Download as doc, pdf, or txt
You might also like
- Advanced Practice Nursing in The Care of Older Adults 7th Ed. by Malone Plank Duffy PDFDocument542 pagesAdvanced Practice Nursing in The Care of Older Adults 7th Ed. by Malone Plank Duffy PDFJeMalyn VieRnes100% (6)
- Nursing Midwifery Staff CBAHI QuestionsDocument13 pagesNursing Midwifery Staff CBAHI QuestionsnasserjubranNo ratings yet
- Hand HyegieneDocument60 pagesHand HyegieneckNo ratings yet
- Infection Control Checklist Nursing DepartmentDocument5 pagesInfection Control Checklist Nursing DepartmentKhaskheli NusratNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- General Principles of Geriatric RehabilitationDocument5 pagesGeneral Principles of Geriatric RehabilitationPraneetha Nouduri100% (2)
- End of Life CareDocument14 pagesEnd of Life Careapi-680119126No ratings yet
- CSSD Performance Quality Analysis at A Super Speciality HospitalDocument29 pagesCSSD Performance Quality Analysis at A Super Speciality HospitalD. GandhirajNo ratings yet
- How To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairDocument9 pagesHow To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairAfniy ApriliaNo ratings yet
- Checklist For CSSD For NABH Preparation and Its Quality IndicatorsDocument3 pagesChecklist For CSSD For NABH Preparation and Its Quality IndicatorsSanjay Kadam100% (1)
- RMO Assessment Form 2016Document8 pagesRMO Assessment Form 2016Tp HoangNo ratings yet
- 63 MdroDocument3 pages63 MdroerwindaNo ratings yet
- COP 8 ICU Manual - docx-PANCHAMDocument16 pagesCOP 8 ICU Manual - docx-PANCHAMSumit SardanaNo ratings yet
- International Patient Safety Goals - 24 September 2021Document43 pagesInternational Patient Safety Goals - 24 September 2021Yunus ElonNo ratings yet
- Surgical Site Marking PolicyDocument11 pagesSurgical Site Marking PolicymiraNo ratings yet
- DAILY ROUND Head NurseDocument1 pageDAILY ROUND Head NurseRao Rizwan ShakoorNo ratings yet
- Scripps Hospital Patient Visitor Policy PDFDocument2 pagesScripps Hospital Patient Visitor Policy PDFcode4saleNo ratings yet
- Admitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentDocument10 pagesAdmitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentAYO NELSONNo ratings yet
- GOI Draft-SOPs-for-Hospital-managementDocument38 pagesGOI Draft-SOPs-for-Hospital-managementksushruuthNo ratings yet
- Obtaining Valid Consent: Clinical Governance Advice No. 6Document9 pagesObtaining Valid Consent: Clinical Governance Advice No. 6Ywagar YwagarNo ratings yet
- 208-Audit Checklist-Autoclave Operation - FinalDocument6 pages208-Audit Checklist-Autoclave Operation - FinalCherry Hope MistioNo ratings yet
- Western Australian Patient Identification Policy PDFDocument14 pagesWestern Australian Patient Identification Policy PDFpuspadiniaNo ratings yet
- Hope RequirementsDocument7 pagesHope Requirementscorona virusNo ratings yet
- Missing Patients ProcedureDocument16 pagesMissing Patients ProcedureAgnieszka WaligóraNo ratings yet
- AAC 10 Standards of NabhDocument46 pagesAAC 10 Standards of NabhgmsNo ratings yet
- In - Patient Service Ward 1Document12 pagesIn - Patient Service Ward 1mitchNo ratings yet
- Apollo KH Hospital: Nursing ManualDocument2 pagesApollo KH Hospital: Nursing ManualSheela Solomon100% (2)
- Checklist IntraOperative Competency Circulating 2022Document2 pagesChecklist IntraOperative Competency Circulating 2022Russel PamaNo ratings yet
- Hospital Staffing PlanDocument1 pageHospital Staffing PlanMilin Anik'sNo ratings yet
- Who Surgical Safety ChecklistDocument12 pagesWho Surgical Safety ChecklistKit Alizon BarredoNo ratings yet
