
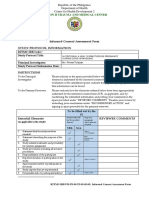
PRE-REC-FO-010 Informed Consent Form (ICF) Checklist
PRE-REC-FO-010 Informed Consent Form (ICF) Checklist
You might also like
- Cnu-Rec-Forms-Margaritta Hermoso - GroupDocument18 pagesCnu-Rec-Forms-Margaritta Hermoso - GroupMichael Clyde lepasana100% (1)
- Sample Non Disclosure AgreementDocument4 pagesSample Non Disclosure AgreementMasauso BandaNo ratings yet
- FDA BIMO ChecklistDocument25 pagesFDA BIMO Checklistnasim50% (2)
- Sales Consultant AgreementDocument6 pagesSales Consultant AgreementeliasNo ratings yet
- CEU IERB Form 14.0 (2020) Informed ConseDocument7 pagesCEU IERB Form 14.0 (2020) Informed ConseMarian CrisolNo ratings yet
- Elements of Informed Consent - Lu PaiDocument31 pagesElements of Informed Consent - Lu PaiAl YsSa Ricafort Millabas100% (1)
- Full Ethics Approval Form (New)Document7 pagesFull Ethics Approval Form (New)Jackson Chua0% (1)
- ETHICS Application, Consent, Debrief, Participant Data Privacy Notice STORAGE (Sept 2019 CD LW 250919)Document14 pagesETHICS Application, Consent, Debrief, Participant Data Privacy Notice STORAGE (Sept 2019 CD LW 250919)floriNo ratings yet
- Template 4 Ethics Review Form DIASS RubricsDocument2 pagesTemplate 4 Ethics Review Form DIASS RubricsJeff Loang100% (1)
- PRE-REC-FO-009 Protocol Review Assessment FormDocument3 pagesPRE-REC-FO-009 Protocol Review Assessment FormMary Ann SantosNo ratings yet
- LDCUREB FORM 2D Informed Consent Assessment FormDocument4 pagesLDCUREB FORM 2D Informed Consent Assessment FormHareen “areshapesgay-” AdlaonNo ratings yet
- Erc Form 2 e Informed Consent Assessment v2-0Document4 pagesErc Form 2 e Informed Consent Assessment v2-0StenoNo ratings yet
- URERB Form 8 Informed Consent Assessment Form REVISEDDocument2 pagesURERB Form 8 Informed Consent Assessment Form REVISEDShane Pearl Lae Sales-EspañolNo ratings yet
- Informed Consent Assessment Form Study Protocol Information: Region Ii Trauma and Medical CenterDocument4 pagesInformed Consent Assessment Form Study Protocol Information: Region Ii Trauma and Medical CenterJM RomiasNo ratings yet
- UPMREB FORM 2 (D) 2012 Informed Consent Assessment FormDocument6 pagesUPMREB FORM 2 (D) 2012 Informed Consent Assessment FormMJ VergaraNo ratings yet
- Informed Consent Assessment FormDocument3 pagesInformed Consent Assessment FormDADYALLA, Raspreet KaurNo ratings yet
- ERCf9 Informed ConsentDocument3 pagesERCf9 Informed ConsentERNEST GABRIEL ADVINCULANo ratings yet
- SOP-QA-9 V5 Receiving Informed ConsentDocument4 pagesSOP-QA-9 V5 Receiving Informed ConsentOlja PopovicNo ratings yet
- SOP Number Insert Number SOP Title: Informed ConsentDocument5 pagesSOP Number Insert Number SOP Title: Informed Consentdiana.alyNo ratings yet
- REC Form 2.4 Informed Consent Assent Evalution FormDocument4 pagesREC Form 2.4 Informed Consent Assent Evalution FormDim PleNo ratings yet
- Sop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentDocument12 pagesSop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentMadhan MohanNo ratings yet
- Human Research Protection Program Informed Consent ProcessDocument6 pagesHuman Research Protection Program Informed Consent ProcessNurul KurniawatiNo ratings yet
- DocumentsDocument7 pagesDocumentsanjali sruthyNo ratings yet
- Acaddemic Work Role Conflict and Balance Among Employed Students of HNU ERB PACKET - EDITIONDocument23 pagesAcaddemic Work Role Conflict and Balance Among Employed Students of HNU ERB PACKET - EDITIONanthonymatthew.nemenzoNo ratings yet
