Download as pdf or txt
You might also like
- MSDS For PN 3000671, Beacon Replacement Kit (Part 1) PDFDocument15 pagesMSDS For PN 3000671, Beacon Replacement Kit (Part 1) PDFAndrianoNo ratings yet
- Period MonologuesDocument9 pagesPeriod Monologueslaurelbeth100% (1)
- Wisdom From TD Jakes FREEDocument224 pagesWisdom From TD Jakes FREEayodeji78100% (3)
- J Jacbts 2021 10 011Document15 pagesJ Jacbts 2021 10 011Martha CeciliaNo ratings yet
- Thecardiovascular Manifestationsof Covid-19Document9 pagesThecardiovascular Manifestationsof Covid-19Alejandro ChecaNo ratings yet
- Tugas Jurnal Gadar Fatkul FaisDocument13 pagesTugas Jurnal Gadar Fatkul FaisUthy SurtyNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & Reviews: Cardiovascular Disease and COVID-19Document4 pagesDiabetes & Metabolic Syndrome: Clinical Research & Reviews: Cardiovascular Disease and COVID-19sanya eusebia lupaca lupacaNo ratings yet
- Lesion Miocardica en COVIDDocument10 pagesLesion Miocardica en COVIDSamuel ToroNo ratings yet
- ACS During Covid-19Document30 pagesACS During Covid-19Mella WarizkaNo ratings yet
- Acute Ischemic Stroke and COVID-19: Clinical and Population SciencesDocument8 pagesAcute Ischemic Stroke and COVID-19: Clinical and Population SciencesYunika KhairinaNo ratings yet
- The Association of Cardiovascular Diseases and Diabetes Mellitus With COVID-19 (SARS-CoV-2) and Their Possible MechanismsDocument6 pagesThe Association of Cardiovascular Diseases and Diabetes Mellitus With COVID-19 (SARS-CoV-2) and Their Possible MechanismsPatty MArivel ReinosoNo ratings yet
- 477-Article Text-1073-1-10-20200407Document6 pages477-Article Text-1073-1-10-20200407dani rahayuNo ratings yet
- Editorial Review Article: Cardiovascular Implications of Coronavirus Disease 2019: Review of Current LiteraturesDocument8 pagesEditorial Review Article: Cardiovascular Implications of Coronavirus Disease 2019: Review of Current LiteraturesDea DickytaNo ratings yet
- Arritmias Cardiacas en CovidDocument8 pagesArritmias Cardiacas en CovidLorena RiveraNo ratings yet
- Molecular Basis of Cardiac and Vascular Injuries Associated With COVID-19Document15 pagesMolecular Basis of Cardiac and Vascular Injuries Associated With COVID-19Aji Prasetyo UtomoNo ratings yet
- COVID y Lesion Miocardica 2020Document40 pagesCOVID y Lesion Miocardica 2020Carlos Alejandro Aguila BravoNo ratings yet
- Current Perspectives On Coronavirus Disease 2019 and Cardiovascular Disease: A White Paper by The JAHA EditorsDocument23 pagesCurrent Perspectives On Coronavirus Disease 2019 and Cardiovascular Disease: A White Paper by The JAHA EditorsCorina NedelcuNo ratings yet
- Myocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationDocument18 pagesMyocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationStephen DonovanNo ratings yet
- Literature Review of Cardiovascular Pathology in Coronavirus InfectionDocument5 pagesLiterature Review of Cardiovascular Pathology in Coronavirus InfectionCentral Asian StudiesNo ratings yet
- 2021 - RodillaDocument12 pages2021 - RodillaCarlNo ratings yet
- Miocarditis y Covid-19Document8 pagesMiocarditis y Covid-19Jesús Evangelista GomerNo ratings yet
- Journal of Cardiac Surgery - 2020 - Hakmi - Cardiac Tamponade in COVID 19 Patients Management and OutcomesDocument8 pagesJournal of Cardiac Surgery - 2020 - Hakmi - Cardiac Tamponade in COVID 19 Patients Management and Outcomesdrnaufal ilmiNo ratings yet
