Download as pdf or txt
You might also like
- Cyberpunk Red Data ScreenDocument4 pagesCyberpunk Red Data ScreenBrandie LynchNo ratings yet
- Test Bank For Essentials of Dental Radiography For Dental Assistants and Hygienists 10th Edition by ThompsonDocument14 pagesTest Bank For Essentials of Dental Radiography For Dental Assistants and Hygienists 10th Edition by ThompsonBarbara Hinkle100% (36)
- Torque in The Base Vs Torque in The FaceDocument5 pagesTorque in The Base Vs Torque in The FacePranshu Mathur100% (6)
- International Standard Test Method For RopesDocument26 pagesInternational Standard Test Method For RopesTziouris VasileiosNo ratings yet
- English AJODO 2004Document3 pagesEnglish AJODO 2004Diego Andres Hincapie HerreraNo ratings yet
- Loops in Orthodontics 3b1b23c9Document12 pagesLoops in Orthodontics 3b1b23c9Aly OsmanNo ratings yet
- Orthodontic WiresDocument10 pagesOrthodontic Wiresanon_191534692No ratings yet
- Bonin Et Al-2018-Catheterization and Cardiovascular InterventionsDocument6 pagesBonin Et Al-2018-Catheterization and Cardiovascular InterventionsPhan AnNo ratings yet
- Loopsinorthodontics 1Document13 pagesLoopsinorthodontics 1mona deby melantyNo ratings yet
- Investigation of Long Riser VIV PDFDocument6 pagesInvestigation of Long Riser VIV PDFsuzilamatsallehNo ratings yet
- Preprint Petersen MechSystemsSignalProcessing 20151Document27 pagesPreprint Petersen MechSystemsSignalProcessing 20151MBADJOUN DanielNo ratings yet
- Predictable Method To Deliver Physiologic Force For Extrusion of Palatally Impacted Maxillary CaninesDocument9 pagesPredictable Method To Deliver Physiologic Force For Extrusion of Palatally Impacted Maxillary CanineschaitreeNo ratings yet
- A Method To Determine The Kink Resistance of Stents and Stent Delivery Systems According To International StandardsDocument4 pagesA Method To Determine The Kink Resistance of Stents and Stent Delivery Systems According To International StandardsAxel MaldonadoNo ratings yet
- The Biomechanics of Lag Screw Insertion A ComparisDocument2 pagesThe Biomechanics of Lag Screw Insertion A ComparisCamilo Marin TovarNo ratings yet
- (MOORINGS) Otc17789 - Predicting The Torsional Response of Large Mooring Chains PDFDocument0 pages(MOORINGS) Otc17789 - Predicting The Torsional Response of Large Mooring Chains PDFAndrew EdwardNo ratings yet
- Jurnal Hypothetical DataDocument7 pagesJurnal Hypothetical DatamuhnameiskristinNo ratings yet
- 3 To 7 Years Longit Study 2004Document6 pages3 To 7 Years Longit Study 2004Hicham AL KHAYARNo ratings yet
- AJODO-98 Clinical Comparison and PerformanceDocument8 pagesAJODO-98 Clinical Comparison and PerformancevaleriaNo ratings yet
- Evaluation of Stent Performan Ce Using Fea Considering A Reali Stic Baloon ExpansionDocument19 pagesEvaluation of Stent Performan Ce Using Fea Considering A Reali Stic Baloon ExpansionduggubabuNo ratings yet
- Design Verification of Winch For Offshore Cranes PDFDocument4 pagesDesign Verification of Winch For Offshore Cranes PDFtonyNo ratings yet
- 04072930Document13 pages04072930df_campos3353No ratings yet
- Measurement of Friction Forces Between Stainless Steel Wires and Reduced-Friction'' Self-Ligating BracketsDocument9 pagesMeasurement of Friction Forces Between Stainless Steel Wires and Reduced-Friction'' Self-Ligating BracketsChintan ChitrodaNo ratings yet
- Schmidt 2009Document11 pagesSchmidt 2009investigation SLTLMNo ratings yet
- Chapter 1 - Coronary WiresDocument9 pagesChapter 1 - Coronary WiresRakesh DashNo ratings yet
- An 385Document8 pagesAn 385Indah GitaswariNo ratings yet
