Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mark Minervini Stage 2 Uptrend and Trend TemplateDocument1 pageMark Minervini Stage 2 Uptrend and Trend TemplateL100% (1)
- From Wikipedia, The Free Encyclopedia: Irrational Exuberance, 2d EdDocument1 pageFrom Wikipedia, The Free Encyclopedia: Irrational Exuberance, 2d EdLNo ratings yet
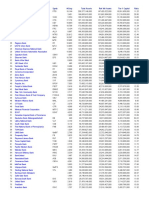
- Tier 1 Capital - All Banks1Document1 pageTier 1 Capital - All Banks1LNo ratings yet
- Tier 1 Capital - All BanksDocument1 pageTier 1 Capital - All BanksLNo ratings yet
- Hat-Trick-3 Easy-Entry-Exit Strategies9Document1 pageHat-Trick-3 Easy-Entry-Exit Strategies9LNo ratings yet
- 101 Things Everyone Should Know About Economics 1Document1 page101 Things Everyone Should Know About Economics 1LNo ratings yet
- Tier 1 Capital - All BanksDocument3 pagesTier 1 Capital - All BanksL100% (1)
- Hat-Trick-3 Easy-Entry-Exit Strategies8Document1 pageHat-Trick-3 Easy-Entry-Exit Strategies8LNo ratings yet
- What Is An ATR Trailing Stop?: New Trader UDocument1 pageWhat Is An ATR Trailing Stop?: New Trader ULNo ratings yet
- Hat-Trick-3 Easy-Entry-Exit Strategies6Document1 pageHat-Trick-3 Easy-Entry-Exit Strategies6LNo ratings yet
- ATR Trailing Stop2Document1 pageATR Trailing Stop2LNo ratings yet
- Guide For Officer and AdvisersDocument58 pagesGuide For Officer and AdvisersLane RandallNo ratings yet
- Toyota Prius Research PaperDocument6 pagesToyota Prius Research Paperzgkuqhxgf100% (1)
- Escalation and Price Indices ESB 450Document31 pagesEscalation and Price Indices ESB 450sarcozy922No ratings yet
- SQL Top 50 Interview Questions and AnswersDocument28 pagesSQL Top 50 Interview Questions and AnswersBiplab SarkarNo ratings yet
- 18 PCIR Action PlansDocument48 pages18 PCIR Action PlansJohanne Rhielle OpridoNo ratings yet
- BCPCDocument2 pagesBCPCBARANGAY BANGGOT BANGGOTNo ratings yet
- Internship Report - Nguyễn Trần Phương ThảoDocument25 pagesInternship Report - Nguyễn Trần Phương ThảoThảo PhươngNo ratings yet
- Subject: ICAO & FAA Airfield Rescue and Fire Fighting Categories For Airbus AircraftDocument2 pagesSubject: ICAO & FAA Airfield Rescue and Fire Fighting Categories For Airbus AircraftAon ThummachaiNo ratings yet
- Mtoa TutorialsDocument214 pagesMtoa Tutorials123batutaNo ratings yet
- MT-010-005 MSA Arva - Navan 110 KV Existing StructuresDocument1 pageMT-010-005 MSA Arva - Navan 110 KV Existing StructuresWeber HahnNo ratings yet
- Huawei CommandsDocument2 pagesHuawei CommandsRade Pralica100% (1)
- Abrasive Technical Data SheetDocument2 pagesAbrasive Technical Data SheetZaid Raslan AyoubNo ratings yet
- Freedom Constitution and The 1987 ConstitutionDocument9 pagesFreedom Constitution and The 1987 ConstitutionWearIt Co.100% (1)
- Metu-Mete-Phd Theses Since 1971 PDFDocument5 pagesMetu-Mete-Phd Theses Since 1971 PDFsiaeatoomNo ratings yet
- On Site Engineering - CompressedDocument12 pagesOn Site Engineering - CompressedanthonythiaNo ratings yet
- Design of Concrete Ring Type Foundation For Storage TankDocument6 pagesDesign of Concrete Ring Type Foundation For Storage TankNabil Al-KhirdajiNo ratings yet
- Databases and Applications ProgramsDocument7 pagesDatabases and Applications ProgramsShibinMohammedIqbalNo ratings yet
- Tugas Case Red Bull - WidyanasariDocument4 pagesTugas Case Red Bull - WidyanasariwdyNo ratings yet
- History of IFRS 7: Reclassification of Financial Assets (Amendments To IAS 39 and IFRS 7) IssuedDocument5 pagesHistory of IFRS 7: Reclassification of Financial Assets (Amendments To IAS 39 and IFRS 7) IssuedTin BatacNo ratings yet
- Impact of Covid-19 Pandemic On The Buying Behavior of Students in A State UniversityDocument30 pagesImpact of Covid-19 Pandemic On The Buying Behavior of Students in A State UniversityCarmelle Callao Dela CernaNo ratings yet
- ErasmusPlus KA2 2021-2027 PartnershipsForCooperationAndExchangesOfPractices Projects Overview 2023-10-03Document1,217 pagesErasmusPlus KA2 2021-2027 PartnershipsForCooperationAndExchangesOfPractices Projects Overview 2023-10-03AyaNo ratings yet
- Overtourism Causes Implications and Solutions 1St Ed Edition Hugues Seraphin Full ChapterDocument67 pagesOvertourism Causes Implications and Solutions 1St Ed Edition Hugues Seraphin Full Chapterevelyn.kennedy635100% (6)
- Measurement Tire Tread Depth Triangularization PDFDocument4 pagesMeasurement Tire Tread Depth Triangularization PDFTrung Hoàng100% (1)
- Rhetorical Analysis EssayDocument2 pagesRhetorical Analysis Essayfemi adeNo ratings yet
- Rainin Pipetting Handbook 17701066 ENDocument78 pagesRainin Pipetting Handbook 17701066 ENLaboratorio Detecto CaliNo ratings yet
- F Flat Pa Anel D Detecto Or: Tech Hnical SP Pecificat TionsDocument2 pagesF Flat Pa Anel D Detecto Or: Tech Hnical SP Pecificat Tionsteten intimedNo ratings yet
- The Electrosynthesis of Organic: CompoundsDocument7 pagesThe Electrosynthesis of Organic: Compoundsmax capetownNo ratings yet
- Vice President Customer Care in Dallas TX Resume Susan RardinDocument2 pagesVice President Customer Care in Dallas TX Resume Susan RardinSusanRardin100% (1)
- MetrologyDocument2 pagesMetrologyMSME Technology CentreNo ratings yet
- Riverside County FY 2020-21 First Quarter Budget ReportDocument50 pagesRiverside County FY 2020-21 First Quarter Budget ReportThe Press-Enterprise / pressenterprise.comNo ratings yet