Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Banquet OrderDocument1 pageBanquet OrderApril NNo ratings yet
- Vip For Dec.10 11 12Document2 pagesVip For Dec.10 11 12April NNo ratings yet
- July 14-26Document2 pagesJuly 14-26April NNo ratings yet
- Edward and EleneeDocument14 pagesEdward and EleneeApril NNo ratings yet
- Sponsors NamesDocument2 pagesSponsors NamesApril NNo ratings yet
- VIPs FOR DECEMBER 16 17 19 22Document2 pagesVIPs FOR DECEMBER 16 17 19 22April NNo ratings yet
- Wedding Itinerary Ran YnahDocument11 pagesWedding Itinerary Ran YnahApril NNo ratings yet
- August 23-September 6Document9 pagesAugust 23-September 6April NNo ratings yet
- Seating ArrangementDocument2 pagesSeating ArrangementApril NNo ratings yet
- December 15 - December 24Document7 pagesDecember 15 - December 24April NNo ratings yet
- August 15-September 7Document7 pagesAugust 15-September 7April NNo ratings yet
- February 28 - March 9Document7 pagesFebruary 28 - March 9April NNo ratings yet
- May 19 - June 13Document13 pagesMay 19 - June 13April NNo ratings yet
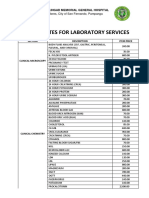
- JBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalDocument4 pagesJBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalApril NNo ratings yet
- July 11 - July 27Document12 pagesJuly 11 - July 27April NNo ratings yet
- T65 PoaDocument2 pagesT65 PoaApril NNo ratings yet
- T65 LogDocument4 pagesT65 LogApril NNo ratings yet
- GL CLS 503 Laboratory Packages 1Document5 pagesGL CLS 503 Laboratory Packages 1April NNo ratings yet
- Invoice # 13Document2 pagesInvoice # 13April NNo ratings yet
- Maid of Honor Best Man Principal Sponsors Bridesmaid GroomsmenDocument2 pagesMaid of Honor Best Man Principal Sponsors Bridesmaid GroomsmenApril NNo ratings yet
- Srts Bofop June 2022Document739 pagesSrts Bofop June 2022April NNo ratings yet
- Wedding Date: Time: Church: Reception: Address: Motif: AttireDocument11 pagesWedding Date: Time: Church: Reception: Address: Motif: AttireApril NNo ratings yet
- Wedding Itinerary Pineda ValenzuelaDocument13 pagesWedding Itinerary Pineda ValenzuelaApril NNo ratings yet
- SOA - Bank of FloridaDocument1 pageSOA - Bank of FloridaApril NNo ratings yet
- Aprilrosedavidnarciso : Hseofdavidinvestment&Mgmt Hdgbldgdolorescsf 2000pampangaDocument6 pagesAprilrosedavidnarciso : Hseofdavidinvestment&Mgmt Hdgbldgdolorescsf 2000pampangaApril NNo ratings yet
- PR Obat PT. DSSP Power Sumsel September 2022Document34 pagesPR Obat PT. DSSP Power Sumsel September 2022dr. Ukie HasibuanNo ratings yet
- A1 Wholesale PriceDocument2 pagesA1 Wholesale PriceNebiyat KitawNo ratings yet
- Backgrounder FDADocument89 pagesBackgrounder FDAWilliams PerdomoNo ratings yet
- Regulatory Requirements: Drs. Jan WelinkDocument37 pagesRegulatory Requirements: Drs. Jan WelinkdocreetisinghalNo ratings yet
- Pilots and Medication: What's The Problem? What To Look ForDocument2 pagesPilots and Medication: What's The Problem? What To Look ForPablo SánchezNo ratings yet
- Laporan Inhouse Clinic PT SIIX 2023Document135 pagesLaporan Inhouse Clinic PT SIIX 2023Tabita SilalahiNo ratings yet
- Pharmacology Reviewer DrugsDocument3 pagesPharmacology Reviewer DrugsChezka MendozaNo ratings yet
- Konfirmasi Persediaan RsudDocument6 pagesKonfirmasi Persediaan RsudCorneLia JacintaNo ratings yet
- The Truth About: Prescription Drug AbuseDocument32 pagesThe Truth About: Prescription Drug AbuseklockNo ratings yet
- Alzheimers DiseaseDocument85 pagesAlzheimers DiseaseThe ChannelNo ratings yet
- Antiepileptic Drug QuestionsDocument2 pagesAntiepileptic Drug QuestionsFerhan AbdiNo ratings yet
- AssignmentDocument9 pagesAssignmentNisu PrajapatiNo ratings yet
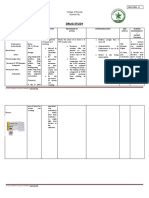
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaNo ratings yet
- Parkinsons Disease Prescribing Guidelines 2019 JMB Master 003 1615205551Document18 pagesParkinsons Disease Prescribing Guidelines 2019 JMB Master 003 1615205551143 lutfiana azzahraNo ratings yet
- Omeprazole - Drug StudyDocument2 pagesOmeprazole - Drug StudyBolasoc, HazelNo ratings yet
- Pharmacology Questions1Document30 pagesPharmacology Questions1Lucy Bamfiwaa AdusaNo ratings yet
- Lamp 2 Standar Matkes Kri SHSDocument10 pagesLamp 2 Standar Matkes Kri SHSmusmanNo ratings yet
- Stok 19 April 2021 AbbasyDocument125 pagesStok 19 April 2021 AbbasyRama RakanataNo ratings yet
- Prescription-Non Prescription Products: Hitanxi Vyas (19-35) Paridhi Trivedi (19-33) Pharm D 3 YearDocument19 pagesPrescription-Non Prescription Products: Hitanxi Vyas (19-35) Paridhi Trivedi (19-33) Pharm D 3 Year19-28 Manan PopatNo ratings yet
- Finasteride in Men With BPHDocument3 pagesFinasteride in Men With BPHmonia agni wiyatamiNo ratings yet
- Tugas Mors Kelompok 5 Analisis ABC Indeks KritisDocument11 pagesTugas Mors Kelompok 5 Analisis ABC Indeks Kritishastomo prabowoNo ratings yet
- E.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsDocument1 pageE.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsSafura IjazNo ratings yet
- Stock Harian ObatDocument5 pagesStock Harian ObatAprilia SilmiNo ratings yet
- Off Exclusivity DrugsDocument17 pagesOff Exclusivity DrugsJagdish ChanderNo ratings yet
- 1g+daftar HRGDocument26 pages1g+daftar HRGJava ShopNo ratings yet
- Data ObatDocument11 pagesData ObatAndreas AndreNo ratings yet
- giải osce nội đợt 1 2 3Document17 pagesgiải osce nội đợt 1 2 3Thành Tài TrầnNo ratings yet
- Daftar Obat Ranap - MiraRevisiDocument6 pagesDaftar Obat Ranap - MiraRevisiMiraNo ratings yet
- STOK8Document35 pagesSTOK8Adinda Nur AtifahNo ratings yet
- Harga ObatDocument71 pagesHarga Obatklinik madaniyahNo ratings yet