- International Journal of Medical Science and Innovative Research (IJMSIR)Document18 pagesInternational Journal of Medical Science and Innovative Research (IJMSIR)Muhammad UzairNo ratings yet
- Sobre Dent A Duras 1Document6 pagesSobre Dent A Duras 1LahurentAndresMejíaNo ratings yet
- HE Elationship Etween Mplant Reload and Crew Oosening On Mplant Supported RosthesesDocument7 pagesHE Elationship Etween Mplant Reload and Crew Oosening On Mplant Supported RosthesesSalam AlbaradieNo ratings yet
- These 2017 SPI Genie Electrique OUBRAHIM ZakaryaDocument151 pagesThese 2017 SPI Genie Electrique OUBRAHIM ZakaryanouhailaNo ratings yet
- Fixation of Regan-Morrey Type II Coronoid Fractures: A Comparison of Screws and Suture Lasso Technique For Resistance To DisplacementDocument4 pagesFixation of Regan-Morrey Type II Coronoid Fractures: A Comparison of Screws and Suture Lasso Technique For Resistance To DisplacementpakemainmainNo ratings yet
- Surgeons - Total Acetabular Allografts ( (Dagger) ) Instructional Course Lectures, The American Academy of OrthopaedicDocument13 pagesSurgeons - Total Acetabular Allografts ( (Dagger) ) Instructional Course Lectures, The American Academy of OrthopaedicYariel AraujoNo ratings yet
- Vibration Analysis of Two Wheeler Connecting Rod: Yeshwant Rao, B S Praveen KumarDocument3 pagesVibration Analysis of Two Wheeler Connecting Rod: Yeshwant Rao, B S Praveen KumarIonut PuscasuNo ratings yet
- Broussard 1964Document19 pagesBroussard 1964drzana78No ratings yet
- Leads and Longevity: How Long Will Your Pacemaker Last?: Richard K. Shepard and Kenneth A. EllenbogenDocument2 pagesLeads and Longevity: How Long Will Your Pacemaker Last?: Richard K. Shepard and Kenneth A. Ellenbogenwahyu suparnoNo ratings yet
- Lab Sheet Tensile Test Steel BarDocument4 pagesLab Sheet Tensile Test Steel BarAbdul nurNo ratings yet
- Condition Monitoring Technologies For Steel Wire Ropes - A ReviewDocument15 pagesCondition Monitoring Technologies For Steel Wire Ropes - A Reviewomar_jamesNo ratings yet
- Krischek2011Document9 pagesKrischek2011Pao PusanisaNo ratings yet
- Experimental and Theoretical Investigation of Prestressing Steel Strand Subjected To Tensile LoadDocument29 pagesExperimental and Theoretical Investigation of Prestressing Steel Strand Subjected To Tensile LoadVarun MangaloreNo ratings yet
- Comparison of Short Term Outcomes Between Endovenous 1940 NM Laser Ablation and 6981Document4 pagesComparison of Short Term Outcomes Between Endovenous 1940 NM Laser Ablation and 6981KHALIL JOUININo ratings yet
- Apex LocatorsDocument19 pagesApex LocatorsChandra Dhar DwivediNo ratings yet
- 2016 16 NDT WireropesDocument2 pages2016 16 NDT WireropessarcofilusNo ratings yet
- Double LayerCarotidStentWissgott2015Document7 pagesDouble LayerCarotidStentWissgott2015Nick NgoNo ratings yet
- Flexibility and Trackability of Laser Cut Coronary Stent SystemsDocument8 pagesFlexibility and Trackability of Laser Cut Coronary Stent SystemsManoj NarukaNo ratings yet
- Chaconas1984 PDFDocument4 pagesChaconas1984 PDFdrzana78No ratings yet
- 1 PDFDocument4 pages1 PDFJHON JAIRO ROJASNo ratings yet
- Braun S Et Al., 1999Document9 pagesBraun S Et Al., 1999Anonymous J320GAJ2otNo ratings yet
- An CorasDocument7 pagesAn CorasMarcelo Wiltemburg AlvesNo ratings yet
- Power SystemDocument64 pagesPower SystemBOGGULA SURENDAR REDDYNo ratings yet
- Comparison of Torsional Stability of 2 Types of Split Crimpable Surgical Hooks With Soldered Brass Surgical HooksDocument5 pagesComparison of Torsional Stability of 2 Types of Split Crimpable Surgical Hooks With Soldered Brass Surgical HooksГне ДзжNo ratings yet