- BIMO Site Audit Check List 8nov11Document8 pagesBIMO Site Audit Check List 8nov11Martijn Van MechelenNo ratings yet
- Informed Consent Assessment Form (UPMREB)Document3 pagesInformed Consent Assessment Form (UPMREB)Joanna CaytonNo ratings yet
- CEU IERB Form 14.0 2021 Informed Consent Assessment Form 2Document7 pagesCEU IERB Form 14.0 2021 Informed Consent Assessment Form 2Alyahanna Sta. MariaNo ratings yet
- Screening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument6 pagesScreening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityAlberio CygnusNo ratings yet
- UPMREB FORM 2 (D) 2012 Informed Consent Assessment Form - 1Document4 pagesUPMREB FORM 2 (D) 2012 Informed Consent Assessment Form - 1mariajorjeNo ratings yet
- Essential Documents For The Conduct of A Clinical TrialDocument10 pagesEssential Documents For The Conduct of A Clinical TrialSandeep SinghalNo ratings yet
- Site Start Up and Maintainence PowerpointDocument6 pagesSite Start Up and Maintainence PowerpointNeha DungNo ratings yet
- Rec FinalDocument10 pagesRec FinalapryllrocksNo ratings yet
- New Ethical Review Submission FormDocument9 pagesNew Ethical Review Submission FormKeshya Maleeza WeerakkodyNo ratings yet
- Monitoring of Clinical StudiesDocument9 pagesMonitoring of Clinical StudiesMostafa SalahNo ratings yet
- Xx/Mmm/Yyyy: Guidance Resource - For Use As An Example Only Adapted From The MTNDocument6 pagesXx/Mmm/Yyyy: Guidance Resource - For Use As An Example Only Adapted From The MTNdiana.alyNo ratings yet
- Site Monitoring Plan TemplateDocument5 pagesSite Monitoring Plan TemplaterajuNo ratings yet
- RTS - Informed Consent Assessment Form UpdatedDocument4 pagesRTS - Informed Consent Assessment Form UpdatedKhristine CocsonNo ratings yet
- Apu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Document4 pagesApu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8shaedowNo ratings yet
- SOPDocument5 pagesSOPJaime HinojosaNo ratings yet
- Apu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Document4 pagesApu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Parvinder McCartneyNo ratings yet
- 3-Informed-Consent-Assessment-Form Filled Out Not CompleteDocument7 pages3-Informed-Consent-Assessment-Form Filled Out Not CompleteARGELINE JOY AMORESNo ratings yet
- Legco Observation RecordDocument4 pagesLegco Observation Recordapi-302215319No ratings yet
- Student's GuideDocument3 pagesStudent's GuideGODWIN VILLANUEVANo ratings yet
- Monitoring Plan 4 WebsiteDocument5 pagesMonitoring Plan 4 WebsitejohncuyNo ratings yet
- Assessment ToolDocument18 pagesAssessment Toolsheila marie canibasNo ratings yet
- Uvirb Form Iid2 Informed Consent Assessment Form1Document6 pagesUvirb Form Iid2 Informed Consent Assessment Form1api-222431624No ratings yet
- Format For Informed Consent FormsDocument14 pagesFormat For Informed Consent FormsErikha ChairilNo ratings yet
- Site Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument4 pagesSite Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State Universityna sarvaNo ratings yet
- Legco Observation RecordDocument4 pagesLegco Observation Recordapi-263399420No ratings yet
- Standard Operating Procedure Trial Master File and 421 Main Evidence in TheDocument33 pagesStandard Operating Procedure Trial Master File and 421 Main Evidence in Theahmed.bouchenakNo ratings yet
