Download as pdf or txt
You might also like
- MEDICAL QUESTIONNAIRE SPJ CONNECT LLC (1) JorgeDocument8 pagesMEDICAL QUESTIONNAIRE SPJ CONNECT LLC (1) JorgeBALANCE DINAMICONo ratings yet
- OS 213 B07 Auscultation and Demonstration of Heart Sounds PDFDocument4 pagesOS 213 B07 Auscultation and Demonstration of Heart Sounds PDFMigs Medina100% (1)
- Horario LavanderiaDocument3 pagesHorario Lavanderiauniformes.lcbNo ratings yet
- The Effectiveness of Using Biochar Derivatives On The Establishment of Oil Palm Plantations in The Osa Peninsula in Costa Rica, Central AmericaDocument28 pagesThe Effectiveness of Using Biochar Derivatives On The Establishment of Oil Palm Plantations in The Osa Peninsula in Costa Rica, Central AmericaFrancisco GarroNo ratings yet
- RS T9 ClassificationDocument61 pagesRS T9 ClassificationShahwaiz MunirNo ratings yet
- Iterative Improvement of A Solution To Linear EquationsDocument41 pagesIterative Improvement of A Solution To Linear EquationsShirshendu RoyNo ratings yet
- Two Gents DoublingDocument1 pageTwo Gents DoublingDominicNo ratings yet
- Code For BP and ACDocument2 pagesCode For BP and ACAnti VitaNo ratings yet
- ADM&CTRL Critical Work ScheduleDocument1 pageADM&CTRL Critical Work Scheduleธนพงศ์ ซีวิล ไลน์ ธนพงศ์ ซีวิล ไลน์No ratings yet
- BABOKTechniquesMap v.01Document38 pagesBABOKTechniquesMap v.01Mohamed Awad0% (1)
- TPR-R Entrv. OnlineDocument12 pagesTPR-R Entrv. OnlineMacka Romy GPNo ratings yet
- TPR-R Entrv. OnlineDocument12 pagesTPR-R Entrv. OnlineMacka Romy GPNo ratings yet
- The Entry of Nanoparticles Into Solid Tumours: ArticlesDocument17 pagesThe Entry of Nanoparticles Into Solid Tumours: ArticlesMARTINA MARIA INSUA CASTRONo ratings yet
- List of Library DatabasesDocument470 pagesList of Library DatabasesAntonio AguiarNo ratings yet
- Science Set 1Document20 pagesScience Set 1Timo- SchutzNo ratings yet
- Consumibles PañolDocument4 pagesConsumibles PañollourdesbelenzariniNo ratings yet
- Random VariablesDocument57 pagesRandom VariablesJaff LawrenceNo ratings yet
- Factors/ GradesDocument4 pagesFactors/ GradesCristian Mihai StanilaNo ratings yet
- Contohpekerjaan PeriodikDocument9 pagesContohpekerjaan Periodikksatria99kyosihNo ratings yet
- StatsticsDocument20 pagesStatsticshussenNo ratings yet
- Maqsimaluri Qula - 4.: PasuxebiDocument3 pagesMaqsimaluri Qula - 4.: Pasuxebiucnobi ucnobiNo ratings yet
- I.2 Examples To Illustrate DOE Concepts 1. Optimally Feeding Fish 2. Targeting A Process/Reducing Process VariationDocument25 pagesI.2 Examples To Illustrate DOE Concepts 1. Optimally Feeding Fish 2. Targeting A Process/Reducing Process Variationhyoung65No ratings yet
- My MusicDocument8 pagesMy MusicNandor88No ratings yet
- Jadwal Shuttle September 2021Document7 pagesJadwal Shuttle September 2021Erwin PrasetyaNo ratings yet
- Address Calculator PDFDocument5 pagesAddress Calculator PDFvictorNo ratings yet
- Cuota Proislas Del Rosario Internos HucDocument4 pagesCuota Proislas Del Rosario Internos Hucapi-26938636No ratings yet
- Gov Corporate Governance VW Ar22Document50 pagesGov Corporate Governance VW Ar22Santiago EspinosaNo ratings yet
- Analisis Data DCMDocument12 pagesAnalisis Data DCMAyecx AmorphusNo ratings yet
- kết quả khảo saDocument5 pageskết quả khảo saDungNo ratings yet
- EnqestaDocument12 pagesEnqestamarialaura150507No ratings yet
- Tabulación de 16 EstudiantesDocument6 pagesTabulación de 16 Estudiantesalex idrugoNo ratings yet
- Date Deposit Withdraw LOT Pair Gross Profit Commision Nett Profit $30.00 Total BalanceDocument4 pagesDate Deposit Withdraw LOT Pair Gross Profit Commision Nett Profit $30.00 Total BalancezicareNo ratings yet
