Download as docx, pdf, or txt
You might also like
- The Hormone Fix: The Natural Way To Balance Your Hormones, Burn Fat and Alleviate The Symptoms of The Perimenopause, The Menopause and Beyond - Anna CabecaDocument5 pagesThe Hormone Fix: The Natural Way To Balance Your Hormones, Burn Fat and Alleviate The Symptoms of The Perimenopause, The Menopause and Beyond - Anna Cabecamonulace14% (7)
- Borax - The Inexpensive Detox, Arthritis, Osteoporosis and Mycoplasma CureDocument10 pagesBorax - The Inexpensive Detox, Arthritis, Osteoporosis and Mycoplasma Cureambertje1283% (6)
- Manejo Miomas 2021Document16 pagesManejo Miomas 2021Laura Daniela MurilloNo ratings yet
- GENERAL CHEMISTRY 2 Module 1Document8 pagesGENERAL CHEMISTRY 2 Module 1Hassel AbayonNo ratings yet
- GENERAL CHEMISTRY 2 Module 1Document8 pagesGENERAL CHEMISTRY 2 Module 1Hassel AbayonNo ratings yet
- Slide PPT Case ReportDocument100 pagesSlide PPT Case ReportLili ManaoNo ratings yet
- Experiencing Transitions: An Emerging Middle-Range TheoryDocument17 pagesExperiencing Transitions: An Emerging Middle-Range TheoryenfhelderNo ratings yet
- Menopause Health QuestionnaireDocument8 pagesMenopause Health QuestionnaireFatma Risda HidayantiNo ratings yet
- MODULE 5 (GEC 1: The Physical and Sexual Self) Lesson 5: The Physical and Sexual SelfDocument20 pagesMODULE 5 (GEC 1: The Physical and Sexual Self) Lesson 5: The Physical and Sexual SelfNovie Viernes100% (1)
- Unpacking The SelfDocument29 pagesUnpacking The SelfRosell SumogatNo ratings yet
- Sexual SelfDocument16 pagesSexual SelfMaripet Maines BagunuNo ratings yet
- Project in UTSDocument30 pagesProject in UTSLorna Edeza EvangelistaNo ratings yet
- Edited UTS Module 5 6Document15 pagesEdited UTS Module 5 6elsa galgaoNo ratings yet
- Understanding The SelfDocument26 pagesUnderstanding The SelfPaula100% (1)
- Psych 101 Lesson 5.1 The Physical and Sexual Self Part 1Document9 pagesPsych 101 Lesson 5.1 The Physical and Sexual Self Part 1Rigel LimaNo ratings yet
- Physical and Sexual Beed 1-bDocument116 pagesPhysical and Sexual Beed 1-brenalyn capulNo ratings yet
- Uts Ch2 Lesson-1Document47 pagesUts Ch2 Lesson-1adrianceneta12No ratings yet
- Lesson 5Document8 pagesLesson 5April ZarsosaNo ratings yet
- Ge 101Document65 pagesGe 101samorales92No ratings yet
- Sex-Education CollegeDocument5 pagesSex-Education CollegeSteffhanie AcunaNo ratings yet
- The Sexual SelfDocument18 pagesThe Sexual SelfAngelo Dale Derramas OndilloNo ratings yet
- THE PHYSICAL AND SEXUAL SELF Part 1Document9 pagesTHE PHYSICAL AND SEXUAL SELF Part 1Ara Minnella MarteNo ratings yet
- MODULEDocument6 pagesMODULEKobe Alcantara ReyesNo ratings yet
- Understanding The Self Module 2 Lesson 1Document18 pagesUnderstanding The Self Module 2 Lesson 1Marites MancerasNo ratings yet
- C2LO1 UTS Physical and Sexual SelfDocument31 pagesC2LO1 UTS Physical and Sexual SelfRuel MillarezNo ratings yet
- The Physical and Sexually SelfDocument8 pagesThe Physical and Sexually SelfAlfred VargasNo ratings yet
- MIDTERM Physical and Sexual Self Part 1Document24 pagesMIDTERM Physical and Sexual Self Part 1earlkevintumulak32No ratings yet
- Group 1Document6 pagesGroup 1alamadadara16No ratings yet