- Philippine Framework For Assurance EngagementDocument5 pagesPhilippine Framework For Assurance EngagementKrizel rochaNo ratings yet
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 pagesSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- General Guidelines (Version-3.0)Document3 pagesGeneral Guidelines (Version-3.0)revanth kallaNo ratings yet
- Sop 602 FdaauditsDocument4 pagesSop 602 FdaauditsqualidadeNo ratings yet
- Master of Advanced Health Care Practice: Professional PortfolioDocument7 pagesMaster of Advanced Health Care Practice: Professional PortfolioAnisah Tifani MaulidyantiNo ratings yet
- External Audits and Inspections May 1 2019Document4 pagesExternal Audits and Inspections May 1 2019Takada NamaNo ratings yet
- Monitoring Plan and Standard Operating Procedure: Protocol TitleDocument5 pagesMonitoring Plan and Standard Operating Procedure: Protocol TitleDipeshNo ratings yet
- MTN - IoR Training - Slides Notes - FINAL - 06.30.16Document64 pagesMTN - IoR Training - Slides Notes - FINAL - 06.30.16luamsmarinsNo ratings yet
- Clinical Trial Registration and Application FormDocument3 pagesClinical Trial Registration and Application FormJerilee Grantoza100% (1)
- Legco Observation RecordDocument6 pagesLegco Observation Recordapi-248093224No ratings yet
- Informed ConsentDocument8 pagesInformed ConsentAlexandra Nadinne100% (1)
- Food Control System Assessment Tool: Dimension D – Science/Knowledge Base and Continuous ImprovementFrom EverandFood Control System Assessment Tool: Dimension D – Science/Knowledge Base and Continuous ImprovementNo ratings yet
- PRE-REC-FO-008 Research Protocol Application FormDocument1 pagePRE-REC-FO-008 Research Protocol Application FormMary Ann SantosNo ratings yet
- PRE REC FO 012 Submission ChecklistDocument1 pagePRE REC FO 012 Submission ChecklistMary Ann SantosNo ratings yet
- PRE REC FO 011 Detailed Budget SheetDocument1 pagePRE REC FO 011 Detailed Budget SheetMary Ann SantosNo ratings yet
- PRE-REC-FO-009 Protocol Review Assessment FormDocument3 pagesPRE-REC-FO-009 Protocol Review Assessment FormMary Ann SantosNo ratings yet
- Confidentiality ClauseDocument3 pagesConfidentiality Clausedrex silvinoNo ratings yet
- International Observership Form KansascityDocument12 pagesInternational Observership Form Kansascityসোমনাথ মহাপাত্রNo ratings yet
- Read The Latest Reports From Florida Coalition Against Domestic ViolenceDocument113 pagesRead The Latest Reports From Florida Coalition Against Domestic ViolencestprepsNo ratings yet
- 36898-IUBT309 Unit Specification v1Document6 pages36898-IUBT309 Unit Specification v1irtantikaNo ratings yet
- NHCP Guidelines PDFDocument15 pagesNHCP Guidelines PDFSuraj MandalNo ratings yet
- Legal EthicsDocument4 pagesLegal EthicsBannylyn Mae Silaroy GamitNo ratings yet
- Riverbook ContractDocument4 pagesRiverbook Contractyeabsira gashawNo ratings yet
- 500 Word Essay CarlDocument1 page500 Word Essay CarlCarl M. CubarolNo ratings yet
- 339 MPHEL729 NorthBristolJDFINAL PAEDIATRICANDPERINATALPATHOLOGIST PDFDocument24 pages339 MPHEL729 NorthBristolJDFINAL PAEDIATRICANDPERINATALPATHOLOGIST PDFMD Luthfy LubisNo ratings yet
- Business Ethics PolicyDocument9 pagesBusiness Ethics Policyjohnmark00947No ratings yet
- Shubhadeep DeyDocument9 pagesShubhadeep DeyMon PagolNo ratings yet
- 43 Secrets ToolkitDocument207 pages43 Secrets Toolkitsundevil2010usa4605No ratings yet
- Final Pre Accreditation Entry Level Standards For SHCO Book1Document50 pagesFinal Pre Accreditation Entry Level Standards For SHCO Book1Javed KhanNo ratings yet
