Download as pdf or txt
You might also like
- Dr. Bielers Natural Way To Sexual HealthDocument264 pagesDr. Bielers Natural Way To Sexual Healthed-o85% (13)
- Harare - Essential Guide To Management of Common Obstetric and GynaecologicDocument98 pagesHarare - Essential Guide To Management of Common Obstetric and GynaecologicTapiwa Munikwa100% (5)
- Elsevier Introduction To Maternity and Pediatric Nursing NCLEX Review Answers Chapter 004Document2 pagesElsevier Introduction To Maternity and Pediatric Nursing NCLEX Review Answers Chapter 004SamNo ratings yet
- No. 29. Chronic Hypertension in PregnancyDocument9 pagesNo. 29. Chronic Hypertension in Pregnancyrolla_hiraNo ratings yet
- Hypertension During PregnancyDocument9 pagesHypertension During PregnancyNera MayaditaNo ratings yet
- Treatment of Mild Chronic Hypertension During PregnancyDocument12 pagesTreatment of Mild Chronic Hypertension During PregnancyChioma AnowaiNo ratings yet
- Kidney News Article p29 17Document1 pageKidney News Article p29 17annafebrinaputriNo ratings yet
- Drug Treatment of Hypertension in PregnancyDocument15 pagesDrug Treatment of Hypertension in PregnancytetriNo ratings yet
- Differentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyDocument6 pagesDifferentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyVera Gardasevic MitrovicNo ratings yet
- Hypertension KehamilanDocument10 pagesHypertension Kehamilanmiss betawiNo ratings yet
- Management of HypertensionDocument6 pagesManagement of HypertensionRioNo ratings yet
- Jurnal Eveidence Based'Document6 pagesJurnal Eveidence Based'chaeworldNo ratings yet
- The Management of Hypertension in Women Planning For PregnancyDocument10 pagesThe Management of Hypertension in Women Planning For PregnancyRadinal PrayitnoNo ratings yet
- Pi Is 0002937822002836Document4 pagesPi Is 0002937822002836Resta PrimastiNo ratings yet
- Paguidian, Griffin John D. Bsn4ADocument10 pagesPaguidian, Griffin John D. Bsn4AGj PaguidianNo ratings yet
- Andrea Surányi, Ábel Altorjay, László Kaiser, Tibor Nyári, Gábor NémethDocument9 pagesAndrea Surányi, Ábel Altorjay, László Kaiser, Tibor Nyári, Gábor NémethfujimeisterNo ratings yet
- Haematocrit Value in Preeclampsia: AbstractDocument6 pagesHaematocrit Value in Preeclampsia: AbstractViraj SenavirathneNo ratings yet
- Pathophysiology and Medical Management of Systemic Hypertension in PregnancyDocument11 pagesPathophysiology and Medical Management of Systemic Hypertension in Pregnancydr faathirNo ratings yet
- Anti HipertesiDocument8 pagesAnti HipertesiLuana Junia BunarliNo ratings yet
- 1 PBDocument4 pages1 PBkadek sanggingNo ratings yet
- Determinants of Preeclampsia in Women With Type 1 DiabetesDocument7 pagesDeterminants of Preeclampsia in Women With Type 1 DiabetesSEPTIASIHNo ratings yet
- Chronic Hypertension and Superimposed PreeclampsiaDocument14 pagesChronic Hypertension and Superimposed PreeclampsiaBelen HerreraNo ratings yet
- Managing Post Partum HypertensionDocument10 pagesManaging Post Partum HypertensionDendyNo ratings yet
- High Blood Pressure During Pregnancy About 544 CasesDocument21 pagesHigh Blood Pressure During Pregnancy About 544 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Summary of The NHLBI Working Group On Research On Hypertension During PregnancyDocument9 pagesSummary of The NHLBI Working Group On Research On Hypertension During PregnancycarlosarmijoNo ratings yet
- Jurnal Farmakoekonomi IndividuDocument13 pagesJurnal Farmakoekonomi IndividuWewi AlfareziNo ratings yet
- Hipertensión en EspañolDocument16 pagesHipertensión en EspañolErick SánchezNo ratings yet
- Consenso THAEDocument22 pagesConsenso THAEsebastian mancillaNo ratings yet
- Mechanisms and Management of Hypertension in Pregnant WomenDocument14 pagesMechanisms and Management of Hypertension in Pregnant WomenMiguel Angel Alvarado AriasNo ratings yet
- Jurnal 6Document8 pagesJurnal 6Bayek NgekekNo ratings yet
