Download as pdf or txt
You might also like
- TWU Anesthesia Cheat SheetDocument2 pagesTWU Anesthesia Cheat Sheetinvading_jam7582100% (6)
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesMigs Migue100% (12)
- P2 Top 200 Part 1Document10 pagesP2 Top 200 Part 1Drashtibahen PatelNo ratings yet
- Child Protection Systems in Emergencies Child Protection Systems in EmergenciesDocument34 pagesChild Protection Systems in Emergencies Child Protection Systems in EmergenciesghawsaddinNo ratings yet
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Bob Beck Protocol - Natural Cancer Treatments at CancerTutorDocument4 pagesBob Beck Protocol - Natural Cancer Treatments at CancerTutorThiago NunesNo ratings yet
- HES School Closure 8 - 14!8!21 - 2020Document3 pagesHES School Closure 8 - 14!8!21 - 2020Mindy WadleyNo ratings yet
- Chapter 20 - Cardiac EmergenciesDocument96 pagesChapter 20 - Cardiac EmergenciesAmit KlNo ratings yet
- ABCDE Approach To The Critically Ill Patient - Nick SmithDocument40 pagesABCDE Approach To The Critically Ill Patient - Nick SmithBadrul Hisyam Alias100% (1)
- Emergency Nephrology - Hyponatremia Approach & ManagementDocument1 pageEmergency Nephrology - Hyponatremia Approach & ManagementEarn PhongpetraNo ratings yet
- Hematology System Lec. 2Document32 pagesHematology System Lec. 2xqfs2cd44sNo ratings yet
- Hypon at R em Ia: ST Epw Ise Appr Oach T o Diagn Osis: Ser U M Sodiu M 135 M M Ol/ LDocument1 pageHypon at R em Ia: ST Epw Ise Appr Oach T o Diagn Osis: Ser U M Sodiu M 135 M M Ol/ LMaría José GalvisNo ratings yet
- HiponatremiaDocument6 pagesHiponatremiaRaka PrazastaNo ratings yet
- Disorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NDocument41 pagesDisorders of Sodium: Presenter: DR Bharath Kumar P Moderator: DR Ramesh K NBharath Kumar PamulapatiNo ratings yet
- Decontamination Information: BathingDocument2 pagesDecontamination Information: BathingNaNo ratings yet
- ClinPath-10.2 - Urine and Other Body FluidsDocument4 pagesClinPath-10.2 - Urine and Other Body FluidsSanielle Karla Garcia LorenzoNo ratings yet
- DKA ProtocolDocument3 pagesDKA Protocolpinky222255554100% (1)
- Health RecordDocument9 pagesHealth RecordNabajit BaruahNo ratings yet
- HyponatremiaDocument40 pagesHyponatremiaarchana p sNo ratings yet
- Medical Surgical 1 PDFDocument19 pagesMedical Surgical 1 PDFheyyymeeeNo ratings yet
- LA GeneralDocument2 pagesLA GeneralNicole CardenasNo ratings yet
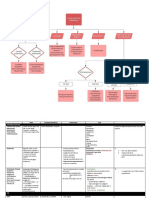
- CONCEPT-MAP 2 GastroDocument1 pageCONCEPT-MAP 2 GastroShimri MagsicoNo ratings yet
- Drug Study - FurosemideDocument2 pagesDrug Study - FurosemideKian HerreraNo ratings yet
- Montalban-Cc2 Lec EaDocument5 pagesMontalban-Cc2 Lec Eakimmynemil80No ratings yet
- Cough and Cold PrepDocument3 pagesCough and Cold PrepJOSLIN ROZ GALILEANo ratings yet
- PharmDrug List Complete SGU-USTDocument116 pagesPharmDrug List Complete SGU-USTMary Camille AzarconNo ratings yet
- Hypoglycemia in The Newborn and Infant: M.A. Sperling O. Escobar O. Pinhas-HamielDocument2 pagesHypoglycemia in The Newborn and Infant: M.A. Sperling O. Escobar O. Pinhas-HamielDaniela CioboataNo ratings yet
- Ferrous Sulfate Drug StudyDocument1 pageFerrous Sulfate Drug Studyjanice paralejas100% (1)
- Poster On Epilepsy Management in CaninesDocument1 pagePoster On Epilepsy Management in Caninessai hemachandNo ratings yet
