Download as pdf or txt
You might also like
- Antibiotic Mixing Chart With SAMF InfoDocument8 pagesAntibiotic Mixing Chart With SAMF Infosumayyah995No ratings yet
- Diabetes Mellitus National Clinical Management Guidelines Final Approved Version High Reso PDF July 6 2021Document107 pagesDiabetes Mellitus National Clinical Management Guidelines Final Approved Version High Reso PDF July 6 2021محمداحمد محمدنور ابايزيدNo ratings yet
- A Drug For IntDocument58 pagesA Drug For IntVajirawit PetchsriNo ratings yet
- Peds Table 07Document1 pagePeds Table 07do101504No ratings yet
- Noradrenaline Infusion Rate BSUH Critical CareDocument4 pagesNoradrenaline Infusion Rate BSUH Critical CareAndreiCostei100% (1)
- Pedia DosesDocument7 pagesPedia DosesSai Krishna MaddiralaNo ratings yet
- NOte BookDocument81 pagesNOte BookDr abdiaziz osman JamaNo ratings yet
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanNo ratings yet
- Malaria Treatment IndiaDocument1 pageMalaria Treatment IndiaSubzer OmerNo ratings yet
- Station 3 LeafletDocument5 pagesStation 3 LeafletFelicianna Ashwinie StanleyNo ratings yet
- 1st Lecture of Respiratory Histology by DR RoomiDocument24 pages1st Lecture of Respiratory Histology by DR RoomiMudassar Roomi100% (1)
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- Smart Pumps Adult ITU Library v3Document73 pagesSmart Pumps Adult ITU Library v3Aqsa Ahmed SiddiquiNo ratings yet
- Pediatric DosesDocument20 pagesPediatric Doseshamadadodo550% (2)
- I Need Doctor On Duty Book PDFDocument52 pagesI Need Doctor On Duty Book PDFAbdullah Jan100% (1)
- Maintenance Fluid Therapy in ChildrenDocument4 pagesMaintenance Fluid Therapy in ChildrenNicole_0No ratings yet
- Drug ListDocument2 pagesDrug ListhahahahaaaaaaaNo ratings yet
- Paediatric Anaesthesia GuideDocument1 pagePaediatric Anaesthesia GuideAndrewBeckNo ratings yet
- Royal Manchester Children's Hospital - PICU (Version 12.0)Document2 pagesRoyal Manchester Children's Hospital - PICU (Version 12.0)ibnNo ratings yet
- Drug ListDocument8 pagesDrug ListpeachandmintsNo ratings yet
- Acute MedicineDocument54 pagesAcute MedicineTipuNo ratings yet
- FormulaDocument5 pagesFormulaEloiseBalasbasNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Common TreatmentsDocument5 pagesCommon TreatmentsRaj MandumulaNo ratings yet
- Cardiovascular Diagnostic Tests & Procedures.Document25 pagesCardiovascular Diagnostic Tests & Procedures.Salman KhanNo ratings yet
- Infusions in CCU 2Document1 pageInfusions in CCU 2MimiNo ratings yet
- PICU Drug Infusions: Drug Add To 50ml Notes Dose Range 1ml/hrDocument2 pagesPICU Drug Infusions: Drug Add To 50ml Notes Dose Range 1ml/hrNeethu Mariya MathewNo ratings yet
- Resuscitation MedicationDocument1 pageResuscitation MedicationDen SinyoNo ratings yet
- Neonate: TPR of Newborns BW 1500gDocument9 pagesNeonate: TPR of Newborns BW 1500gAnne Lorraine BringasNo ratings yet
- Paediatric DosesDocument2 pagesPaediatric DosesEdio PathicNo ratings yet
- Antibiotic IV Administration During COVID-19Document5 pagesAntibiotic IV Administration During COVID-19David Hines LopezNo ratings yet
- Spinal Cord CompressionDocument4 pagesSpinal Cord Compressionian3yeung-2No ratings yet
- Quick Reference Guide Corrections 2021Document6 pagesQuick Reference Guide Corrections 2021Prashin RocharamNo ratings yet