- Competency ChecklistDocument3 pagesCompetency ChecklistJon Bandola100% (2)
- E NabhDocument64 pagesE NabhRenuka Murugan100% (1)
- Nabh - HicDocument40 pagesNabh - HicShejil BalakrishnanNo ratings yet
- Ipsg 2017Document41 pagesIpsg 2017hum JavedNo ratings yet
- Policies and Procedures Manual Infection Control in General Nursing UnitDocument9 pagesPolicies and Procedures Manual Infection Control in General Nursing UnitDerick RanaNo ratings yet
- Nursing Services Manual, Aiims New Delhi - 25!2!21Document91 pagesNursing Services Manual, Aiims New Delhi - 25!2!21praveenjenaNo ratings yet
- Standardized Hospital Colour CodesDocument5 pagesStandardized Hospital Colour CodesRichard Deo R. AlaveNo ratings yet
- DamaDocument2 pagesDamajerimiah_manzon100% (1)
- Infection Control Checklist Nursing DepartmentDocument5 pagesInfection Control Checklist Nursing DepartmentNoreen PunjwaniNo ratings yet
- 2011 Newborn Care SOP 29-11-11Document95 pages2011 Newborn Care SOP 29-11-11Safiqul Islam ShawnNo ratings yet
- Nabh ChecklistDocument2 pagesNabh ChecklistJatoveda Haldar100% (1)
- Road Accidents 107 B ReportDocument2 pagesRoad Accidents 107 B ReportTrish 0019No ratings yet
- Pre and Post TestDocument3 pagesPre and Post TestNurhayatiNo ratings yet
- MedicineDocument19 pagesMedicineSarah100% (1)
- Job Responsibilities FoDocument4 pagesJob Responsibilities FoKumar BalramNo ratings yet
- 5 Labour Room Laqshya Assessment ToolkitDocument16 pages5 Labour Room Laqshya Assessment ToolkitAnjali Rahul Ajmeri50% (2)
- Clarification On Fire SafetyDocument1 pageClarification On Fire SafetyNaviin KrishnanNo ratings yet
- Improving Operating Theatre Performance Complete Step Guide Without Pic PDFDocument83 pagesImproving Operating Theatre Performance Complete Step Guide Without Pic PDFAddison RousdyNo ratings yet
- Hospital Infection Control ManualDocument59 pagesHospital Infection Control Manualابراهيم الحربيNo ratings yet
- Policies and Procedures For Sound-Alike and Look-Alike MedicationsDocument6 pagesPolicies and Procedures For Sound-Alike and Look-Alike Medicationsrelena badrNo ratings yet
- SOP For Dermatologist For DOH PuplicationDocument13 pagesSOP For Dermatologist For DOH Puplicationhitham shehataNo ratings yet
- Pre-Operative & Post-Operative Care PlansDocument4 pagesPre-Operative & Post-Operative Care PlansHal00mNo ratings yet
- Central Sterile Supply Department: Mallikarjuna MHADocument25 pagesCentral Sterile Supply Department: Mallikarjuna MHAsandhyakrishnanNo ratings yet
- 0 List of ProceduresDocument1 page0 List of ProceduresSanjay KadamNo ratings yet
- Timely Simple DischargeDocument52 pagesTimely Simple DischargeDesti Setyaningrum100% (1)
- Ngeles Niversity Oundation: College of NursingDocument2 pagesNgeles Niversity Oundation: College of NursingAllyana de JesusNo ratings yet
- Hospital Ethics HandbookDocument47 pagesHospital Ethics HandbookZiaul Haque100% (1)
- Needle Stick InjuryDocument24 pagesNeedle Stick InjuryShivani TiwariNo ratings yet
- Final HICC Manual AIIMSDocument35 pagesFinal HICC Manual AIIMSNaMakNo ratings yet
- Quality Improvement Program ON Improvement of Legibility and Appropriateness of Medication Orders in Patient RecordDocument44 pagesQuality Improvement Program ON Improvement of Legibility and Appropriateness of Medication Orders in Patient RecordNandakishore RajkumarNo ratings yet
- IPSG May28Document62 pagesIPSG May28S. Pichammal - Quality ManagerNo ratings yet
- A SepsisDocument5 pagesA SepsisAi KogaNo ratings yet
- Humana Scope of App. - 2Document2 pagesHumana Scope of App. - 2family-instituteNo ratings yet