- Corona 2019 Revised PDFDocument9 pagesCorona 2019 Revised PDFGhassan SaffariniNo ratings yet
- Estado Del Arte CoronavirusDocument17 pagesEstado Del Arte CoronavirusJosé AñorgaNo ratings yet
- Jamacardiology Puntmann 2020 Oi 200057 1605207404.62135Document9 pagesJamacardiology Puntmann 2020 Oi 200057 1605207404.62135Faizal MusthofaNo ratings yet
- Unusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Document5 pagesUnusual Pattern of Arterial Macrothrombosis Causing Stroke in A Young Adult Recovered From COVID-19Audrey Beatrice ReyesNo ratings yet
- Dandel2021 Heart - Lung Interactions in COVID-19Document15 pagesDandel2021 Heart - Lung Interactions in COVID-19Mario TGNo ratings yet
- Jamacardiology Puntmann 2020 Oi 200057Document9 pagesJamacardiology Puntmann 2020 Oi 200057Henry DanielNo ratings yet
- Dr. A. Lucia Panda, SPPD, SPJP (K) - Cardiac Implication Due To COVID-19 Infection PDFDocument51 pagesDr. A. Lucia Panda, SPPD, SPJP (K) - Cardiac Implication Due To COVID-19 Infection PDFGeabyNo ratings yet
- Covid19 y CardioDocument4 pagesCovid19 y CardioNestor Alonso Lopez RubioNo ratings yet
- Clinical Microbiology and InfectionDocument12 pagesClinical Microbiology and Infectionre septian IlhamsyahNo ratings yet
- Cardiovascular Manifestations and Treatment in Covid 19Document10 pagesCardiovascular Manifestations and Treatment in Covid 19ollyvia mariance kembuanNo ratings yet
- Characteristics of Ischaemic Stroke Associated With COVID-19Document3 pagesCharacteristics of Ischaemic Stroke Associated With COVID-19Qisti AshariNo ratings yet
- Sindrome Cardiovascular Agudo COVID 2020Document12 pagesSindrome Cardiovascular Agudo COVID 2020Carlos Alejandro Aguila BravoNo ratings yet
- Adults 6Document7 pagesAdults 6Bshara SleemNo ratings yet
- COVID 19 Is A Systemic Vascular HemopathyDocument34 pagesCOVID 19 Is A Systemic Vascular HemopathyYuri YogyaNo ratings yet
- Vlachakis2020 Article ConcernsForManagementOfSTEMIPaDocument5 pagesVlachakis2020 Article ConcernsForManagementOfSTEMIPaDr. RajibNo ratings yet
- Considerations For Heart Failure Care During The COVID-19 PandemicDocument11 pagesConsiderations For Heart Failure Care During The COVID-19 PandemicBasilio BabarNo ratings yet
- Acute Cerebrovascular Disease Following COVID-19: A Single Center, Retrospective, Observational StudyDocument6 pagesAcute Cerebrovascular Disease Following COVID-19: A Single Center, Retrospective, Observational StudysomyahNo ratings yet
- The Coagulopathy, Endotheliopathy, and Vasculitis of COVID 19Document9 pagesThe Coagulopathy, Endotheliopathy, and Vasculitis of COVID 19arif 2006No ratings yet
- Myocarditis CovidDocument7 pagesMyocarditis CovidbagholderNo ratings yet
- Cardiac Arrhythmia Among Hospitalized COVID-19 Patients at Gunung Jati General Hospital, IndonesiaDocument13 pagesCardiac Arrhythmia Among Hospitalized COVID-19 Patients at Gunung Jati General Hospital, IndonesiasalinasheviaNo ratings yet
- Scutelnic-Heldner2020 Article VascularEventsVascularDiseaseADocument16 pagesScutelnic-Heldner2020 Article VascularEventsVascularDiseaseAdenisNo ratings yet
- MainDocument13 pagesMainKaren NascimentoNo ratings yet
- COVID 19 and Acute Coronary Syndrome Lessons ForDocument2 pagesCOVID 19 and Acute Coronary Syndrome Lessons ForYuning tyas Nursyah FitriNo ratings yet
