Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
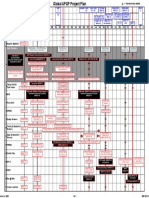
- GM 1927 01 Project PlanDocument1 pageGM 1927 01 Project Planmark100% (2)
- Expt 2Document7 pagesExpt 2toshgangwarNo ratings yet
- History: I. General DataDocument16 pagesHistory: I. General DataEnzo PamaNo ratings yet
- Pama - Joao Artemio Lorenzo PATHOLOGY LABORATORY CORRELATE ACTIVITY NO. 2Document5 pagesPama - Joao Artemio Lorenzo PATHOLOGY LABORATORY CORRELATE ACTIVITY NO. 2Enzo PamaNo ratings yet
- PPE Food PreparationDocument1 pagePPE Food PreparationEnzo PamaNo ratings yet
- Meeting Starts AgendaDocument2 pagesMeeting Starts AgendaEnzo PamaNo ratings yet
- Advt 2013 Ver 3Document6 pagesAdvt 2013 Ver 3mukesh_mlbNo ratings yet
- Resume - Soumya Prasad SenguptaDocument2 pagesResume - Soumya Prasad Senguptagcgary87No ratings yet
- File DisksDocument22 pagesFile DisksAlana PetersonNo ratings yet
- Am at Photogr 21 February 2015Document92 pagesAm at Photogr 21 February 2015TraficantdePufarineNo ratings yet
- Industrial Training ReportDocument6 pagesIndustrial Training Reportmayank guptaNo ratings yet
- Ch6-Mechanical PropertiesDocument39 pagesCh6-Mechanical PropertiesSaif AlbaddawiNo ratings yet
- Benefits of Being Bilingual Lesson PlanDocument4 pagesBenefits of Being Bilingual Lesson PlanCristina BoantaNo ratings yet
- Safety Rules and Laboratory Equipment: Experiment 1Document5 pagesSafety Rules and Laboratory Equipment: Experiment 1ricardojosecortinaNo ratings yet
- A Total Productive Maintenance (TPM) Approach To Improve Overall Equipment EfficiencyDocument4 pagesA Total Productive Maintenance (TPM) Approach To Improve Overall Equipment EfficiencyIJMERNo ratings yet
- Settima Screw Pumps - SMT SeriesDocument28 pagesSettima Screw Pumps - SMT SerieskikinNo ratings yet
- Rw15 ManualDocument314 pagesRw15 ManualpedrogerardohjNo ratings yet
- Tutorial Materials SelectionDocument2 pagesTutorial Materials SelectionSyahmiNo ratings yet
- Calculation of Potential Flow Around An Elliptic Cylinder Using Boundary Element MethodDocument15 pagesCalculation of Potential Flow Around An Elliptic Cylinder Using Boundary Element MethodDoğancan UzunNo ratings yet
- Hindalco ReportDocument42 pagesHindalco ReportAman RoyNo ratings yet
- DP FourSeals ENGDocument60 pagesDP FourSeals ENGgeorgia83609No ratings yet
- Author's Purpose Mini PassagesDocument5 pagesAuthor's Purpose Mini Passages18118No ratings yet
- Revision On Unit 1,2 First Secondry (Hello)Document11 pagesRevision On Unit 1,2 First Secondry (Hello)Vivian GendyNo ratings yet
- How To Implement SAP NoteDocument13 pagesHow To Implement SAP NoteSurya NandaNo ratings yet
- SuperWale Data SheetDocument8 pagesSuperWale Data SheetMagnum CompositesNo ratings yet
- Year 9 Naplan Non CalcDocument12 pagesYear 9 Naplan Non CalcSophieNoorSalibiNo ratings yet
- Terraformer D TsDocument7 pagesTerraformer D TsprogramhNo ratings yet
- Ingeteam Catalogo Cms Mayo2019 Eng MailDocument7 pagesIngeteam Catalogo Cms Mayo2019 Eng MailChrist Rodney MAKANANo ratings yet
- DGD2106M App NoteDocument9 pagesDGD2106M App NotecharlesNo ratings yet
- Conceptual Approaches To Human EcologyDocument24 pagesConceptual Approaches To Human EcologyBilly WenNo ratings yet
- 如何写一个简短的开场白Document6 pages如何写一个简短的开场白afmojdevnNo ratings yet
- 320DLRR GMX ELE SchematicDocument14 pages320DLRR GMX ELE Schematicthaw3tar3minNo ratings yet
- Nynas Transformer Oil - Nytro 10GBN: Naphthenics Product Data SheetDocument1 pageNynas Transformer Oil - Nytro 10GBN: Naphthenics Product Data SheetAnonymous S29FwnFNo ratings yet
- Dokumen - Tips - Incalzire Cu Pompe de CalduraDocument34 pagesDokumen - Tips - Incalzire Cu Pompe de CalduraPitique De TarencriqueNo ratings yet