- SPCDocument49 pagesSPCJosephi_abbasNo ratings yet
- TSV' Complimentary Design Spooktacular Bookmark by Jo-Anne Mason For Dinky-Dyes DesignsDocument4 pagesTSV' Complimentary Design Spooktacular Bookmark by Jo-Anne Mason For Dinky-Dyes DesignsJennifer Koren FeichtNo ratings yet
- rf4 Fishing GuideDocument1 pagerf4 Fishing Guideeric gabNo ratings yet
- Random Variables 2Document56 pagesRandom Variables 2Jaff LawrenceNo ratings yet
- Capstone Week 4Document2 pagesCapstone Week 4Keshav SinghNo ratings yet
- SLIK KUMPULAN Nambuhan Cengklik - Mitra SUYATMIDocument958 pagesSLIK KUMPULAN Nambuhan Cengklik - Mitra SUYATMIagus purwantoNo ratings yet
- Feature Selection For Unsupervised Learning: Jennifer G. DyDocument45 pagesFeature Selection For Unsupervised Learning: Jennifer G. DyBruno Fabio Bedón VásquezNo ratings yet
- Perimeter Protection FunctionalitiesDocument1 pagePerimeter Protection FunctionalitiesRomiNo ratings yet
- Chapter 8: Correlaiton and Simple Linear Regression AnalysisDocument7 pagesChapter 8: Correlaiton and Simple Linear Regression AnalysisRUHDRANo ratings yet
- 09 - Partial Fraction Decomposition PDFDocument2 pages09 - Partial Fraction Decomposition PDFRenelyn AbacanNo ratings yet
- 09 - Partial Fraction Decomposition PDFDocument2 pages09 - Partial Fraction Decomposition PDFJan Leynard ParraNo ratings yet
- Partial Fraction DecompositionDocument2 pagesPartial Fraction DecompositionRowena ZabalaNo ratings yet
- SLIK KUMPULAN Nambuhan Cengklik - PJ Sri CahyaniDocument958 pagesSLIK KUMPULAN Nambuhan Cengklik - PJ Sri Cahyaniagus purwantoNo ratings yet
- Tabulasi Dan Olah Data Untuk WiyaDocument6 pagesTabulasi Dan Olah Data Untuk WiyaazmanRRNo ratings yet
- Decanter Cake SiteDocument1 pageDecanter Cake SiteSteve Stephianus LausNo ratings yet
- Lesson 04-The DerivativeDocument14 pagesLesson 04-The DerivativeAXELLE NICOLE GOMEZNo ratings yet
- Jin-Han2010 ReferenceWorkEntry K-MeansClusteringDocument10 pagesJin-Han2010 ReferenceWorkEntry K-MeansClusteringEduards Moises Triviño VildósolaNo ratings yet
- 2819 Ang Huling El Bimbo714902287554464242Document1 page2819 Ang Huling El Bimbo714902287554464242Escalation ACN WhirlpoolNo ratings yet
- Din en Iso 2338Document1 pageDin en Iso 2338Rafi UdeenNo ratings yet
- DIN EN ISO 2338 Dowel Pins: d-m6 d-h8 C Length LDocument1 pageDIN EN ISO 2338 Dowel Pins: d-m6 d-h8 C Length LPatrascu Robert-GabrielNo ratings yet
- J Joen 2016 06 007Document15 pagesJ Joen 2016 06 007Luis KabreraNo ratings yet
- PlanDocument11 pagesPlansgsfNo ratings yet
- Location: Toquepala Client: SPCC User Name: Famesa Explosivos Sac General: Asistencia TecnicaDocument1 pageLocation: Toquepala Client: SPCC User Name: Famesa Explosivos Sac General: Asistencia TecnicaJohnNo ratings yet
- FM-GAHRD-01 Training Matrix FinalDocument12 pagesFM-GAHRD-01 Training Matrix FinalimamNo ratings yet
- Questionnaire ResultsDocument3 pagesQuestionnaire Resultsemat mendozaNo ratings yet
- Differentiating Productsand Quotientsof Functions PR4 BDocument4 pagesDifferentiating Productsand Quotientsof Functions PR4 BAlperen ÇelebiNo ratings yet
- Indicate Location of Membrane-Shell Prototype at Bernburg Campus ?Document21 pagesIndicate Location of Membrane-Shell Prototype at Bernburg Campus ?pedrormunozNo ratings yet
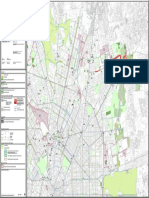
- 04PS S02 Servizi Verde Mobilita 2 N-EDocument1 page04PS S02 Servizi Verde Mobilita 2 N-EDiploma 2020No ratings yet
- Subcutaneous Emphysema From Crown PreparationDocument4 pagesSubcutaneous Emphysema From Crown PreparationAamir BidiwalaNo ratings yet