- A Review of ST Elevation Myocardial Infarction inDocument8 pagesA Review of ST Elevation Myocardial Infarction inJaime Guillén OrdóñezNo ratings yet
- Reviews: Thrombocytopathy and Endotheliopathy: Crucial Contributors To COVID-19 ThromboinflammationDocument16 pagesReviews: Thrombocytopathy and Endotheliopathy: Crucial Contributors To COVID-19 ThromboinflammationVictor StarkNo ratings yet
- COVID - 19 and Thromboembolism 05.08.20Document68 pagesCOVID - 19 and Thromboembolism 05.08.20Dr. RajibNo ratings yet
- Cerebrovascular Disease in COVID-19: Adult BrainDocument3 pagesCerebrovascular Disease in COVID-19: Adult BrainUsman Agus PrasetyoNo ratings yet
- COVID 19 and Stroke Incidence and Etiological Description inDocument9 pagesCOVID 19 and Stroke Incidence and Etiological Description innascool2016No ratings yet
- Covid19 2Document2 pagesCovid19 2nico lempanNo ratings yet
- AF PredictorDocument9 pagesAF PredictorandreaNo ratings yet
- PDF - Vol 98-12-N02Document2 pagesPDF - Vol 98-12-N02Carla CarvalhoNo ratings yet
- A Brand-New Cardiorenal Syndrome in The COVID-19 SettingDocument6 pagesA Brand-New Cardiorenal Syndrome in The COVID-19 SettingfannyNo ratings yet
- FCVM 08 634291Document13 pagesFCVM 08 634291simona.visan19No ratings yet
- Optimal Management of Acute Coronary Syndromes in The Era of COVID-19Document8 pagesOptimal Management of Acute Coronary Syndromes in The Era of COVID-19Dr. RajibNo ratings yet
- Managemen ACS COVID-19Document29 pagesManagemen ACS COVID-19Lydia ElimNo ratings yet
- Bibliografi A: Carta Cientı Fica / Rev Esp Cardiol. 2020 73 (8) :665-687Document4 pagesBibliografi A: Carta Cientı Fica / Rev Esp Cardiol. 2020 73 (8) :665-687DANIA LUCERO SANCHEZ SOTONo ratings yet
- Adults 4Document7 pagesAdults 4Bshara SleemNo ratings yet
- 3 PBDocument2 pages3 PBSyifa PutriNo ratings yet
- Ijmm 47 3 4854 PDFDocument13 pagesIjmm 47 3 4854 PDFarif 2006No ratings yet
- (2021 - Atherosclerosis Reports) COVID and Cardiovascular Disease, What We Know in 2021Document12 pages(2021 - Atherosclerosis Reports) COVID and Cardiovascular Disease, What We Know in 2021Iván PérezNo ratings yet
- COVID-19: Effects in Comorbidities and Special PopulationsFrom EverandCOVID-19: Effects in Comorbidities and Special PopulationsNo ratings yet
- Cardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal DiseaseDocument12 pagesCardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal Diseasetenty isniNo ratings yet
- Administration of Alpha1 Antitrypsin in Haemodialysis KDC 1000102Document3 pagesAdministration of Alpha1 Antitrypsin in Haemodialysis KDC 1000102tenty isniNo ratings yet
- Avfistula or Tunnelled Catheter For Haemodialysis Jok 1000e102Document1 pageAvfistula or Tunnelled Catheter For Haemodialysis Jok 1000e102tenty isniNo ratings yet
- Atrial Fibrillation and Thromboembolism in Patients With Chronic Kidney DiseaseDocument13 pagesAtrial Fibrillation and Thromboembolism in Patients With Chronic Kidney Diseasetenty isniNo ratings yet
- A Haemodialysis Journey From The West To The EastDocument7 pagesA Haemodialysis Journey From The West To The Easttenty isniNo ratings yet
- Role of Imaging in Post Pnemumonia COVID-19Document22 pagesRole of Imaging in Post Pnemumonia COVID-19tenty isniNo ratings yet
- Jadwal Zaal Anak-1Document20 pagesJadwal Zaal Anak-1tenty isniNo ratings yet
- Diagnostik Dasar Radiologis COVID-19Document42 pagesDiagnostik Dasar Radiologis COVID-19tenty isniNo ratings yet