- Er MathDocument17 pagesEr MathMichael RamosoNo ratings yet
- Sepsis Quick Reference GuideDocument1 pageSepsis Quick Reference GuideRavin DebieNo ratings yet
- Summary of DiureticsDocument3 pagesSummary of DiureticsHaris SaeedNo ratings yet
- Anaphylactic ShockDocument7 pagesAnaphylactic ShockKat QNo ratings yet
- Tec Grave IsraelDocument1 pageTec Grave IsraelJorge DíazNo ratings yet
- Caso AnemiaDocument2 pagesCaso AnemiakennethNo ratings yet
- ToxicologyDocument7 pagesToxicologysaadalotaibi31No ratings yet
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianNo ratings yet
- Ek Ah YG EIA: AlbuminDocument1 pageEk Ah YG EIA: AlbuminRebekah EquizNo ratings yet
- YH Neonatal Paediatric Hyperammonaemia GuidelineDocument9 pagesYH Neonatal Paediatric Hyperammonaemia GuidelineTrishenth FonsekaNo ratings yet
- Intravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineDocument9 pagesIntravenous Anaesthetics: Thiopentone Methohexitone Propofol KetamineTomNo ratings yet
- Ipratropium SalbutamolDocument2 pagesIpratropium SalbutamolGwyn RosalesNo ratings yet
- b8 - Anticholinesterase DrugsDocument11 pagesb8 - Anticholinesterase DrugsNav ThiranNo ratings yet
- Adult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateDocument1 pageAdult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateRyggie Comelon0% (1)
- D5LRDocument2 pagesD5LRjonoelc100% (5)
- b8 - Ache InhibitorsDocument16 pagesb8 - Ache InhibitorsNav ThiranNo ratings yet
- Catalogue HV Fia 3000Document6 pagesCatalogue HV Fia 3000Matheus NovaesNo ratings yet
- Drug CounsellingDocument4 pagesDrug CounsellingAnkit PandeyNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Gonadal Hormone Cology - GPAT - 25367565Document48 pagesGonadal Hormone Cology - GPAT - 25367565manjitplk3No ratings yet
- AdrenalineDocument11 pagesAdrenalineAli AkhtarNo ratings yet
- CC 2 - ElecDocument4 pagesCC 2 - Elecjohnjoseph.ermitanoNo ratings yet
- Fertilidad SEMECEDocument14 pagesFertilidad SEMECEArnoldo FelixNo ratings yet
- Triage: Severe Pneumonia Ards Sepsis Septic ShockDocument1 pageTriage: Severe Pneumonia Ards Sepsis Septic ShockRajagopal ReddyNo ratings yet
- Amilasa BEIS37 SPINREACTDocument2 pagesAmilasa BEIS37 SPINREACTMishell YajairaNo ratings yet
- Succunylcholine (Anectine) : University of San Carlos College of Nursing Drug StudyDocument1 pageSuccunylcholine (Anectine) : University of San Carlos College of Nursing Drug StudyFederico AndalesNo ratings yet
- Pocket Notes - CompressedDocument93 pagesPocket Notes - CompressedRey NhlNo ratings yet
- Anti Cancer DrugsDocument4 pagesAnti Cancer Drugsnerdo1999No ratings yet
- (Local Anaesthetics) : Dr. MizajDocument17 pages(Local Anaesthetics) : Dr. MizajaliNo ratings yet
- 038 AnaphylaxisDocument5 pages038 AnaphylaxisabbuahmedibbuNo ratings yet
- HPT DDX (Sarah)Document3 pagesHPT DDX (Sarah)Maisarah RepinNo ratings yet
- Erba ALBUMIN PDFDocument2 pagesErba ALBUMIN PDFAniket dubeyNo ratings yet
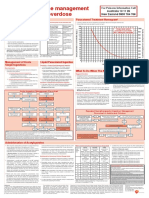
- Paracetamol OD Poster 2016 VersionDocument1 pageParacetamol OD Poster 2016 Versionmuhamed bwamkuuNo ratings yet
- Adrenal GlandsDocument7 pagesAdrenal Glands8wgmhh9ks9No ratings yet
- Peri-Arrest ArrythmiaDocument14 pagesPeri-Arrest Arrythmiamohamed mowafeyNo ratings yet
- College of Allied Health Studies: Bachelor of Science in NursingDocument10 pagesCollege of Allied Health Studies: Bachelor of Science in NursingPatricia FaraonNo ratings yet