- Central Retinal Artery Occlusion - Rethinking TimeDocument6 pagesCentral Retinal Artery Occlusion - Rethinking TimeAamir BidiwalaNo ratings yet
- Oral Surgery Specialist List Application FormDocument13 pagesOral Surgery Specialist List Application FormAamir BidiwalaNo ratings yet
- Sensory Nerve Grafting of Lingual and Inferior Alveolar NervesDocument22 pagesSensory Nerve Grafting of Lingual and Inferior Alveolar NervesAamir BidiwalaNo ratings yet
- Alveolar OstitisDocument8 pagesAlveolar OstitisAamir BidiwalaNo ratings yet
- Alveolar OstitisDocument8 pagesAlveolar OstitisAamir BidiwalaNo ratings yet
- Nurse Practitioner Resume 1Document2 pagesNurse Practitioner Resume 1api-596656815No ratings yet
- Total Protein FS : Order InformationDocument2 pagesTotal Protein FS : Order InformationMikko DecolongonNo ratings yet
- Cva DocumentationDocument17 pagesCva DocumentationgannadortchNo ratings yet
- Case Study AFPMedCen Crypt Orchid IsmDocument14 pagesCase Study AFPMedCen Crypt Orchid Isme25g60No ratings yet
- HIV Manifestations in ENTDocument23 pagesHIV Manifestations in ENTRajesh darlingNo ratings yet
- Preeclampsia Early Recognition ToolDocument1 pagePreeclampsia Early Recognition ToolHaniv Prasetya AdhiNo ratings yet
- Project in Mapeh (Health)Document8 pagesProject in Mapeh (Health)guache warrinNo ratings yet
- SUMMATIVE TEST QUARTER 3 Week 3Document2 pagesSUMMATIVE TEST QUARTER 3 Week 3Mary CrisNo ratings yet
- BPHDocument57 pagesBPHDiannetotz MoralesNo ratings yet
- BMJ Fever in The Returning TravellerDocument9 pagesBMJ Fever in The Returning Travellertayfan1No ratings yet
- Clinical Laboratory Immunology 1st Edition Mahon Test BankDocument7 pagesClinical Laboratory Immunology 1st Edition Mahon Test Banksarahpalmerotpdkjcwfq100% (35)
- A Case Study On Mild Compression Deformity L1Document25 pagesA Case Study On Mild Compression Deformity L1JM UncianoNo ratings yet
- MTO Medical Condition ReportDocument2 pagesMTO Medical Condition ReportecNo ratings yet
- EPB - PPT EconomicDocument23 pagesEPB - PPT EconomicRafia ButtNo ratings yet
- Kings Phlebotomists HCP Information BookletDocument7 pagesKings Phlebotomists HCP Information Bookletapi-94821083No ratings yet
- Office of The Punong Barangay Barangay Certification of AcceptanceDocument1 pageOffice of The Punong Barangay Barangay Certification of AcceptanceMah Jane DivinaNo ratings yet
- Preeklampsia BeratDocument5 pagesPreeklampsia BeratmelatiigdNo ratings yet
- Skill: Assessing The Mouth and Oropharynx: Lips and Buccal MucosaDocument3 pagesSkill: Assessing The Mouth and Oropharynx: Lips and Buccal MucosaAlmira GamaoNo ratings yet
- Gammagard Us PiDocument4 pagesGammagard Us Pibmartindoyle6396No ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJessa BorreNo ratings yet
- 2nd Exam Vice and DrugsDocument15 pages2nd Exam Vice and DrugsCeilo TrondilloNo ratings yet
- Vitasum PDFDocument22 pagesVitasum PDFHen8No ratings yet
- Evidence of Learning 1Document4 pagesEvidence of Learning 1api-655779303No ratings yet
- 68w Chapter 01 - RevDocument7 pages68w Chapter 01 - Revsmith.kevin1420344No ratings yet
- Psychiatric Nursing Bullets Neurotransmission TheoryDocument4 pagesPsychiatric Nursing Bullets Neurotransmission TheoryDefensor Pison Gringgo100% (1)
- 05 N017 2931Document13 pages05 N017 2931anju negalurNo ratings yet
- AntibioticsDocument56 pagesAntibioticsCabdi IshakNo ratings yet
- Insulin AspartDocument2 pagesInsulin AspartPatricia MaglasangNo ratings yet
- Is Atopica Safe - Should I Give Atopica To My Dog - PDFDocument19 pagesIs Atopica Safe - Should I Give Atopica To My Dog - PDFJason GrohNo ratings yet