Download as pdf or txt
You might also like
- Essential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi ArabiaDocument36 pagesEssential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi Arabiarelena badr100% (1)
- Cooling Tower and Chiller Cleaning ProceduresDocument4 pagesCooling Tower and Chiller Cleaning ProceduresAndeska Pratama100% (2)
- Indikasi, Teknik Pembuatan Stoma, ReanastomosispptDocument43 pagesIndikasi, Teknik Pembuatan Stoma, ReanastomosispptErwin Aritama Ismail100% (1)
- Treatment of Adhesive Capsulitis of The Shoulder-1Document12 pagesTreatment of Adhesive Capsulitis of The Shoulder-1JONATHAN IVANNo ratings yet
- Frozen Shoulder5B15DDocument15 pagesFrozen Shoulder5B15DTri Ayu AstutiNo ratings yet
- 0 1 The Pathophysiology of Shoulder Instability 2800953368Document8 pages0 1 The Pathophysiology of Shoulder Instability 2800953368César ArveláezNo ratings yet
- Coccygectomy: April 2015Document7 pagesCoccygectomy: April 2015Waeel HamoudaNo ratings yet
- Whiplash Associated DisordersDocument12 pagesWhiplash Associated DisorderspuchioNo ratings yet
- Long Head of The Biceps Tendinopathy Diagnosis and ManagementDocument12 pagesLong Head of The Biceps Tendinopathy Diagnosis and ManagementJUAN MANUEL MOSQUERA FERNANDEZ DE CASTRONo ratings yet
- Frozen ShoulderDocument10 pagesFrozen Shoulderrifa fasyiaNo ratings yet
- Empowering The Path From Stiffness To Recovery in Adhesive Shoulder Capsulitis ComplexityDocument10 pagesEmpowering The Path From Stiffness To Recovery in Adhesive Shoulder Capsulitis ComplexityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Recovery With Posterior Decompression and Dural Suturing 2024 InternationalDocument5 pagesRecovery With Posterior Decompression and Dural Suturing 2024 InternationalRonald QuezadaNo ratings yet
- 618 FullDocument11 pages618 Fulleric22hkNo ratings yet
- Treatment of Central Cord Syndrome Without Associated Spinal InstabilityDocument5 pagesTreatment of Central Cord Syndrome Without Associated Spinal Instabilityfori:=1tondoNo ratings yet
- Physiotherapy of Adhesive Capsulitis: A Review: Kaushik GuhaDocument5 pagesPhysiotherapy of Adhesive Capsulitis: A Review: Kaushik GuhaVeby JabirNo ratings yet
- NIH Public Access: Author ManuscriptDocument26 pagesNIH Public Access: Author ManuscriptEma DanciuNo ratings yet
- Capsulitis Adhesiva PDFDocument14 pagesCapsulitis Adhesiva PDFErika LópezNo ratings yet
- 2017 Article 9386 TendinitisDocument9 pages2017 Article 9386 TendinitisKirana lupitaNo ratings yet
- 1 s2.0 S2589514122001001 MainDocument14 pages1 s2.0 S2589514122001001 MainAnkur RastogiNo ratings yet
- 1 s2.0 S1836955322000893 MainDocument17 pages1 s2.0 S1836955322000893 Mainnikhilmascarenhas07No ratings yet
- Paper 5Document8 pagesPaper 5Francisco Javier Luza RamosNo ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- Pre-Hospital Spinal Immobilisation - An Initial Consensus StatementDocument4 pagesPre-Hospital Spinal Immobilisation - An Initial Consensus StatementJade OttoniNo ratings yet
- Rotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Document6 pagesRotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Rilind ShalaNo ratings yet
- Achilles 1Document9 pagesAchilles 1diretoriacmbaNo ratings yet
- Adhesive CapsulitisDocument10 pagesAdhesive CapsulitisGumDropNo ratings yet
- Rotator Cuff Tendinopathy:subacromial Impingement Syndrome - Is It Time For A New Method of Assessment?Document6 pagesRotator Cuff Tendinopathy:subacromial Impingement Syndrome - Is It Time For A New Method of Assessment?杨钦杰No ratings yet
- Rotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Document7 pagesRotator Cuff Tendinopathy/subacromial Impingement Syndrome: Is It Time For A New Method of Assessment?Abdul Wahid ShaikhNo ratings yet
- Rotator Cuff Lesions: A Case ReportDocument8 pagesRotator Cuff Lesions: A Case ReportUbaidillah Romadlon AlfairuziNo ratings yet
- 1108 ShoulderDocument5 pages1108 ShoulderMilton RezzaNo ratings yet
- Grupo 2 Current Trends in Anterior Cruciate Ligament Reconstruction 1 378755938Document10 pagesGrupo 2 Current Trends in Anterior Cruciate Ligament Reconstruction 1 378755938eduacv2No ratings yet