- DP CellDocument18 pagesDP CellbrindaNo ratings yet
- Experimental Investigation of Performanc PDFDocument10 pagesExperimental Investigation of Performanc PDFdeepeshsagarNo ratings yet
- Gleason Reel - Reeling SystemsDocument17 pagesGleason Reel - Reeling SystemsMahmoud ElboraeNo ratings yet
- Tensile Testing Faqs: February 2022Document9 pagesTensile Testing Faqs: February 2022AMIRTHARAAJ A/L VIJAYAN MBS211063No ratings yet
- Volar Locking Plates Versus Kirschner Wires For Distal Radial Fractures-A Cost Analysis StudyDocument3 pagesVolar Locking Plates Versus Kirschner Wires For Distal Radial Fractures-A Cost Analysis StudyAli AliNo ratings yet
- An Investigation Into The Effect of Denture Adhesives On Incisal Bite Force of Complete Denture Wearers Using Pressure Transducers - A Clinical StudyDocument6 pagesAn Investigation Into The Effect of Denture Adhesives On Incisal Bite Force of Complete Denture Wearers Using Pressure Transducers - A Clinical StudypalliNo ratings yet
- ad77794c5d4d03fa77cba9f6c926993aDocument8 pagesad77794c5d4d03fa77cba9f6c926993aValeriaNo ratings yet
- Analysis of Strain at Selected Bone Sites of A Cantilevered Implant-Supported ProsthesisDocument7 pagesAnalysis of Strain at Selected Bone Sites of A Cantilevered Implant-Supported ProsthesisMR GOKCHENNo ratings yet
- Baker Surge Testing Electric Motors WPDocument8 pagesBaker Surge Testing Electric Motors WPBisto MasiloNo ratings yet
- Comparison of Strength and Failure Mode of Seven Implant Systems: An in Vitro TestDocument10 pagesComparison of Strength and Failure Mode of Seven Implant Systems: An in Vitro TestDr FarhatNo ratings yet
- 2013 Advances in Tribological Testing of Arti Cial Joint Biomaterials Using Multidirectional Pin-On-Disk TestersDocument18 pages2013 Advances in Tribological Testing of Arti Cial Joint Biomaterials Using Multidirectional Pin-On-Disk TestersFarhanNo ratings yet
- Mechanical Properties of Wires and Its Orthodontic ApplicationDocument12 pagesMechanical Properties of Wires and Its Orthodontic Applicationabhishek_meenuNo ratings yet
- An Introduction to Biomedical Instrumentation: Pergamon International Library of Science, Technology, Engineering and Social StudiesFrom EverandAn Introduction to Biomedical Instrumentation: Pergamon International Library of Science, Technology, Engineering and Social StudiesRating: 1 out of 5 stars1/5 (1)
- Transportation Validation ProtocolDocument2 pagesTransportation Validation ProtocolKhushboo Warhade100% (1)
- Surface Area For BiocompatibilityDocument34 pagesSurface Area For BiocompatibilityKhushboo WarhadeNo ratings yet
- MRD Carotid StentDocument5 pagesMRD Carotid StentKhushboo WarhadeNo ratings yet
- Mimicking Soft Living Tissues For 3D Printed Surgical Planning Prototypes Using Different MaterialsDocument5 pagesMimicking Soft Living Tissues For 3D Printed Surgical Planning Prototypes Using Different MaterialsKhushboo WarhadeNo ratings yet
- MPC Durethane-S 11 - 4Document2 pagesMPC Durethane-S 11 - 4Khushboo WarhadeNo ratings yet
- ACFrOgAbfh9MQqF T2zJql CgjL58dkcbaWRgwWqadW1hkwrQXfNpAKO0YLZTwlVEDReOsAOrckY PxpSZT8UuLB KE6ecrxMyxali7rRaUuYvYgU6kIXI1jT7u8bB D YiMroXuL0ZA6acCXPDbDocument2 pagesACFrOgAbfh9MQqF T2zJql CgjL58dkcbaWRgwWqadW1hkwrQXfNpAKO0YLZTwlVEDReOsAOrckY PxpSZT8UuLB KE6ecrxMyxali7rRaUuYvYgU6kIXI1jT7u8bB D YiMroXuL0ZA6acCXPDbKhushboo WarhadeNo ratings yet
- EN CS 4 DA NL FR DE EL HU IT NO PL PT ES SV: MedicalDocument48 pagesEN CS 4 DA NL FR DE EL HU IT NO PL PT ES SV: MedicalKhushboo WarhadeNo ratings yet
- Padlock ClipDocument116 pagesPadlock ClipKhushboo WarhadeNo ratings yet
