Download as pdf or txt
You might also like
- Osteopathic Considerations in Systemic Dysfunction (2nd Ed)Document296 pagesOsteopathic Considerations in Systemic Dysfunction (2nd Ed)Natan Babek100% (1)
- Risk Factors For post-ERCP Pancreatitis: A Systematic Review of Clinical Trials With A Large Sample Size in The Past 10 YearsDocument7 pagesRisk Factors For post-ERCP Pancreatitis: A Systematic Review of Clinical Trials With A Large Sample Size in The Past 10 YearsEmanuel CandelasNo ratings yet
- The Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFDocument9 pagesThe Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFCristobal Alejandro Falado SantanderNo ratings yet
- Blue Dye TestDocument9 pagesBlue Dye TestMacarena Elizabeth Olavarría Gómez100% (1)
- PIIS2214109X23001353Document14 pagesPIIS2214109X23001353Joaquin OlivaresNo ratings yet
- Validity and Reliability of The Novel Thyroid-Specific Quality of Life Questionnaire, ThyproDocument7 pagesValidity and Reliability of The Novel Thyroid-Specific Quality of Life Questionnaire, ThyproPriyanaka NaraniyaNo ratings yet
- 10.1007@s00383 019 04527 9Document18 pages10.1007@s00383 019 04527 9Claudia Sughey Herrera PalominoNo ratings yet
- Metanalisis 2010Document11 pagesMetanalisis 2010Elmer chavezNo ratings yet
- Laparoscopic Versus Conventional Appendectomy - A Meta-Analysis of Randomized Controlled TrialsDocument8 pagesLaparoscopic Versus Conventional Appendectomy - A Meta-Analysis of Randomized Controlled TrialsAdrian HaningNo ratings yet
- Ultrasound Imaging Reduces Failure Rates of Percutaneous Central Venous Catheterization in ChildrenDocument8 pagesUltrasound Imaging Reduces Failure Rates of Percutaneous Central Venous Catheterization in Childrenangelama1783riosNo ratings yet
- (13360329 - Endocrine Regulations) Elevated Neutrophil-Lymphocyte Ratio in Patients With Euthyroid Chronic Autoimmune ThyreotidisDocument6 pages(13360329 - Endocrine Regulations) Elevated Neutrophil-Lymphocyte Ratio in Patients With Euthyroid Chronic Autoimmune Thyreotidisjournal proNo ratings yet
- Hirscprung 2 PDFDocument5 pagesHirscprung 2 PDFputriNo ratings yet
- Edinburgh Research ExplorerDocument11 pagesEdinburgh Research ExplorerBurhan SabirNo ratings yet
- Abses HeparDocument4 pagesAbses HeparIecHa RizkaMaulidaNo ratings yet
- Management of Patients Admitted With Pneumothorax: A Multi-Centre Study of The Practice and Outcomes in Hong KongDocument7 pagesManagement of Patients Admitted With Pneumothorax: A Multi-Centre Study of The Practice and Outcomes in Hong Kongハルァン ファ烏山No ratings yet
- Tratamiento Esofago Cervical Lu, 2021Document9 pagesTratamiento Esofago Cervical Lu, 2021Carlos N. Rojas PuyolNo ratings yet
- Thyroid NodulesDocument34 pagesThyroid NodulesEphobiaNo ratings yet
- Dor Versus Toupet Fundoplication After Laparoscopic Heller Myotomy: Systematic Review and Bayesian Meta-Analysis of Randomized Controlled TrialsDocument9 pagesDor Versus Toupet Fundoplication After Laparoscopic Heller Myotomy: Systematic Review and Bayesian Meta-Analysis of Randomized Controlled TrialsDavids MarinNo ratings yet
- Cuff-Leak Test For Predicting Postextubation Airway Complications: A Systematic ReviewDocument13 pagesCuff-Leak Test For Predicting Postextubation Airway Complications: A Systematic ReviewMau MillanNo ratings yet
- GADAR Abdominal PainDocument7 pagesGADAR Abdominal PainIlham salman AlawyNo ratings yet
- Research Journal ClubDocument12 pagesResearch Journal ClubUsama SalehNo ratings yet