- Non Compete SignedDocument12 pagesNon Compete SignedfhrtechNo ratings yet
- Alorica WAH Expectations Supplement RJBDocument3 pagesAlorica WAH Expectations Supplement RJByepNo ratings yet
- Standards of ConductDocument3 pagesStandards of ConductNews 8 WROCNo ratings yet
- Documenting and Reporting LEARNING OUTCOMES After Completing This ChapterDocument29 pagesDocumenting and Reporting LEARNING OUTCOMES After Completing This Chaptertwy113No ratings yet
- Personnel Policies and Practices in Early ChildhoodDocument8 pagesPersonnel Policies and Practices in Early ChildhoodcarechildNo ratings yet
- RA 8552 - Domestic Adoption ActDocument12 pagesRA 8552 - Domestic Adoption ActGerry Payno100% (1)
- Receive VisitorsDocument7 pagesReceive Visitorsrenni16No ratings yet
- Sify Total Lifecycle Channel Partner Agreement FY 2017-20 July17Document18 pagesSify Total Lifecycle Channel Partner Agreement FY 2017-20 July17Genesis Pvt LtdNo ratings yet
- PRICING STRATEGY OF Zara 1 (Recovered)Document41 pagesPRICING STRATEGY OF Zara 1 (Recovered)Twinkle vermaNo ratings yet
- Employee Code of Conduct - Islamic SchoolsDocument2 pagesEmployee Code of Conduct - Islamic SchoolsSajjad M ShafiNo ratings yet
- Intellectual Property - OutlineDocument47 pagesIntellectual Property - Outlinesnicklefritz1865100% (1)
- HtsDocument5 pagesHtsMouliNo ratings yet
- 2016 12 19 PAGA Complaint Against GoogleDocument24 pages2016 12 19 PAGA Complaint Against GoogleZerohedgeNo ratings yet
- P1018 Fraud Report Form 290609Document9 pagesP1018 Fraud Report Form 290609yyeeaaboiNo ratings yet
- Code of EthicsDocument5 pagesCode of Ethicsapi-316470548No ratings yet


























































































Download as docx, pdf, or txt
You might also like
- Cnu-Rec-Forms-Margaritta Hermoso - GroupDocument18 pagesCnu-Rec-Forms-Margaritta Hermoso - GroupMichael Clyde lepasana100% (1)
- Sample Non Disclosure AgreementDocument4 pagesSample Non Disclosure AgreementMasauso BandaNo ratings yet
- FDA BIMO ChecklistDocument25 pagesFDA BIMO Checklistnasim50% (2)
- Sales Consultant AgreementDocument6 pagesSales Consultant AgreementeliasNo ratings yet
- CEU IERB Form 14.0 (2020) Informed ConseDocument7 pagesCEU IERB Form 14.0 (2020) Informed ConseMarian CrisolNo ratings yet
- Elements of Informed Consent - Lu PaiDocument31 pagesElements of Informed Consent - Lu PaiAl YsSa Ricafort Millabas100% (1)
- Full Ethics Approval Form (New)Document7 pagesFull Ethics Approval Form (New)Jackson Chua0% (1)
- ETHICS Application, Consent, Debrief, Participant Data Privacy Notice STORAGE (Sept 2019 CD LW 250919)Document14 pagesETHICS Application, Consent, Debrief, Participant Data Privacy Notice STORAGE (Sept 2019 CD LW 250919)floriNo ratings yet
- Template 4 Ethics Review Form DIASS RubricsDocument2 pagesTemplate 4 Ethics Review Form DIASS RubricsJeff Loang100% (1)
- PRE-REC-FO-009 Protocol Review Assessment FormDocument3 pagesPRE-REC-FO-009 Protocol Review Assessment FormMary Ann SantosNo ratings yet
- LDCUREB FORM 2D Informed Consent Assessment FormDocument4 pagesLDCUREB FORM 2D Informed Consent Assessment FormHareen “areshapesgay-” AdlaonNo ratings yet
- Erc Form 2 e Informed Consent Assessment v2-0Document4 pagesErc Form 2 e Informed Consent Assessment v2-0StenoNo ratings yet
