Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Microbiology Experiments A Health Science Perspective 10Th Edition John Kleyn Online Ebook Texxtbook Full Chapter PDFDocument69 pagesMicrobiology Experiments A Health Science Perspective 10Th Edition John Kleyn Online Ebook Texxtbook Full Chapter PDFmargaret.lavergne883100% (10)
- Download: Natures Law: The Secret of The Universe (Elliott Wave)Document3 pagesDownload: Natures Law: The Secret of The Universe (Elliott Wave)hariganesh3750% (12)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2 21 PDX and Organoids Model Therapy Response in Prostate CancerDocument13 pages2 21 PDX and Organoids Model Therapy Response in Prostate CancerShuang LiNo ratings yet
- PCa 20 EU Prostate Cancer IncidenceDocument15 pagesPCa 20 EU Prostate Cancer IncidenceShuang LiNo ratings yet
- 0 SREBF1 AR:MTOR Nuclear Axis in Prostate CancerDocument11 pages0 SREBF1 AR:MTOR Nuclear Axis in Prostate CancerShuang LiNo ratings yet
- 3 Nature Rapalink-1Document28 pages3 Nature Rapalink-1Shuang LiNo ratings yet
- Reactivation ARDocument12 pagesReactivation ARShuang LiNo ratings yet
- Modeling Heterogeneity 2022Document12 pagesModeling Heterogeneity 2022Shuang LiNo ratings yet
- LNCaP and C4-2B Transcriptomic AnalysesDocument8 pagesLNCaP and C4-2B Transcriptomic AnalysesShuang LiNo ratings yet
- Rob - Report 41+508 - 01.02.2016Document13 pagesRob - Report 41+508 - 01.02.2016vivekNo ratings yet
- The Hunger Level Scale: 3. Think About Other Reasons You May Want To EatDocument3 pagesThe Hunger Level Scale: 3. Think About Other Reasons You May Want To EatA Puffin LekvárNo ratings yet
- User Analysis SampleDocument8 pagesUser Analysis Samplecece vergieNo ratings yet
- Laughter Is Best Essay OtherDocument2 pagesLaughter Is Best Essay OtherArchana SharmaNo ratings yet
- Non Ferrous Tpu 10Document49 pagesNon Ferrous Tpu 10natan anandaNo ratings yet
- Unit 7 - Assignment - Fictional CharactersDocument6 pagesUnit 7 - Assignment - Fictional Charactersapi-493788043No ratings yet
- High-Speed Twin-Roll Strip Casting of Al-Mg-Si Alloys With High Iron ContentDocument7 pagesHigh-Speed Twin-Roll Strip Casting of Al-Mg-Si Alloys With High Iron ContentVidya me20d015No ratings yet
- Lect2 Anes Drugs PDFDocument109 pagesLect2 Anes Drugs PDFJidapa SEELADEENo ratings yet
- Complete ABB BA Solutions 2018Document123 pagesComplete ABB BA Solutions 2018Ayoub DjemaciNo ratings yet
- Unlad Kabataan Program (Ukp) : Guidelines in The Implementation ofDocument37 pagesUnlad Kabataan Program (Ukp) : Guidelines in The Implementation ofRabhak Khal-Hadjj100% (12)
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- CDS57006 Bosch LSU 4.9 Sensor PDFDocument4 pagesCDS57006 Bosch LSU 4.9 Sensor PDFAnonymous K3FaYFlNo ratings yet
- (Class 6) Fun With Magnets & Seperation of SubstancesDocument4 pages(Class 6) Fun With Magnets & Seperation of SubstancesSnigdha GoelNo ratings yet
- Case Study3-FitbitDocument11 pagesCase Study3-FitbitKwai Fong PANGNo ratings yet
- Pipeline Defect Repair MethodsDocument20 pagesPipeline Defect Repair MethodsAyon RoyNo ratings yet
- Performance Appraisal SystemDocument13 pagesPerformance Appraisal SystemAli AsgarNo ratings yet
- TỔNG HỢP CÁC ĐỀ CHUYÊN ANH QUỐC HỌC CÁC NĂMDocument61 pagesTỔNG HỢP CÁC ĐỀ CHUYÊN ANH QUỐC HỌC CÁC NĂMLan Phong TranNo ratings yet
- Elecrolysis Cell DrawingDocument2 pagesElecrolysis Cell DrawingRimaNo ratings yet
- 5V6 DiodeDocument5 pages5V6 DiodeAchmad Rifdatul HisanNo ratings yet
- 2011 Douglas County Fair - Schedule of EventsDocument3 pages2011 Douglas County Fair - Schedule of EventsNews-Review of Roseburg OregonNo ratings yet
- Week 7 - Rheumatoid ArthritisDocument1 pageWeek 7 - Rheumatoid ArthritisTuTitNo ratings yet
- Chapter 6 Hexavalent ChromiumDocument56 pagesChapter 6 Hexavalent Chromiumgabriel100% (1)
- Breast Cancer TCM 2Document5 pagesBreast Cancer TCM 2Ivonne Flores FernándezNo ratings yet
- People vs. Sy PioDocument3 pagesPeople vs. Sy PioPrincessAngelaDeLeon100% (2)
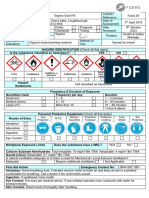
- 07 Gyproc Eas-Fill COSHH Ass'tDocument2 pages07 Gyproc Eas-Fill COSHH Ass'tphil.jacksonNo ratings yet
- BasuhTanganDenganBetul BIDocument1 pageBasuhTanganDenganBetul BIAdnan ShamsudinNo ratings yet
- GlyphosateDocument7 pagesGlyphosateantonio leonNo ratings yet
- Business Plan AbmDocument42 pagesBusiness Plan AbmMikaela MassalangNo ratings yet