- Ablación Con Etanol QuistesDocument15 pagesAblación Con Etanol Quistesjessica MárquezNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleReagen DeNo ratings yet
- The Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyDocument6 pagesThe Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyArizkamhNo ratings yet
- Am J Gastro - NET - 2010Document9 pagesAm J Gastro - NET - 2010RobiViNo ratings yet
- Jurnal 3 - Husnul AridhaDocument9 pagesJurnal 3 - Husnul AridhaHusnul AridhaNo ratings yet
- Research: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysisDocument7 pagesResearch: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysiswindaintanpNo ratings yet
- Biopsia Endoscopica Guiada Por UsDocument12 pagesBiopsia Endoscopica Guiada Por UsDavidNo ratings yet
- Efficacy of Transoral IncisionDocument14 pagesEfficacy of Transoral IncisionResidentes CirugiaNo ratings yet
- Evaluation of Fowler-Stephens Orchiopexy For High-Level Intra-Abdominal Cryptorchidism A Systematic Review and Meta-AnalysisDocument15 pagesEvaluation of Fowler-Stephens Orchiopexy For High-Level Intra-Abdominal Cryptorchidism A Systematic Review and Meta-AnalysisAL MUNAWIRNo ratings yet
- MallapatiDocument8 pagesMallapatiudjkwNo ratings yet
- Supine Versus Prone Position For Percutaneous Nephrolit - 2019 - International JDocument10 pagesSupine Versus Prone Position For Percutaneous Nephrolit - 2019 - International JFelicia JesslynNo ratings yet
- Tang 2019Document8 pagesTang 2019sarahsamaliaNo ratings yet
- Is The Supine Position Superior To The Prone Position For Percutaneous Nephrolithotomy (PCNL) ?Document7 pagesIs The Supine Position Superior To The Prone Position For Percutaneous Nephrolithotomy (PCNL) ?Iqbal TafwidNo ratings yet
- Treatment of Enterocutaneous Fistula A Systematic Review and MetaanalysisDocument12 pagesTreatment of Enterocutaneous Fistula A Systematic Review and MetaanalysisMarcus CezilloNo ratings yet
- A Systematic Review of Satisfaction With TeledermatologyDocument8 pagesA Systematic Review of Satisfaction With Teledermatologysri karuniaNo ratings yet
- There Is No Evidence To Support Use of Occlusal Adjustment For Prevention or Treatment of TMDDocument1 pageThere Is No Evidence To Support Use of Occlusal Adjustment For Prevention or Treatment of TMDTomas Raul Wiche SalinasNo ratings yet
- Adapted T Cell Interferon-Gamma Release Assay For The Diagnosis of Pleural TuberculosisDocument8 pagesAdapted T Cell Interferon-Gamma Release Assay For The Diagnosis of Pleural TuberculosisMikael Reynardi SutantoNo ratings yet
- David Zurakowski, James Di Canzio, and Joseph A. MajzoubDocument5 pagesDavid Zurakowski, James Di Canzio, and Joseph A. MajzoubChaitanya Kumar ChaituNo ratings yet
- 1 s2.0 S1553725021000982 MainDocument7 pages1 s2.0 S1553725021000982 MainNovia khasanahNo ratings yet
- Percutaneous Needle Aspiration Versus Catheter Drainage in Treating Hepatic AbscessDocument8 pagesPercutaneous Needle Aspiration Versus Catheter Drainage in Treating Hepatic AbscessRatna TriasnawatiNo ratings yet
- Clinical Presentation and Treatment Outcomes of Thyroglossal Duct Cysts: A Systematic ReviewDocument8 pagesClinical Presentation and Treatment Outcomes of Thyroglossal Duct Cysts: A Systematic ReviewR KNo ratings yet
- Research Forum Abstracts: 70, No. 4s: October 2017 Annals of Emergency MedicineDocument2 pagesResearch Forum Abstracts: 70, No. 4s: October 2017 Annals of Emergency Medicinerachmat hidayatNo ratings yet