- URERB Form 8 Informed Consent Assessment Form REVISEDDocument2 pagesURERB Form 8 Informed Consent Assessment Form REVISEDShane Pearl Lae Sales-EspañolNo ratings yet
- Informed Consent Assessment Form Study Protocol Information: Region Ii Trauma and Medical CenterDocument4 pagesInformed Consent Assessment Form Study Protocol Information: Region Ii Trauma and Medical CenterJM RomiasNo ratings yet
- UPMREB FORM 2 (D) 2012 Informed Consent Assessment FormDocument6 pagesUPMREB FORM 2 (D) 2012 Informed Consent Assessment FormMJ VergaraNo ratings yet
- Informed Consent Assessment FormDocument3 pagesInformed Consent Assessment FormDADYALLA, Raspreet KaurNo ratings yet
- ERCf9 Informed ConsentDocument3 pagesERCf9 Informed ConsentERNEST GABRIEL ADVINCULANo ratings yet
- SOP-QA-9 V5 Receiving Informed ConsentDocument4 pagesSOP-QA-9 V5 Receiving Informed ConsentOlja PopovicNo ratings yet
- SOP Number Insert Number SOP Title: Informed ConsentDocument5 pagesSOP Number Insert Number SOP Title: Informed Consentdiana.alyNo ratings yet
- REC Form 2.4 Informed Consent Assent Evalution FormDocument4 pagesREC Form 2.4 Informed Consent Assent Evalution FormDim PleNo ratings yet
- Sop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentDocument12 pagesSop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentMadhan MohanNo ratings yet
- Human Research Protection Program Informed Consent ProcessDocument6 pagesHuman Research Protection Program Informed Consent ProcessNurul KurniawatiNo ratings yet
- DocumentsDocument7 pagesDocumentsanjali sruthyNo ratings yet
- Acaddemic Work Role Conflict and Balance Among Employed Students of HNU ERB PACKET - EDITIONDocument23 pagesAcaddemic Work Role Conflict and Balance Among Employed Students of HNU ERB PACKET - EDITIONanthonymatthew.nemenzoNo ratings yet
- BIMO Site Audit Check List 8nov11Document8 pagesBIMO Site Audit Check List 8nov11Martijn Van MechelenNo ratings yet
- Informed Consent Assessment Form (UPMREB)Document3 pagesInformed Consent Assessment Form (UPMREB)Joanna CaytonNo ratings yet
- CEU IERB Form 14.0 2021 Informed Consent Assessment Form 2Document7 pagesCEU IERB Form 14.0 2021 Informed Consent Assessment Form 2Alyahanna Sta. MariaNo ratings yet
- Screening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument6 pagesScreening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityAlberio CygnusNo ratings yet
- UPMREB FORM 2 (D) 2012 Informed Consent Assessment Form - 1Document4 pagesUPMREB FORM 2 (D) 2012 Informed Consent Assessment Form - 1mariajorjeNo ratings yet
- Essential Documents For The Conduct of A Clinical TrialDocument10 pagesEssential Documents For The Conduct of A Clinical TrialSandeep SinghalNo ratings yet
- Site Start Up and Maintainence PowerpointDocument6 pagesSite Start Up and Maintainence PowerpointNeha DungNo ratings yet
- Rec FinalDocument10 pagesRec FinalapryllrocksNo ratings yet
- New Ethical Review Submission FormDocument9 pagesNew Ethical Review Submission FormKeshya Maleeza WeerakkodyNo ratings yet
- Monitoring of Clinical StudiesDocument9 pagesMonitoring of Clinical StudiesMostafa SalahNo ratings yet
- Xx/Mmm/Yyyy: Guidance Resource - For Use As An Example Only Adapted From The MTNDocument6 pagesXx/Mmm/Yyyy: Guidance Resource - For Use As An Example Only Adapted From The MTNdiana.alyNo ratings yet
- Site Monitoring Plan TemplateDocument5 pagesSite Monitoring Plan TemplaterajuNo ratings yet
- RTS - Informed Consent Assessment Form UpdatedDocument4 pagesRTS - Informed Consent Assessment Form UpdatedKhristine CocsonNo ratings yet