- Nerve Entrapment - UpdateDocument17 pagesNerve Entrapment - UpdatealobrienNo ratings yet
- Marrez 2013 - Supraspinatus Rotator Cuff Muscle Testing 315-Article Text-311-1-10-20140612Document7 pagesMarrez 2013 - Supraspinatus Rotator Cuff Muscle Testing 315-Article Text-311-1-10-20140612Ikhsan JohnsonNo ratings yet
- Diagnosis and Management of Adhesive CapsulitisDocument10 pagesDiagnosis and Management of Adhesive CapsulitisCarlos Martín De RosasNo ratings yet
- Physical Examination of The Shoulder: Key WordsDocument10 pagesPhysical Examination of The Shoulder: Key WordsJavi LiraNo ratings yet
- To Identify The Spectrum of Post Operative Complications and Appropriate Management in Polytraumatised Patients With Musculoskeletal InjuriesDocument4 pagesTo Identify The Spectrum of Post Operative Complications and Appropriate Management in Polytraumatised Patients With Musculoskeletal InjuriesShaneed KpNo ratings yet
- Complex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDDocument14 pagesComplex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDAndrea Z MilanoNo ratings yet
- SHOULDER INSTABILITY ManagDocument18 pagesSHOULDER INSTABILITY ManagFarhan JustisiaNo ratings yet
- Yanxi Liu, MD, Zhan Zhang, MD, Jiangbo Wang, MD, Guangzhi Wu, MD, Wei Yu, MD, and Shusen Cui, MDDocument11 pagesYanxi Liu, MD, Zhan Zhang, MD, Jiangbo Wang, MD, Guangzhi Wu, MD, Wei Yu, MD, and Shusen Cui, MDGeorgios StathisNo ratings yet
- Cystic Hy GromaDocument3 pagesCystic Hy GromaAhsan JamilNo ratings yet
- Left Ventricular Volume Reduction: HistoryDocument6 pagesLeft Ventricular Volume Reduction: HistoryPeter Paul PascualNo ratings yet
- Management of Chronic Unreduced Anterior Dislocations of The Shoulder: Case Series of 53 PatientsDocument7 pagesManagement of Chronic Unreduced Anterior Dislocations of The Shoulder: Case Series of 53 PatientsOtman BenabdallahNo ratings yet
- Pitch-Side Management of Acute Shoulder Dislocations: A Conceptual ReviewDocument9 pagesPitch-Side Management of Acute Shoulder Dislocations: A Conceptual ReviewElan R.S.No ratings yet
- Pi Is 0003999308015530Document19 pagesPi Is 0003999308015530Ireng PramanaNo ratings yet
- The History of Clinical Musculoskeletal RadiologyDocument8 pagesThe History of Clinical Musculoskeletal RadiologyVALENTINA LOPEZ MARINNo ratings yet
- Guideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementDocument4 pagesGuideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementTriz BeaNo ratings yet
- Tendinopathy Continuum 2008 (Cook & Purdam)Document8 pagesTendinopathy Continuum 2008 (Cook & Purdam)nsboyadzhievNo ratings yet
- Clinical Tests of The Shoulder: Accuracy and Extension Using Dynamic UltrasoundDocument9 pagesClinical Tests of The Shoulder: Accuracy and Extension Using Dynamic UltrasoundMohammad Al AbdullaNo ratings yet
- Cystic Lesions of The Brain A Classification Based On PathogenesisDocument16 pagesCystic Lesions of The Brain A Classification Based On Pathogenesisveerraju tvNo ratings yet
- Intervalo de Los Rotadores PDFDocument10 pagesIntervalo de Los Rotadores PDFdiegovirusNo ratings yet
- PRM2020 6965381Document9 pagesPRM2020 6965381zoreNo ratings yet
- Cools 2008 Screening The Athletes Shoulder ForDocument9 pagesCools 2008 Screening The Athletes Shoulder ForLucyFloresNo ratings yet
- Subacromial Impingement Syndrome: Review ArticleDocument8 pagesSubacromial Impingement Syndrome: Review ArticleshewaleakhileshNo ratings yet
- Gimblett1999 PDFDocument6 pagesGimblett1999 PDFEleana HurtadoNo ratings yet
- Int J Sports Phys Ther 2014 9 (2) 274Document15 pagesInt J Sports Phys Ther 2014 9 (2) 274Lucas MaggiNo ratings yet
- Pressure SoresDocument43 pagesPressure SoresArpanpatelNo ratings yet
- Aneurysmal Bone Cyst: Review ArticleDocument9 pagesAneurysmal Bone Cyst: Review ArticleJeyachandran MariappanNo ratings yet
- Rotator Cuff TendinopathyDocument7 pagesRotator Cuff TendinopathyMarcus Dos SantosNo ratings yet
- Rehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewDocument10 pagesRehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewEduardo Santana SuárezNo ratings yet