- PAVM em Terapia IntensivaDocument10 pagesPAVM em Terapia IntensivaVictor Hugo SilveiraNo ratings yet
- Research Article: Paediatric Posttonsillectomy Haemorrhage Rates in Auckland: A Retrospective Case SeriesDocument6 pagesResearch Article: Paediatric Posttonsillectomy Haemorrhage Rates in Auckland: A Retrospective Case SeriesJeffrey EkaNo ratings yet
- Apendicitis AgudaDocument17 pagesApendicitis Agudalbritez7No ratings yet
- An Updated Meta Analysis of Laparoscopic Versus Open Repair For Perforated Peptic UlcerDocument13 pagesAn Updated Meta Analysis of Laparoscopic Versus Open Repair For Perforated Peptic UlcerSANDRA MILENA GUTIERREZ CAÑASNo ratings yet
- Clinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyDocument8 pagesClinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyPriya JainNo ratings yet
- Effectiveness of Cough Exercise and Expiratory Muscle Training: A Meta-AnalysisDocument6 pagesEffectiveness of Cough Exercise and Expiratory Muscle Training: A Meta-AnalysisDian Andi PrastiyoNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Prothrombin Time and Activated Partial Thromboplastin Time in Pregnant Women Attending Antenatal Clinic at Nnamdi Azikiwe University Teaching Hospital (Nauth), Nnewi, Nigeria - A Cohort StudyDocument4 pagesProthrombin Time and Activated Partial Thromboplastin Time in Pregnant Women Attending Antenatal Clinic at Nnamdi Azikiwe University Teaching Hospital (Nauth), Nnewi, Nigeria - A Cohort StudyasclepiuspdfsNo ratings yet
- Laparoscopic Versus Open Pediatric Inguinal Hernia RepairDocument15 pagesLaparoscopic Versus Open Pediatric Inguinal Hernia Repairmelon segerNo ratings yet
- 1 s2.0 S2590280622000079 MainDocument10 pages1 s2.0 S2590280622000079 MainDimas Bintoro KyhNo ratings yet
- Pone 0190952Document14 pagesPone 0190952SangiliNo ratings yet
- Critical Appraisal For RCT & Meta AnalisisDocument8 pagesCritical Appraisal For RCT & Meta AnalisisHanniNo ratings yet
- Luan2019 PDFDocument12 pagesLuan2019 PDFrifki irsyadNo ratings yet
- Merola 2021Document10 pagesMerola 2021FedericoNo ratings yet
- Diagnostic Accuracy of Ultrasonography and Radiography in Detection of Pulmonary Contusion A Systematic Review and Meta-AnalysisDocument10 pagesDiagnostic Accuracy of Ultrasonography and Radiography in Detection of Pulmonary Contusion A Systematic Review and Meta-AnalysisfahrunisaNo ratings yet
- International Journal of Surgery: ReviewDocument14 pagesInternational Journal of Surgery: ReviewRizka Desti AyuniNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Mendeley CiteDocument1 pageMendeley CiteEngga CandranataNo ratings yet
- Defining The Degree of Intravesical Prostatic Protrusion in Association With Bladder Outlet ObstructionDocument4 pagesDefining The Degree of Intravesical Prostatic Protrusion in Association With Bladder Outlet ObstructionEngga CandranataNo ratings yet
- MainDocument7 pagesMainEngga CandranataNo ratings yet
- Factors Affecting Postoperative Respiratory Tract Function in Type-C Esophageal Atresia. Thoracoscopic Versus Open RepairDocument5 pagesFactors Affecting Postoperative Respiratory Tract Function in Type-C Esophageal Atresia. Thoracoscopic Versus Open RepairEngga CandranataNo ratings yet
- Outcome Reporting in Randomized Controlled Trials and Systematic Reviews of Gastroschisis Treatment A Systematic ReviewDocument5 pagesOutcome Reporting in Randomized Controlled Trials and Systematic Reviews of Gastroschisis Treatment A Systematic ReviewEngga CandranataNo ratings yet