- Apu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Document4 pagesApu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8shaedowNo ratings yet
- SOPDocument5 pagesSOPJaime HinojosaNo ratings yet
- Apu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Document4 pagesApu / Apiit Fast-Track Ethical Approval Form (Students) : YES NO N/A 1 2 3 4 5 6 7 8Parvinder McCartneyNo ratings yet
- 3-Informed-Consent-Assessment-Form Filled Out Not CompleteDocument7 pages3-Informed-Consent-Assessment-Form Filled Out Not CompleteARGELINE JOY AMORESNo ratings yet
- Legco Observation RecordDocument4 pagesLegco Observation Recordapi-302215319No ratings yet
- Student's GuideDocument3 pagesStudent's GuideGODWIN VILLANUEVANo ratings yet
- Monitoring Plan 4 WebsiteDocument5 pagesMonitoring Plan 4 WebsitejohncuyNo ratings yet
- Assessment ToolDocument18 pagesAssessment Toolsheila marie canibasNo ratings yet
- Uvirb Form Iid2 Informed Consent Assessment Form1Document6 pagesUvirb Form Iid2 Informed Consent Assessment Form1api-222431624No ratings yet
- Format For Informed Consent FormsDocument14 pagesFormat For Informed Consent FormsErikha ChairilNo ratings yet
- Site Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument4 pagesSite Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State Universityna sarvaNo ratings yet
- Legco Observation RecordDocument4 pagesLegco Observation Recordapi-263399420No ratings yet
- Standard Operating Procedure Trial Master File and 421 Main Evidence in TheDocument33 pagesStandard Operating Procedure Trial Master File and 421 Main Evidence in Theahmed.bouchenakNo ratings yet
- Philippine Framework For Assurance EngagementDocument5 pagesPhilippine Framework For Assurance EngagementKrizel rochaNo ratings yet
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 pagesSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- General Guidelines (Version-3.0)Document3 pagesGeneral Guidelines (Version-3.0)revanth kallaNo ratings yet
- Sop 602 FdaauditsDocument4 pagesSop 602 FdaauditsqualidadeNo ratings yet
- Master of Advanced Health Care Practice: Professional PortfolioDocument7 pagesMaster of Advanced Health Care Practice: Professional PortfolioAnisah Tifani MaulidyantiNo ratings yet
- External Audits and Inspections May 1 2019Document4 pagesExternal Audits and Inspections May 1 2019Takada NamaNo ratings yet
- Monitoring Plan and Standard Operating Procedure: Protocol TitleDocument5 pagesMonitoring Plan and Standard Operating Procedure: Protocol TitleDipeshNo ratings yet
- MTN - IoR Training - Slides Notes - FINAL - 06.30.16Document64 pagesMTN - IoR Training - Slides Notes - FINAL - 06.30.16luamsmarinsNo ratings yet
- Clinical Trial Registration and Application FormDocument3 pagesClinical Trial Registration and Application FormJerilee Grantoza100% (1)
- Legco Observation RecordDocument6 pagesLegco Observation Recordapi-248093224No ratings yet
- Informed ConsentDocument8 pagesInformed ConsentAlexandra Nadinne100% (1)
- Food Control System Assessment Tool: Dimension D – Science/Knowledge Base and Continuous ImprovementFrom EverandFood Control System Assessment Tool: Dimension D – Science/Knowledge Base and Continuous ImprovementNo ratings yet
- PRE-REC-FO-008 Research Protocol Application FormDocument1 pagePRE-REC-FO-008 Research Protocol Application FormMary Ann SantosNo ratings yet