- J of Clinical Hypertension - 2007 - Moser - Working Group Report On High Blood Pressure in PregnancyDocument14 pagesJ of Clinical Hypertension - 2007 - Moser - Working Group Report On High Blood Pressure in PregnancycarlosarmijoNo ratings yet
- Best Practices For Managing Postpartum HypertensionDocument10 pagesBest Practices For Managing Postpartum HypertensionYhogerlys LucenaNo ratings yet
- Jurnal 3Document8 pagesJurnal 3Hana Nuraisa BasyaNo ratings yet
- ISSHP Classification of Hypertensive Disorders of Pregnancy 2014Document8 pagesISSHP Classification of Hypertensive Disorders of Pregnancy 2014Firah Triple'sNo ratings yet
- Chips Trial ReferenceDocument11 pagesChips Trial ReferenceDr.Nilar WinNo ratings yet
- 1 s2.0 S2210778919304714 MainDocument6 pages1 s2.0 S2210778919304714 MainsandrakucabaNo ratings yet
- Firoz Et Al-2014-BJOG - An International Journal of Obstetrics & GynaecologyDocument9 pagesFiroz Et Al-2014-BJOG - An International Journal of Obstetrics & GynaecologyImelda AtikaNo ratings yet
- Hypertensive Disorders of Pregnancy - ReviewDocument16 pagesHypertensive Disorders of Pregnancy - Reviewsafa HADFINo ratings yet
- Healthcare: Antihypertensive Medications For Severe Hypertension in Pregnancy: A Systematic Review and Meta-AnalysisDocument22 pagesHealthcare: Antihypertensive Medications For Severe Hypertension in Pregnancy: A Systematic Review and Meta-AnalysismartinNo ratings yet
- Consenso SHAE ACOG 2000Document22 pagesConsenso SHAE ACOG 2000Sergio Andrés Flórez VelásquezNo ratings yet
- Jurnal CohortDocument21 pagesJurnal CohortAstri Anindita UtomoNo ratings yet
- Association Between Intrahepatic Cholestasis in Pregnancy and Gestational Diabetes Mellitus. A Retrospective AnalysisDocument6 pagesAssociation Between Intrahepatic Cholestasis in Pregnancy and Gestational Diabetes Mellitus. A Retrospective AnalysisDr.Karima EldarhobiNo ratings yet
- The CHIPS Randomized Controlled Trial (Control of Hypertension in Pregnancy Study)Document7 pagesThe CHIPS Randomized Controlled Trial (Control of Hypertension in Pregnancy Study)fitriNo ratings yet
- 2016 Management of Severe Hypertension in PregnancyDocument7 pages2016 Management of Severe Hypertension in PregnancyMaria del Pilar Devis MoralesNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument6 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyfujimeisterNo ratings yet
- Management of Severe Hypertension in PregnancyDocument7 pagesManagement of Severe Hypertension in PregnancyAnastasia RiuneszveNo ratings yet
- Impact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboDocument8 pagesImpact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboPramatama AndhikaNo ratings yet
- Regional Anesthesia in Patients With Pregnancy Induced HypertensionDocument10 pagesRegional Anesthesia in Patients With Pregnancy Induced HypertensionEdo GeradNo ratings yet
- 10.1016@j.bjae.2020.07.007 2Document6 pages10.1016@j.bjae.2020.07.007 2atikaNo ratings yet
- JGWH - Ms.id.555623 1 KirimDocument6 pagesJGWH - Ms.id.555623 1 KirimBaiq Bunga Citra PratiwiNo ratings yet
- Bahan Chronic HypertensionDocument13 pagesBahan Chronic HypertensionMuhammad NazliNo ratings yet
- Antepartum and Postpartum Uterine ArteryDocument7 pagesAntepartum and Postpartum Uterine ArterypaolabriglimNo ratings yet
- Association Between Hypertensive Disorders of Pregnancy and Later Risk of CardiomyopathyDocument8 pagesAssociation Between Hypertensive Disorders of Pregnancy and Later Risk of CardiomyopathyPujiyono SuwadiNo ratings yet
- Jurnal Dila 1Document15 pagesJurnal Dila 1Kiki Celiana TiffanyNo ratings yet
- J of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaDocument5 pagesJ of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaDefi SelvianitaNo ratings yet
- Hipertension en El EmbarazoDocument12 pagesHipertension en El EmbarazofsitoNo ratings yet
- Influence of Maternal and Perinatal Characteristics On Risk of Postpartum Chronic Hypertension After Pre-EclampsiaDocument17 pagesInfluence of Maternal and Perinatal Characteristics On Risk of Postpartum Chronic Hypertension After Pre-EclampsiadinaNo ratings yet