- 11 October UTS Complete VersionDocument43 pages11 October UTS Complete VersionMhar BrandonNo ratings yet
- Sexual SelfDocument13 pagesSexual SelfswitbbgirlNo ratings yet
- Chapter 2 UTS RevDocument11 pagesChapter 2 UTS RevYsabel ApostolNo ratings yet
- (Template) MODULE PART 2 UNPACKING THE SELFDocument14 pages(Template) MODULE PART 2 UNPACKING THE SELFMary Abegail MorandarteNo ratings yet
- Chapter 1 - UtsDocument5 pagesChapter 1 - UtsJeng JengNo ratings yet
- Lesson 5 - The Physical and Sexual Self: Understanding The Self/ Compiled By: Minera Laiza C. Acosta 1Document11 pagesLesson 5 - The Physical and Sexual Self: Understanding The Self/ Compiled By: Minera Laiza C. Acosta 1Daylan Lindo MontefalcoNo ratings yet
- Understanding The SelfDocument29 pagesUnderstanding The SelfBianca Joy Aquino100% (1)
- Module 2Document14 pagesModule 2Marian claire TambalNo ratings yet
- Understanding The Self Chapter 2: Unpacking The Self Miss KZ Ulboc REFERENCE: Cierva, M Chapter 2: Lesson 1 Physical Self: The Beautiful MeDocument5 pagesUnderstanding The Self Chapter 2: Unpacking The Self Miss KZ Ulboc REFERENCE: Cierva, M Chapter 2: Lesson 1 Physical Self: The Beautiful MeKimNo ratings yet
- Understading The Self NotesDocument15 pagesUnderstading The Self NotesdorothyzoeesbietoNo ratings yet
- The Physical and Sexual SelfDocument15 pagesThe Physical and Sexual SelfBrianna ValerioNo ratings yet
- Midterm Understanding The Self ModuleDocument51 pagesMidterm Understanding The Self ModuleMarlon TrinidadNo ratings yet
- Midterm Understanding The Self ModuleDocument53 pagesMidterm Understanding The Self ModuleMarlon TrinidadNo ratings yet
- CHAPTER 2 Lessons 1Document17 pagesCHAPTER 2 Lessons 1Zeo AlcantaraNo ratings yet
- I. The BiologyDocument7 pagesI. The BiologyOffice AcadNo ratings yet
- The Physical and Sexual SelfDocument44 pagesThe Physical and Sexual SelfJudy Mar Cabahug OlivarNo ratings yet
- Chapter II Lesson 1 Lecture HandoutDocument7 pagesChapter II Lesson 1 Lecture HandoutGelay, Lyca L.No ratings yet
- Unpacking The SelfDocument46 pagesUnpacking The SelfBrenda CastilloNo ratings yet
- Chapter 7. The Sexual SelfDocument14 pagesChapter 7. The Sexual SelfdocgioreNo ratings yet
- 1 Ch2 PDFDocument33 pages1 Ch2 PDFJOHNMARK ALMENDRALEJONo ratings yet
- Chapter2 Lesson-1 BSME 1ADocument23 pagesChapter2 Lesson-1 BSME 1AFate GraphiteNo ratings yet
- Psy512 CH 6Document8 pagesPsy512 CH 6mayagee03No ratings yet
- Chapter 7. The Sexual SelfDocument16 pagesChapter 7. The Sexual SelfAna Lorraine BaldozNo ratings yet
- Мужская2Document5 pagesМужская2lkgffjgdlNo ratings yet
- Chapter 2 Unpacking The Self The Sexual SelfDocument3 pagesChapter 2 Unpacking The Self The Sexual SelfcondrillondenmarjohnNo ratings yet
- Biological Differences of Men and Women 1Document281 pagesBiological Differences of Men and Women 1Jed Vincent EsguerraNo ratings yet
- CHAPTERII Lesson 1 The Physical and Sexual Self (GROUP 3)Document56 pagesCHAPTERII Lesson 1 The Physical and Sexual Self (GROUP 3)Brenda CastilloNo ratings yet
- Lesson 5 - Physical and Sexual SelfDocument20 pagesLesson 5 - Physical and Sexual Selfsigma rusNo ratings yet
- Uts Gomez Granada BSMX 2 1Document38 pagesUts Gomez Granada BSMX 2 1PHILLIP KRISTOFFER B. CUIZONNo ratings yet