- 2015 Pain Management For PediatricDocument2 pages2015 Pain Management For Pediatricdiany astutiNo ratings yet
- Pedia Notes - 112923Document59 pagesPedia Notes - 112923RASHEED ALADDIN N GUIOMALANo ratings yet
- Recommended Dose Revised 1 PDFDocument3 pagesRecommended Dose Revised 1 PDFmikayNo ratings yet
- S.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlDocument3 pagesS.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlmrs raamNo ratings yet
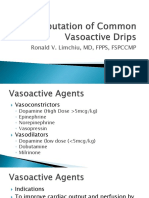
- Computation of Common Vasoactive DripsDocument23 pagesComputation of Common Vasoactive DripsRoxanneGailBigcasGoleroNo ratings yet
- Antibiotic Dosing Guidelines For Renal ImpairmentDocument6 pagesAntibiotic Dosing Guidelines For Renal ImpairmentvitauxianaNo ratings yet
- Critical Care Drugs 2Document23 pagesCritical Care Drugs 2Asri Ernadi100% (1)
- Elsharnoby Pediatric Made Easy Up Load Waheed Tantawy 2014Document160 pagesElsharnoby Pediatric Made Easy Up Load Waheed Tantawy 2014Emad AdelNo ratings yet
- Criticalcaredrugs PDFDocument2 pagesCriticalcaredrugs PDFRakhmat RamadhaniNo ratings yet
- Ioc Gold StandardDocument6 pagesIoc Gold StandardjohnNo ratings yet
- 2014 SHC ABX Dosing GuideDocument4 pages2014 SHC ABX Dosing GuideisnaeniNo ratings yet
- ICU IV Infusion GuidelinesDocument2 pagesICU IV Infusion Guidelinessgod34No ratings yet
- Syrup Prescription in Infants and ChildrenDocument1 pageSyrup Prescription in Infants and ChildrenRawa MuhsinNo ratings yet
- Ans 2 PDFDocument101 pagesAns 2 PDFrab yoNo ratings yet
- Best Practice in ShockDocument30 pagesBest Practice in ShockFoungZanz D. LuffyzNo ratings yet
- Pediatric Drug Doses PDFDocument8 pagesPediatric Drug Doses PDFSaqlain Haider 19No ratings yet
- Paediatric DoseDocument12 pagesPaediatric DoseYohanes AdiputraNo ratings yet
- جرعات الاطفالDocument50 pagesجرعات الاطفالWael Hamdy100% (1)
- Anesthesiology Quick Reference (Adult) : Intubating MaintenanceDocument2 pagesAnesthesiology Quick Reference (Adult) : Intubating Maintenanceanestesi unpadNo ratings yet
- Dka CalculatorDocument1 pageDka CalculatorTalib AdilNo ratings yet
- Recommended Dosage For DrugsDocument2 pagesRecommended Dosage For DrugsJohn Christopher LucesNo ratings yet
- Paediatric Drug Chart CalculatorDocument3 pagesPaediatric Drug Chart CalculatorgregraynerNo ratings yet
- Episode 86 - HyperkalemiaDocument7 pagesEpisode 86 - HyperkalemiaAlok yadav100% (1)
- Pedia 2Document4 pagesPedia 2John Christopher LucesNo ratings yet
- Actual Weight in Kgs OR Age in Years (Min 1)Document3 pagesActual Weight in Kgs OR Age in Years (Min 1)not here 2make friends sorryNo ratings yet
- AnafilaxisDocument1 pageAnafilaxisalkutbiNo ratings yet
- Anapost1 PDFDocument1 pageAnapost1 PDFIvana Vučić KlarićNo ratings yet
- 01 - Management of Critically Ill ChildrenDocument42 pages01 - Management of Critically Ill ChildrenMin MinTheinNo ratings yet
- Postgraduate Funding Information 2022/23: Graeme Fraser - Student Welfare AdviserDocument23 pagesPostgraduate Funding Information 2022/23: Graeme Fraser - Student Welfare Adviserمحمداحمد محمدنور ابايزيدNo ratings yet
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocument18 pagesWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNo ratings yet
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocument18 pagesWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNo ratings yet