- Online Consult Patient Telemedicine Consent, Disclaimer and Release FormDocument3 pagesOnline Consult Patient Telemedicine Consent, Disclaimer and Release FormDiwas UpadhyayNo ratings yet
- How To Give An Im Injection Portfolio Track ChangesDocument4 pagesHow To Give An Im Injection Portfolio Track Changesapi-582970027No ratings yet
- Students Assignment SheetDocument2 pagesStudents Assignment Sheetjoy daladagNo ratings yet
- 09 2023uganda Demographic and Health Survey (Udhs) 2022 Key FindingsDocument67 pages09 2023uganda Demographic and Health Survey (Udhs) 2022 Key FindingsYIKI ISAACNo ratings yet
- DF50、DF51、DF53 Auto Hematology Analyzer Service Manual - V6.0Document124 pagesDF50、DF51、DF53 Auto Hematology Analyzer Service Manual - V6.0Arnoldo FelixNo ratings yet
- Homeopathic Medicine List-SymptomsDocument2 pagesHomeopathic Medicine List-SymptomsMask55No ratings yet
- 10%approval Hospital Claims-March2013Document52 pages10%approval Hospital Claims-March2013abdulkhaderjeelani14No ratings yet
- G.01 Orthopaedic Implant - Brochure - 06.07.2021 - 4Document1 pageG.01 Orthopaedic Implant - Brochure - 06.07.2021 - 4mostafa adelNo ratings yet
- Daftar Obat Lasa BaruDocument3 pagesDaftar Obat Lasa Baruyuni winarniNo ratings yet
- Dilution FormulaDocument2 pagesDilution FormulaFazilah ShahromNo ratings yet
- Corazon Aquino Delivery RoomDocument5 pagesCorazon Aquino Delivery RoomJustine CagatanNo ratings yet
- Andangin 4-Badac Data Capture FormsDocument8 pagesAndangin 4-Badac Data Capture FormsMikaela FernandezNo ratings yet
- Herbal Healing Practices of Indigenous Irular Tribal Peoples of Sendurai Block at Ariyalur District TamilnaduDocument8 pagesHerbal Healing Practices of Indigenous Irular Tribal Peoples of Sendurai Block at Ariyalur District TamilnaduJyotsana JonwalNo ratings yet
- Idma Bulletin 7TH April 2021Document72 pagesIdma Bulletin 7TH April 2021RAKESH KUMARNo ratings yet
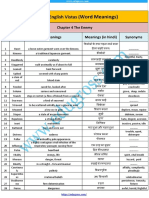
- Chapter 4 The EnemyDocument4 pagesChapter 4 The EnemyAnil DangiNo ratings yet
- WHO Labour Care Guide at GraphDocument1 pageWHO Labour Care Guide at GraphAnonymous efqPXILEQJNo ratings yet
- Brochure ASPICon2023Document12 pagesBrochure ASPICon2023Naveen KumarNo ratings yet
- Self Introduction / My Job and Responsibilities: BY: Nova MustikaDocument8 pagesSelf Introduction / My Job and Responsibilities: BY: Nova MustikaannisaNo ratings yet
- FHSIS 2021 Annual Report v2Document155 pagesFHSIS 2021 Annual Report v2isnainfsonlineNo ratings yet
- Keracunan Coklat (Theobroma Cacao) Pada Anjing: Manajemen Terapi Dan PencegahanDocument13 pagesKeracunan Coklat (Theobroma Cacao) Pada Anjing: Manajemen Terapi Dan PencegahanGharsina SorayaNo ratings yet
- 2021 Cape Town Atls Course ScheduleDocument2 pages2021 Cape Town Atls Course Schedulermullah23No ratings yet
- 1. Đề số 01Document25 pages1. Đề số 01havietvuNo ratings yet
- Anglais Mock Probatoire Acdti 2024Document5 pagesAnglais Mock Probatoire Acdti 2024Jean MbargaNo ratings yet
- Journal HomepageDocument11 pagesJournal HomepageIJAR JOURNALNo ratings yet
- Addis Ababa Sciece and Technology University Collage of Biological and Chemical Engineering Department of BiotechnologyDocument14 pagesAddis Ababa Sciece and Technology University Collage of Biological and Chemical Engineering Department of BiotechnologyEshetu ShemetNo ratings yet
- Alaribe 2021Document7 pagesAlaribe 2021CoNo ratings yet
- Dental Crowding AbdullahDocument15 pagesDental Crowding AbdullahAbdullah Muhammed khaleel HassanNo ratings yet
- Ifra 20356800Document9 pagesIfra 20356800Carlos Gonzalez CastroNo ratings yet