- Pregnancy Hypertension: SciencedirectDocument7 pagesPregnancy Hypertension: Sciencedirectdds (TMU)No ratings yet
- First-Trimester Prediction of Gestational Hypertension Through The Bioelectrical Impedance Analysis of The Body CompositionDocument6 pagesFirst-Trimester Prediction of Gestational Hypertension Through The Bioelectrical Impedance Analysis of The Body Compositionppdsobginunsrijan23No ratings yet
- HEG in NorwayDocument6 pagesHEG in NorwayDian Laras SuminarNo ratings yet
- NIH Public Access: The Management of Hypertension in PregnancyDocument20 pagesNIH Public Access: The Management of Hypertension in PregnancymeliabudiNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
- Radiolgy IlustratedDocument596 pagesRadiolgy IlustratedAli CiaNo ratings yet
- ENG-PM-iM8 Series-V2.5-20190611Document2 pagesENG-PM-iM8 Series-V2.5-20190611modki27No ratings yet
- Management of Pre - EclampsiaDocument22 pagesManagement of Pre - Eclampsiaapi-3705046No ratings yet
- Basic Principle and Step-by-Step Procedure of Abdominal Hysterectomy: Part 2Document11 pagesBasic Principle and Step-by-Step Procedure of Abdominal Hysterectomy: Part 2Made SuryaNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- Forearm Fractures PDFDocument4 pagesForearm Fractures PDFNur Ashriawati BurhanNo ratings yet
- NO 2. Triphasic Computed Tomography (CT) Scan in Focal Tumoral Liver Le-1Document7 pagesNO 2. Triphasic Computed Tomography (CT) Scan in Focal Tumoral Liver Le-1hermanusNo ratings yet
- Chapter 22 The First Heart SoundDocument5 pagesChapter 22 The First Heart SoundAbhilash ReddyNo ratings yet
- Medical Education in South East Asia Current Trend and Malaysia's PerspectiveDocument4 pagesMedical Education in South East Asia Current Trend and Malaysia's PerspectiveRiry AmbarsaryNo ratings yet
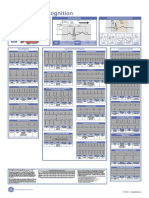
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- Biophysical AssessmentDocument9 pagesBiophysical AssessmentSanjeev NambalateNo ratings yet
- Up-To-Date at The Age of Implant Dentistry: VestibuloplastyDocument3 pagesUp-To-Date at The Age of Implant Dentistry: VestibuloplastyDemmy WijayaNo ratings yet
- Btl-Physio Cat En202Document56 pagesBtl-Physio Cat En202avaNo ratings yet
- PGY 1 Survival Guide MICU 1Document3 pagesPGY 1 Survival Guide MICU 1Abdulelah MurshidNo ratings yet
- ENGLISH FOR MIDWIFE UNIT 1 I Will Become A MidwifeDocument2 pagesENGLISH FOR MIDWIFE UNIT 1 I Will Become A MidwifeDestyana ArabelNo ratings yet
- Milobar Alexus Resume MayoDocument2 pagesMilobar Alexus Resume Mayoapi-338646789No ratings yet
- WHO MPS 10.1 Participants Workbook EngDocument164 pagesWHO MPS 10.1 Participants Workbook EngTri Ari dityaNo ratings yet
- PDF Obgyn Secrets 4Th Edition Amanda Mularz Ebook Full ChapterDocument53 pagesPDF Obgyn Secrets 4Th Edition Amanda Mularz Ebook Full Chapterrichard.heinz235100% (1)
- Hospital Follow Up Progress Note MedicalTemplateDocument1 pageHospital Follow Up Progress Note MedicalTemplatee-MedTools100% (18)
- Guerrilla Girls - HysteriaDocument14 pagesGuerrilla Girls - Hysteriagattita07No ratings yet
- The Physiological Mechanism of Uterine Contraction With Emphasis On Calcium IonDocument6 pagesThe Physiological Mechanism of Uterine Contraction With Emphasis On Calcium IonpolygoneNo ratings yet
- Femto Vs Phaco 2Document6 pagesFemto Vs Phaco 2Bonita AsyigahNo ratings yet
- 2010.08.10 Ancls Int For PrintDocument12 pages2010.08.10 Ancls Int For PrintMuhamad ZakyNo ratings yet
- Transversus Abdominis Plane (Tap) BlockDocument6 pagesTransversus Abdominis Plane (Tap) BlockSuresh KumarNo ratings yet
- Med Surg Concept Map Clinical Make UpDocument6 pagesMed Surg Concept Map Clinical Make UpColin MillerNo ratings yet
- Laparoscopic Abdominoperineal ResectionDocument19 pagesLaparoscopic Abdominoperineal ResectionJohnson Mallibago100% (2)
- Magnetic Resonance Imaging of Male and Female Genitals During Coitus and Female Sexual ArousalDocument6 pagesMagnetic Resonance Imaging of Male and Female Genitals During Coitus and Female Sexual Arousalapi-3738541100% (1)