- 2014 Oman Heart Association Guidelines For The Management of HypertensionDocument28 pages2014 Oman Heart Association Guidelines For The Management of Hypertensionمحمداحمد محمدنور ابايزيدNo ratings yet
- Red Eye: by DR Shihab.A.BabekerDocument7 pagesRed Eye: by DR Shihab.A.Babekerمحمداحمد محمدنور ابايزيدNo ratings yet
- SZPDocument11 pagesSZPمحمداحمد محمدنور ابايزيدNo ratings yet
- MTT Assay To Evaluate The Cytotoxic Potential of A DrugDocument5 pagesMTT Assay To Evaluate The Cytotoxic Potential of A DrugThanh KieuNo ratings yet
- William Gann Method PDFDocument1 pageWilliam Gann Method PDFchandra widjajaNo ratings yet
- Support/downloads or Scan Above QR Code For Detailed Policy WordingDocument10 pagesSupport/downloads or Scan Above QR Code For Detailed Policy Wordingraj VenkateshNo ratings yet
- Paul CooksDocument4 pagesPaul CooksMicNo ratings yet
- UntitledDocument5 pagesUntitledGerard Phoenix MaximoNo ratings yet
- Partnership in Class Questions 2015Document3 pagesPartnership in Class Questions 2015Nella KingNo ratings yet
- OptiMix - Manual - EN - Rev.03.05 (Mixer)Document89 pagesOptiMix - Manual - EN - Rev.03.05 (Mixer)Đức Nguyễn100% (2)
- GraphsDocument18 pagesGraphssaloniNo ratings yet
- RailTel Annual Report For Web-CompressedDocument228 pagesRailTel Annual Report For Web-CompressedAmit SahooNo ratings yet
- SPB ClientDocument4 pagesSPB ClientRKNo ratings yet
- ENGR387 Mini Project Code Kayra 67425975Document8 pagesENGR387 Mini Project Code Kayra 67425975capturemrahNo ratings yet
- Agile TestingDocument5 pagesAgile TestingAman YadavNo ratings yet
- Getting Started With Nuvoton NUC140 32-Bit ARM Cortex-M0 Microcontroller PDFDocument7 pagesGetting Started With Nuvoton NUC140 32-Bit ARM Cortex-M0 Microcontroller PDFoktaNo ratings yet
- Ged Test Accom App AdhdDocument7 pagesGed Test Accom App AdhdJeannette DorfmanNo ratings yet
- Edc 2Document103 pagesEdc 2abhi_engg06No ratings yet
- Sandy Point Brochure 2016Document7 pagesSandy Point Brochure 2016miller999No ratings yet
- Z19 Tnoo 000517 PDFDocument1 pageZ19 Tnoo 000517 PDFGuna RajNo ratings yet
- Power Electronics ProjectDocument38 pagesPower Electronics Projectvishwatheja198950% (2)
- MT2OL-Ia6 2 1Document136 pagesMT2OL-Ia6 2 1QUILIOPE, JUSTINE JAY S.No ratings yet
- Soc TB 25 May 2017Document37 pagesSoc TB 25 May 2017Ipie BsaNo ratings yet
- SPECALOG Hitachi Ex2600-6Document7 pagesSPECALOG Hitachi Ex2600-6andrefilthNo ratings yet
- BitBox CarList 2022 10 28Document97 pagesBitBox CarList 2022 10 28marcos hernandezNo ratings yet
- Laboratorium Pengujian Teknik Sipil Universitas Bandar LampungDocument1 pageLaboratorium Pengujian Teknik Sipil Universitas Bandar LampungPanji OctaWirawanNo ratings yet
- Action ResearchDocument10 pagesAction ResearchNacion EstefanieNo ratings yet
- Vol-37 Let's Eat! MagazineDocument80 pagesVol-37 Let's Eat! MagazineLetseatmagNo ratings yet
- Unhappy Meals - Michael Pollan - The New York TimesDocument25 pagesUnhappy Meals - Michael Pollan - The New York TimesBob0% (1)
- 38 Parasrampuria Synthetics LTD 20 Sot 248Document5 pages38 Parasrampuria Synthetics LTD 20 Sot 248Chanakya ReddyNo ratings yet
- Activity Sheets Signal WordsDocument15 pagesActivity Sheets Signal WordsGrace Ann EscabarteNo ratings yet
- Fallas VenezuelaDocument20 pagesFallas VenezuelaDaniel Quintana GaviriaNo ratings yet
- Free CV Template 31Document1 pageFree CV Template 31Aaron WilsonNo ratings yet