- EWS and Triage in COVID - 19 FIXDocument26 pagesEWS and Triage in COVID - 19 FIXtenty isniNo ratings yet
- Peran Kedokteran ForensikDocument63 pagesPeran Kedokteran Forensiktenty isniNo ratings yet
- Anti Inflammasi Pada Covid 19Document54 pagesAnti Inflammasi Pada Covid 19tenty isniNo ratings yet
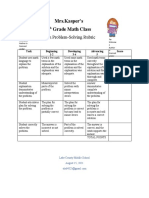
- Problemsolving RubricDocument1 pageProblemsolving Rubricapi-560491685No ratings yet
- Naamlp 2002 ProceedDocument578 pagesNaamlp 2002 ProceedRussell HartillNo ratings yet
- Panasonic TH-P42C10M, S, T, K, DDocument122 pagesPanasonic TH-P42C10M, S, T, K, DEliel PinheiroNo ratings yet
- Sample Questions FinalDocument11 pagesSample Questions FinaldunyaNo ratings yet
- Azosprilum 2Document24 pagesAzosprilum 2Dipti PriyaNo ratings yet
- PAYROLLMANAGEMENTDocument5 pagesPAYROLLMANAGEMENTSai Prabhav (Sai Prabhav)No ratings yet
- BlueStack Platform Marketing PlanDocument10 pagesBlueStack Platform Marketing PlanFıratcan KütükNo ratings yet
- LG 49uf680tDocument40 pagesLG 49uf680tnghanoiNo ratings yet
- VP3401 As04Document2 pagesVP3401 As04shivamtyagi68637No ratings yet
- ResearchDocument38 pagesResearchHelen McClintockNo ratings yet
- Gershwin George Rhapsody in Blue For Sax Quartet 64734Document113 pagesGershwin George Rhapsody in Blue For Sax Quartet 64734Jessica HowardNo ratings yet
- Unit 1 - Task 3 - Reader Guru Adventure! - Evaluation Quiz - Revisión Del IntentoDocument7 pagesUnit 1 - Task 3 - Reader Guru Adventure! - Evaluation Quiz - Revisión Del IntentoNelson AbrilNo ratings yet
- Sustainable Consumption Production in India - AnalysisDocument8 pagesSustainable Consumption Production in India - Analysisanon_794541559No ratings yet
- Effects of Organic Manure On Okra (AbelmoschusDocument4 pagesEffects of Organic Manure On Okra (AbelmoschusShailendra RajanNo ratings yet
- Drawing Using Cad SoftwareDocument21 pagesDrawing Using Cad SoftwareChris HeydenrychNo ratings yet
- 11a - Advanced - Turkish Grammar - NotesDocument79 pages11a - Advanced - Turkish Grammar - Notesfardousa ibNo ratings yet
- Summary 2Document2 pagesSummary 2Admin OfficeNo ratings yet
- Asmaa Mamdouh CVDocument1 pageAsmaa Mamdouh CVAsmaa MamdouhNo ratings yet
- Oma TS MLP V3 - 2 20110719 ADocument128 pagesOma TS MLP V3 - 2 20110719 AkennychanklNo ratings yet
- Comfort ZoneDocument4 pagesComfort Zonesigal ardanNo ratings yet
- Maunakea Brochure C SEED and L Acoustics CreationsDocument6 pagesMaunakea Brochure C SEED and L Acoustics Creationsmlaouhi MajedNo ratings yet
- Board of Technical Education (Student Marksheet)Document2 pagesBoard of Technical Education (Student Marksheet)Manoj SainiNo ratings yet
- Telegram DocumeDocument21 pagesTelegram Documemilli birhanuNo ratings yet
- HG-G9 Module 7 RTP PDFDocument10 pagesHG-G9 Module 7 RTP PDFDaniel Robert BuccatNo ratings yet
- Understanding Organizational Behavior: de Castro, Donna Amor Decretales, Thea Marie Estimo, Adrian Maca-Alin, SaharaDocument41 pagesUnderstanding Organizational Behavior: de Castro, Donna Amor Decretales, Thea Marie Estimo, Adrian Maca-Alin, SaharaAnna Marie RevisadoNo ratings yet
- Chapter 1 Peanut Growing and HarvestingDocument18 pagesChapter 1 Peanut Growing and HarvestingKapil BhattNo ratings yet
- Department of Mechanical Engineering: Final Year Mini Project PresentationDocument22 pagesDepartment of Mechanical Engineering: Final Year Mini Project PresentationNaresh DamaNo ratings yet