- Q&A Random Selection #16Document5 pagesQ&A Random Selection #16Yuuki Chitose (tai-kun)No ratings yet
- 7.stool Examination - Morphology of Eggs, Cysts, LarvaeDocument9 pages7.stool Examination - Morphology of Eggs, Cysts, LarvaeKowshik AvulaNo ratings yet
- Avian ImmunityDocument65 pagesAvian Immunityarmanda06No ratings yet
- HDU AuditDocument3 pagesHDU AuditAsdf DgfhgNo ratings yet
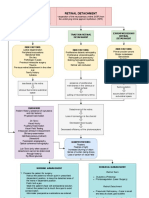
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Sade, Robert M. 2012 "The Graying of America Challenges and ControversiesDocument8 pagesSade, Robert M. 2012 "The Graying of America Challenges and ControversiesTengiz VerulavaNo ratings yet
- Canine OA Recognition and ManagementDocument10 pagesCanine OA Recognition and ManagementAngeles MerinoNo ratings yet
- History Taking FormDocument9 pagesHistory Taking FormEren ErkılınçNo ratings yet
- Name Module No: - 8 - Module Title: Learners With Difficulty Seeing Course and Section: BSED-3A - Major: Social ScienceDocument6 pagesName Module No: - 8 - Module Title: Learners With Difficulty Seeing Course and Section: BSED-3A - Major: Social ScienceChristine Joy MarcelNo ratings yet
- Anemia in Children CBC (Complete Blood Count)Document4 pagesAnemia in Children CBC (Complete Blood Count)Edraline LumawigNo ratings yet
- Boundless March 2021Document12 pagesBoundless March 2021Shafay AsgharNo ratings yet
- Nosocomial Infections: Causes, Controls, Preventions and Future ChallengesDocument11 pagesNosocomial Infections: Causes, Controls, Preventions and Future ChallengesAy GlassesNo ratings yet
- Nebosh Igc2 QaDocument12 pagesNebosh Igc2 Qaselvaprpc50% (2)
- Renal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityDocument8 pagesRenal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityManci Bito-onNo ratings yet
- Full Ebook of Surgery Sixer For Nbe 5Th Edition R Rajamahendran Harindra Sandhu Online PDF All ChapterDocument69 pagesFull Ebook of Surgery Sixer For Nbe 5Th Edition R Rajamahendran Harindra Sandhu Online PDF All Chapterchestersandlin305982100% (5)
- GENERAL WARD Sample Case PresDocument4 pagesGENERAL WARD Sample Case PresCons Tan TinoNo ratings yet
- Intellectual Disability: Menchie M. Garachico Freddie C. Santos JRDocument42 pagesIntellectual Disability: Menchie M. Garachico Freddie C. Santos JRTEAM SPORTS GADTCNo ratings yet
- Module 1Document10 pagesModule 1Katelyn Algones Toledo100% (1)
- Capitulo 5 StudervantDocument23 pagesCapitulo 5 StudervantDiegoMoralesNo ratings yet
- 4D OvaryDocument108 pages4D OvaryrubenNo ratings yet
- GMP Dry SausageDocument26 pagesGMP Dry SausageJade NguyenNo ratings yet
- Using Visual Rating To Diagnose DementiaDocument10 pagesUsing Visual Rating To Diagnose DementiaImágenes Rosendo GarcíaNo ratings yet
- Facility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileDocument2 pagesFacility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileHeba HanyNo ratings yet
- Computers in Biology and MedicineDocument9 pagesComputers in Biology and MedicinePraneethaNo ratings yet
- Multiple Endocrine NeoplasiaDocument10 pagesMultiple Endocrine NeoplasiacarmenNo ratings yet
- 纽约时报 New York TimesDocument6 pages纽约时报 New York TimesMauricio PadronNo ratings yet
- Nej MC 2201160Document3 pagesNej MC 2201160Πάνος ΣταγήςNo ratings yet
- 2 Davao City Health - Case Investigation FormDocument3 pages2 Davao City Health - Case Investigation FormRobee Camille Desabelle-SumatraNo ratings yet
- Practice Teaching: Era UniversityDocument14 pagesPractice Teaching: Era UniversityAru VermaNo ratings yet