- Standing Orders For Acute Pain NursesDocument2 pagesStanding Orders For Acute Pain NursesJerome SamuelNo ratings yet
- Iyeokan Ativie's Cover Letter 2013Document1 pageIyeokan Ativie's Cover Letter 2013Ella McAtiveNo ratings yet
- Stress and Coping Strategies Among Senior Citizen in Selected Old Age Home, BerhampurDocument5 pagesStress and Coping Strategies Among Senior Citizen in Selected Old Age Home, BerhampuramitNo ratings yet
- Icd 10Document3 pagesIcd 10boblishNo ratings yet
- St. Luke's College of Nursing: Trinity University of AsiaDocument2 pagesSt. Luke's College of Nursing: Trinity University of AsiaRalph Lorenz Avila AquinoNo ratings yet
- Normative Data For The Boston Naming Test-Spanish-2008Document7 pagesNormative Data For The Boston Naming Test-Spanish-2008SaraNo ratings yet
- 6-Cit Test PDFDocument2 pages6-Cit Test PDFnurasyikah100% (1)
- 707 Area Code FacilitiesDocument13 pages707 Area Code FacilitiesEmerson BigginsNo ratings yet
- Hospital Bed and FunctionsDocument8 pagesHospital Bed and Functionsfajri khanNo ratings yet
- Soal UAS S2 Penelitian Kuantitatif 2023-2024 - Prof. Dr. Christantie Effendy, SKP., M.KesDocument2 pagesSoal UAS S2 Penelitian Kuantitatif 2023-2024 - Prof. Dr. Christantie Effendy, SKP., M.KesNELSON VIDIGALNo ratings yet
- The Confusion Assessment Method For The ICU (CAM-ICU) : Training ManualDocument14 pagesThe Confusion Assessment Method For The ICU (CAM-ICU) : Training ManualParvathy R NairNo ratings yet
- Ambulatory Care SystemDocument7 pagesAmbulatory Care Systemkint manlangitNo ratings yet
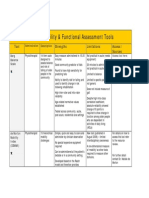
- Mobility and Functional Assessment ToolsDocument4 pagesMobility and Functional Assessment Toolssonya63265No ratings yet
- OIG VA Inspection ReportDocument84 pagesOIG VA Inspection ReportFOX59/CBS4No ratings yet
- Panti Jompo Presentation FinalizedDocument13 pagesPanti Jompo Presentation FinalizedAyu Putri AgniNo ratings yet
- CTG Classification PDFDocument1 pageCTG Classification PDFAkhmad Ikhsan Prafita PutraNo ratings yet
- Speech Language Pathology: Background and NatureDocument8 pagesSpeech Language Pathology: Background and NatureNikki Nina Arabe BarcinasNo ratings yet
- Marija Lapkus CV 2020 3Document9 pagesMarija Lapkus CV 2020 3api-536839399No ratings yet
- Physical Therapy BrochureDocument2 pagesPhysical Therapy Brochureapi-491457391No ratings yet
- Resources in Egypt For Geriatrics CareDocument52 pagesResources in Egypt For Geriatrics CareDoha Ebed100% (2)
- The New Philippine Geriatric Center: A Proposed Resort-Oriented Geriatric Health Complex Towards Optimistic and Holistic ArchitectureDocument2 pagesThe New Philippine Geriatric Center: A Proposed Resort-Oriented Geriatric Health Complex Towards Optimistic and Holistic ArchitectureCindy RatificadoNo ratings yet
- International Case Study of Assisted Living For The ElderlyDocument27 pagesInternational Case Study of Assisted Living For The ElderlyArathi Suresh100% (2)
- 13B Week 1 NRG 303 Trends and IssuesDocument7 pages13B Week 1 NRG 303 Trends and IssuesERAN MARK ROJASNo ratings yet
- Geriatric MonikaDocument74 pagesGeriatric MonikaKrishnaveni MurugeshNo ratings yet
- Approval LetterDocument4 pagesApproval LetterRoger RanigoNo ratings yet
- International Association For Promotion of Healthcare and Life-Science Research (Iaphlsr)Document23 pagesInternational Association For Promotion of Healthcare and Life-Science Research (Iaphlsr)Global Research and Development ServicesNo ratings yet
- Direction: Kurnihayati, M.PDDocument28 pagesDirection: Kurnihayati, M.PDKurnihayati MuklasNo ratings yet