- UTS - Chapter 2, Lesson 1Document9 pagesUTS - Chapter 2, Lesson 1Krishna Faith P. DelaraNo ratings yet
- LESSON 8: Sexual SelfDocument6 pagesLESSON 8: Sexual SelfJeya Plays YTNo ratings yet
- ReproductiveDocument4 pagesReproductiveZenab AlmussallamNo ratings yet
- Physical-Sexual Self MaterialDocument17 pagesPhysical-Sexual Self MaterialJhapzy Dinagat PerezNo ratings yet
- Uts Prefinal ModuleDocument14 pagesUts Prefinal ModuleValery Ann PaciaNo ratings yet
- Understanding The Self-Module2Document31 pagesUnderstanding The Self-Module2Dante Jr. BitoonNo ratings yet
- SexualityDocument64 pagesSexualityjmclacasNo ratings yet
- The Physical and Sexual Self: Puberty Is The Period of Life, Generally Between The Ages of 10 and 15 Years Old, When TheDocument8 pagesThe Physical and Sexual Self: Puberty Is The Period of Life, Generally Between The Ages of 10 and 15 Years Old, When ThePez BughawNo ratings yet
- Module 2 Lesson 1 Physical and Sexual SelfDocument6 pagesModule 2 Lesson 1 Physical and Sexual SelfRyan Kenneth Oliver E. MacahipayNo ratings yet
- Lecture 5 Human 100 Sir RalphDocument41 pagesLecture 5 Human 100 Sir RalphAngelica Mae PeriaNo ratings yet
- Module For Income TaxationDocument1 pageModule For Income TaxationHassel AbayonNo ratings yet
- Final Pec 102Document1 pageFinal Pec 102Hassel AbayonNo ratings yet
- NS 102 Module 2Document39 pagesNS 102 Module 2Hassel AbayonNo ratings yet
- Science Adv - Handouts - Outputlinks - GroupingsDocument3 pagesScience Adv - Handouts - Outputlinks - GroupingsHassel AbayonNo ratings yet
- Teaching Science ModuleDocument22 pagesTeaching Science ModuleHassel AbayonNo ratings yet
- NS 102 Module 2 To 4 2022-2023Document39 pagesNS 102 Module 2 To 4 2022-2023Hassel AbayonNo ratings yet
- Math 9 - Curriculum Map - 2021-2022 - 2Document4 pagesMath 9 - Curriculum Map - 2021-2022 - 2Hassel Abayon100% (1)
- Unit LP-Science 9Document7 pagesUnit LP-Science 9Hassel AbayonNo ratings yet
- Aurora Pioneers Memorial College: (Cebuano Barracks Institute)Document4 pagesAurora Pioneers Memorial College: (Cebuano Barracks Institute)Hassel AbayonNo ratings yet
- Math 7 - Curriculum Map - 2021-2022Document5 pagesMath 7 - Curriculum Map - 2021-2022Hassel Abayon0% (1)
- FIDPDocument7 pagesFIDPHassel AbayonNo ratings yet
- G.E Elect 110 Midtem ExamDocument2 pagesG.E Elect 110 Midtem ExamHassel Abayon100% (1)
- 2020 INSET For Junior High School (JHS) Teachers Via An Online Delivery ModeDocument2 pages2020 INSET For Junior High School (JHS) Teachers Via An Online Delivery ModeHassel AbayonNo ratings yet
- Ge Elect 110 Module 1Document5 pagesGe Elect 110 Module 1Hassel AbayonNo ratings yet
- Curriculum Map Math 10Document6 pagesCurriculum Map Math 10Hassel AbayonNo ratings yet
- CidamDocument8 pagesCidamHassel AbayonNo ratings yet
- CURRICULUM MAP Grade 9Document14 pagesCURRICULUM MAP Grade 9Hassel AbayonNo ratings yet
- Aurora, Zamboanga Del Sur: (Cebuano Barracks Institute)Document3 pagesAurora, Zamboanga Del Sur: (Cebuano Barracks Institute)Hassel AbayonNo ratings yet
- Flexible Instructional Delivery Plan (Fidp) : (Cebuano Barracks Institute)Document2 pagesFlexible Instructional Delivery Plan (Fidp) : (Cebuano Barracks Institute)Hassel AbayonNo ratings yet