- PRE REC FO 012 Submission ChecklistDocument1 pagePRE REC FO 012 Submission ChecklistMary Ann SantosNo ratings yet
- PRE REC FO 011 Detailed Budget SheetDocument1 pagePRE REC FO 011 Detailed Budget SheetMary Ann SantosNo ratings yet
- PRE-REC-FO-009 Protocol Review Assessment FormDocument3 pagesPRE-REC-FO-009 Protocol Review Assessment FormMary Ann SantosNo ratings yet
- Confidentiality ClauseDocument3 pagesConfidentiality Clausedrex silvinoNo ratings yet
- International Observership Form KansascityDocument12 pagesInternational Observership Form Kansascityসোমনাথ মহাপাত্রNo ratings yet
- Read The Latest Reports From Florida Coalition Against Domestic ViolenceDocument113 pagesRead The Latest Reports From Florida Coalition Against Domestic ViolencestprepsNo ratings yet
- 36898-IUBT309 Unit Specification v1Document6 pages36898-IUBT309 Unit Specification v1irtantikaNo ratings yet
- NHCP Guidelines PDFDocument15 pagesNHCP Guidelines PDFSuraj MandalNo ratings yet
- Legal EthicsDocument4 pagesLegal EthicsBannylyn Mae Silaroy GamitNo ratings yet
- Riverbook ContractDocument4 pagesRiverbook Contractyeabsira gashawNo ratings yet
- 500 Word Essay CarlDocument1 page500 Word Essay CarlCarl M. CubarolNo ratings yet
- 339 MPHEL729 NorthBristolJDFINAL PAEDIATRICANDPERINATALPATHOLOGIST PDFDocument24 pages339 MPHEL729 NorthBristolJDFINAL PAEDIATRICANDPERINATALPATHOLOGIST PDFMD Luthfy LubisNo ratings yet
- Business Ethics PolicyDocument9 pagesBusiness Ethics Policyjohnmark00947No ratings yet
- Shubhadeep DeyDocument9 pagesShubhadeep DeyMon PagolNo ratings yet
- 43 Secrets ToolkitDocument207 pages43 Secrets Toolkitsundevil2010usa4605No ratings yet
- Final Pre Accreditation Entry Level Standards For SHCO Book1Document50 pagesFinal Pre Accreditation Entry Level Standards For SHCO Book1Javed KhanNo ratings yet
- Non Compete SignedDocument12 pagesNon Compete SignedfhrtechNo ratings yet
- Alorica WAH Expectations Supplement RJBDocument3 pagesAlorica WAH Expectations Supplement RJByepNo ratings yet
- Standards of ConductDocument3 pagesStandards of ConductNews 8 WROCNo ratings yet
- Documenting and Reporting LEARNING OUTCOMES After Completing This ChapterDocument29 pagesDocumenting and Reporting LEARNING OUTCOMES After Completing This Chaptertwy113No ratings yet
- Personnel Policies and Practices in Early ChildhoodDocument8 pagesPersonnel Policies and Practices in Early ChildhoodcarechildNo ratings yet
- RA 8552 - Domestic Adoption ActDocument12 pagesRA 8552 - Domestic Adoption ActGerry Payno100% (1)
- Receive VisitorsDocument7 pagesReceive Visitorsrenni16No ratings yet
- Sify Total Lifecycle Channel Partner Agreement FY 2017-20 July17Document18 pagesSify Total Lifecycle Channel Partner Agreement FY 2017-20 July17Genesis Pvt LtdNo ratings yet
- PRICING STRATEGY OF Zara 1 (Recovered)Document41 pagesPRICING STRATEGY OF Zara 1 (Recovered)Twinkle vermaNo ratings yet
- Employee Code of Conduct - Islamic SchoolsDocument2 pagesEmployee Code of Conduct - Islamic SchoolsSajjad M ShafiNo ratings yet
- Intellectual Property - OutlineDocument47 pagesIntellectual Property - Outlinesnicklefritz1865100% (1)
- HtsDocument5 pagesHtsMouliNo ratings yet
- 2016 12 19 PAGA Complaint Against GoogleDocument24 pages2016 12 19 PAGA Complaint Against GoogleZerohedgeNo ratings yet
- P1018 Fraud Report Form 290609Document9 pagesP1018 Fraud Report Form 290609yyeeaaboiNo ratings yet
- Code of EthicsDocument5 pagesCode of Ethicsapi-316470548No ratings yet