- Sample Safety Health and Environmental ManualDocument13 pagesSample Safety Health and Environmental Manualtony s100% (1)
- Isosorbide Dinitrate Sublingual TabletsDocument9 pagesIsosorbide Dinitrate Sublingual TabletsGatot WidyatmoNo ratings yet
- The Accuracy of The Edinburgh Red Eye Diagnostic Algorithm: H Timlin, L Butler and M WrightDocument15 pagesThe Accuracy of The Edinburgh Red Eye Diagnostic Algorithm: H Timlin, L Butler and M WrightKuntya SarettaNo ratings yet
- Psychological Resilience Hope and Adaptability As Protective Factors in Times of Crisis A Study in Greek and Cypriot Society During The Covid 19 Pandemic 'PDF'Document15 pagesPsychological Resilience Hope and Adaptability As Protective Factors in Times of Crisis A Study in Greek and Cypriot Society During The Covid 19 Pandemic 'PDF'Demetris HadjicharalambousNo ratings yet
- Almaghrabi Resp ExaminationDocument33 pagesAlmaghrabi Resp ExaminationSagit Nauman81No ratings yet
- Communication Skills Training For Health Professionals PDFDocument2 pagesCommunication Skills Training For Health Professionals PDFMaggieNo ratings yet
- 55 - Draft Ordinance No. 14 - Support To PWDDocument2 pages55 - Draft Ordinance No. 14 - Support To PWDJun OrbitaNo ratings yet
- Respiratory Disorders and PregnancyDocument23 pagesRespiratory Disorders and PregnancyAngelie RojasNo ratings yet
- Radzyk, J.J. - s1171984 (Verslag)Document54 pagesRadzyk, J.J. - s1171984 (Verslag)Ambreen AANo ratings yet
- Ecd 735 Professional Disclosure Statement Supervision 9 2015 For SiteDocument4 pagesEcd 735 Professional Disclosure Statement Supervision 9 2015 For Siteapi-314123316No ratings yet
- Nursing Management of AggressionDocument7 pagesNursing Management of AggressionMark Guerrero Jabonitalla100% (2)
- Diabetes in Elderly Adults: Graydon S. Meneilly and Daniel TessierDocument9 pagesDiabetes in Elderly Adults: Graydon S. Meneilly and Daniel Tessierdita prameswariNo ratings yet
- In Primary Care: Chronic Kidney Disease (CKD)Document4 pagesIn Primary Care: Chronic Kidney Disease (CKD)NotForAbuseNo ratings yet
- Competition Ratios 2019 - 1Document4 pagesCompetition Ratios 2019 - 1Dr Shawgat Ul Karim KhanNo ratings yet
- Breast Cancer Diagnosed During PregnancyDocument3 pagesBreast Cancer Diagnosed During PregnancyJonny CardenasNo ratings yet
- Sensory Processing DisorderDocument9 pagesSensory Processing Disorderapi-360330020No ratings yet
- Epilepsy in PregnancyDocument20 pagesEpilepsy in Pregnancytenri olaNo ratings yet
- Ateneo de Zamboanga University: Case Study (HOSPITAL)Document7 pagesAteneo de Zamboanga University: Case Study (HOSPITAL)Lyka SaysonNo ratings yet
- Sec31 250Document14 pagesSec31 250Richie DalyNo ratings yet
- Acute Appendicitis: Introduction: Chronic Appendicitis Chronic AppendicitisDocument7 pagesAcute Appendicitis: Introduction: Chronic Appendicitis Chronic AppendicitisCherry Lyn Pugal MarcosNo ratings yet
- Funda Basic Care and ComfortDocument11 pagesFunda Basic Care and Comfortjericho obiceNo ratings yet
- Thời gian: 180 phút (không kể thời gian giao đề) : Page 1 of 15Document15 pagesThời gian: 180 phút (không kể thời gian giao đề) : Page 1 of 15Quốc Duy ĐỗNo ratings yet
- Tratment of The Plaque-Induced GingivitisDocument10 pagesTratment of The Plaque-Induced GingivitisPragita Ayu SaputriNo ratings yet