- ASSESSING SHOCK RESUSCITATION STRATEGIES BY OXYGEN DEBT REPAYMENT Robert Wayne Barbee 2010Document10 pagesASSESSING SHOCK RESUSCITATION STRATEGIES BY OXYGEN DEBT REPAYMENT Robert Wayne Barbee 2010Mara TorrealbaNo ratings yet
- PTJ 0357Document19 pagesPTJ 0357Jose JuniorNo ratings yet
- Case Report Embolic Shotgun Pellet To The Righ 2024 International JournalDocument5 pagesCase Report Embolic Shotgun Pellet To The Righ 2024 International JournalRonald QuezadaNo ratings yet
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- Xiao 2016Document13 pagesXiao 2016Shiba MiyukiNo ratings yet
- Frozen Shoulder JurnalDocument11 pagesFrozen Shoulder JurnalShiba MiyukiNo ratings yet
- Frozen Shoulder JurnalDocument10 pagesFrozen Shoulder JurnalShiba MiyukiNo ratings yet
- The Gift of Pearls: ScriptDocument5 pagesThe Gift of Pearls: ScriptShiba MiyukiNo ratings yet
- Overview of Public Health-Part 2Document44 pagesOverview of Public Health-Part 2omegasauronNo ratings yet
- Lumbar Canal Stenosis: Start With Nonsurgical Therapy: ReviewDocument9 pagesLumbar Canal Stenosis: Start With Nonsurgical Therapy: Reviewsrinidhi2011No ratings yet
- Pharmacology and The Nursing Process Lilley 6th Edition Test BankDocument5 pagesPharmacology and The Nursing Process Lilley 6th Edition Test BankStephen Breedon100% (33)
- Brandt-Daroff Exercises: AudiologyDocument3 pagesBrandt-Daroff Exercises: AudiologyMatt XanNo ratings yet
- Nausea and Vomiting PDFDocument8 pagesNausea and Vomiting PDFRoosita Arbaane SafitriNo ratings yet
- Ferrari Et Al-2022-Nature Reviews Disease PrimersDocument20 pagesFerrari Et Al-2022-Nature Reviews Disease PrimersMarco Antonio KoffNo ratings yet
- Treatment of Xanthelasma Palpebrarum by Fractional Carbon Dioxide LaserDocument1 pageTreatment of Xanthelasma Palpebrarum by Fractional Carbon Dioxide LaserАркадий ЖивицаNo ratings yet
- Phlebotomy Issues and Quality Improvement (Review)Document15 pagesPhlebotomy Issues and Quality Improvement (Review)Yuendri IrawantoNo ratings yet
- Public Speaking Project Part 2Document3 pagesPublic Speaking Project Part 2api-388841477No ratings yet
- AbortionDocument92 pagesAbortionniraj_sdNo ratings yet
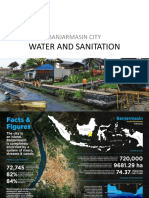
- Water and Sanitation: Banjarmasin CityDocument13 pagesWater and Sanitation: Banjarmasin CityAmelia MajidNo ratings yet
- Role of The Psychiatric Nurse in Initial Assessment & Specialling in Ward 4KDocument2 pagesRole of The Psychiatric Nurse in Initial Assessment & Specialling in Ward 4KYwagar YwagarNo ratings yet
- Cholecystitis CholelithiasisDocument8 pagesCholecystitis CholelithiasisNdhe PoetryNo ratings yet
- Behavior AdhdDocument8 pagesBehavior Adhdapi-533709691No ratings yet
- Resident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)Document104 pagesResident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)scalixto100% (1)
- MCQs Pharmacology - Series III-ADocument13 pagesMCQs Pharmacology - Series III-Asidharta_chatterjee100% (1)
- 1-Overview of Bipolar DisorderDocument10 pages1-Overview of Bipolar DisorderTcobb1969No ratings yet
- Lactation InsufficiencyDocument10 pagesLactation InsufficiencyThomas Regina PutraNo ratings yet
- Pharmaceutical Care: Qais AlefanDocument18 pagesPharmaceutical Care: Qais AlefanSaddamix AL OmariNo ratings yet
- Benefits of CounsellingDocument2 pagesBenefits of CounsellingJc OnyekwereNo ratings yet
- Ankle Disarticulation Prosthetics: Course Work ManualDocument52 pagesAnkle Disarticulation Prosthetics: Course Work ManualJananthan Thavarajah67% (3)
- Nueva Ecija University of Science and TechnologyDocument7 pagesNueva Ecija University of Science and TechnologyKym RonquilloNo ratings yet
- Blood ProductDocument89 pagesBlood ProductSam0% (1)
- Are We Ready For CannabisDocument15 pagesAre We Ready For CannabisBeatta RamirezNo ratings yet
- MENU Free Packet BW1Document10 pagesMENU Free Packet BW1Ana MariaNo ratings yet
- Ortho FractureDocument2 pagesOrtho FractureFritzTarronasNo ratings yet
- What Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyDocument1 pageWhat Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyE. LópezNo ratings yet