDr. Kobal Low CarbGhea Putri HendrianiNo ratings yet
- EnuresisDocument32 pagesEnuresisMorteza DehnookhalajiNo ratings yet
- 24hr Fluid Balance ADULT Chart - v3Document2 pages24hr Fluid Balance ADULT Chart - v3anggita diah100% (1)
- ANNEX B - LGU Information SheetDocument2 pagesANNEX B - LGU Information SheetToni Quitalig GamezNo ratings yet
- Genetic Disorders PDFDocument38 pagesGenetic Disorders PDFEllen Mae PrincipeNo ratings yet
- Mary C. Gomez, MD, DPBP, FPPA Child, Adolescent, Adult PsychiatristDocument66 pagesMary C. Gomez, MD, DPBP, FPPA Child, Adolescent, Adult Psychiatristxiejie22590No ratings yet
- Radiofrequency AblationDocument7 pagesRadiofrequency AblationRohit singhNo ratings yet
- Ankylosing SpondylitisDocument4 pagesAnkylosing SpondylitisHenry TirtosuhartoNo ratings yet