- HRM SyllabusDocument3 pagesHRM SyllabusHassel AbayonNo ratings yet
- (Cebuano Barracks Institute) : Aurora, Zamboanga Del SurDocument1 page(Cebuano Barracks Institute) : Aurora, Zamboanga Del SurHassel AbayonNo ratings yet
- Soya BeanDocument5 pagesSoya BeanNityantiniNo ratings yet
- Prolia PatientBrochure English PDFDocument14 pagesProlia PatientBrochure English PDFwilhelmtewariNo ratings yet
- Burnout Psicológico de Mujeres Que Trabajan y Amas de Casa en La Etapa de La Menopausia en La Ciudad de Amman JordaniaDocument9 pagesBurnout Psicológico de Mujeres Que Trabajan y Amas de Casa en La Etapa de La Menopausia en La Ciudad de Amman JordaniaHanna BethNo ratings yet
- Xerosis CutisDocument6 pagesXerosis CutisHadi FirmansyahNo ratings yet
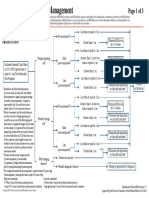
- Clin Management Ovarian Cysts WEB Algorithm-1Document3 pagesClin Management Ovarian Cysts WEB Algorithm-1linglingNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanPaul Loujin LeeNo ratings yet
- MRKH MenopauseDocument3 pagesMRKH Menopausediudiu93No ratings yet
- Estrasorb: Micellar Nanoparticle (MNP) Technology Was Invented in The Mid-1990s at Novavax DevelopedDocument11 pagesEstrasorb: Micellar Nanoparticle (MNP) Technology Was Invented in The Mid-1990s at Novavax DevelopedAnant Kumar SrivastavaNo ratings yet
- Gyn 9 - All Gynecology 5 2021Document22 pagesGyn 9 - All Gynecology 5 2021Menna Kamal100% (3)
- Synopsis DR - VasundhraDocument8 pagesSynopsis DR - Vasundhraprince395No ratings yet
- 500s Willcox Okinawa DietDocument17 pages500s Willcox Okinawa DietSorin Sorinos100% (1)
- 3RD Q Module 1 Quiz 2 Endocrine SystemDocument2 pages3RD Q Module 1 Quiz 2 Endocrine Systemsinunuc nhsNo ratings yet
- Approach To The Patient With An Adnexal Mass: 1 Table 1Document11 pagesApproach To The Patient With An Adnexal Mass: 1 Table 1Zyla PaulineNo ratings yet
- Evolution of Bhramari Pranayam in The Management of Menopausal SyndromeDocument7 pagesEvolution of Bhramari Pranayam in The Management of Menopausal SyndromeDr Kirti BhatiNo ratings yet
- Prasuti Tantra Striroga Paper 2Document20 pagesPrasuti Tantra Striroga Paper 2Girish Bhai MethaniyaNo ratings yet
- Chapter 6 - Endocrine System 2Document12 pagesChapter 6 - Endocrine System 2AyeshaNo ratings yet
- Women Health Lec 6Document27 pagesWomen Health Lec 6Shimaa WahidNo ratings yet
- Review: Diagnosis and Management of Premature Ovarian FailureDocument6 pagesReview: Diagnosis and Management of Premature Ovarian FailureKhong Jac MunNo ratings yet
- Dysfunctional Uterine Bleedin1Document15 pagesDysfunctional Uterine Bleedin1Hendy SetiawanNo ratings yet
- The Cortisol Rescue GuideDocument33 pagesThe Cortisol Rescue GuidekanishkbhatiaNo ratings yet
- Pulse 2018 - Obs and Gyne (Last Edit)Document37 pagesPulse 2018 - Obs and Gyne (Last Edit)Mohammad AlrefaiNo ratings yet
- 2014 06 22 The Healing Codes of The Divine MotherDocument10 pages2014 06 22 The Healing Codes of The Divine MotherfififlaunderNo ratings yet
- Homeopathy QuestionnaireDocument10 pagesHomeopathy Questionnaireshaileshvc0% (1)
- Lession PlanDocument14 pagesLession PlanShekhar SunthaNo ratings yet