Download as docx, pdf, or txt
You might also like
- Gipsy Oracle Cards MeaningsDocument4 pagesGipsy Oracle Cards MeaningsFidel H. Viegas92% (12)
- Trigger Point Therapy Made Simple Serious Pain Relief in 4 Easy StepsDocument275 pagesTrigger Point Therapy Made Simple Serious Pain Relief in 4 Easy StepsMohaideen Subaire100% (11)
- Client Profile: Case StudyDocument1 pageClient Profile: Case Studysivakamasundari pichaipillaiNo ratings yet
- Reflection EssayDocument4 pagesReflection EssayaltonlinusNo ratings yet
- FNCP FinaaaalDocument5 pagesFNCP FinaaaalSoniaMarieBalanay0% (1)
- Sample 13 Areas of AssessmentDocument4 pagesSample 13 Areas of AssessmentLes Tarnate FechaNo ratings yet
- 13 AREAS of ASSESSMENT (Geriatrict Ward)Document2 pages13 AREAS of ASSESSMENT (Geriatrict Ward)Crystal Queen Marquez100% (1)
- 13 Areas of Assessment FrejDocument3 pages13 Areas of Assessment FrejJoMa TuazonNo ratings yet
- 13 Areas of AssessmentDocument4 pages13 Areas of AssessmentFretz John Z CamNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentShehada Marcos BondadNo ratings yet
- 13 Areas of AssessmentDocument4 pages13 Areas of AssessmentKryzza LeizellNo ratings yet
- Section: 2F-2A Clinical Instructor: Crisanto PulasDocument4 pagesSection: 2F-2A Clinical Instructor: Crisanto PulasKryzza LeizellNo ratings yet
- NCM 114 - NCPDocument3 pagesNCM 114 - NCPReysiela Mae ValinoNo ratings yet
- NCP For Rapid Shallow BreathingDocument1 pageNCP For Rapid Shallow Breathingbamboo2dNo ratings yet
- 13 Areas of AssessmentDocument2 pages13 Areas of AssessmentElija Leigh MauricioNo ratings yet
- NPI NCMH StephDocument12 pagesNPI NCMH StephAnonymous 2fUBWme6wNo ratings yet
- CHN - IdbDocument11 pagesCHN - IdbCharm RoweNo ratings yet
- Open I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityDocument21 pagesOpen I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityPOTENCIANA MAROMANo ratings yet
- Nursing Drug StudyDocument12 pagesNursing Drug StudyJoshkorro Geronimo100% (2)
- Nursing History and Gordon'sDocument2 pagesNursing History and Gordon'sCarlo bersamiraNo ratings yet
- Document (4) FNCP PrioritizationDocument7 pagesDocument (4) FNCP Prioritizationrose angelaNo ratings yet
- Pain Nursing Care Plan and Bactrobran Drug StudyDocument2 pagesPain Nursing Care Plan and Bactrobran Drug StudyAnni BarbaNo ratings yet
- Nursing Progress Notes FINALDocument2 pagesNursing Progress Notes FINALROXANNE V. LOPEZNo ratings yet
- NVS Written ReportDocument20 pagesNVS Written ReportbabiNo ratings yet
- Osteogenesis ImperfectaDocument52 pagesOsteogenesis ImperfectaTrias AdnyanaNo ratings yet
- 13 Areas of AssessmentDocument2 pages13 Areas of Assessmentmarkraymundangelica50% (2)
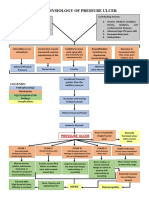
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- 13 Areas of Assessment 1 6 RevisedDocument10 pages13 Areas of Assessment 1 6 RevisedSherena NicolasNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument11 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaNo ratings yet
- CARE PLAN For BRONCHIECTASISDocument8 pagesCARE PLAN For BRONCHIECTASISCecil MonteroNo ratings yet
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Cu 3 Week 3Document3 pagesCu 3 Week 3Maica LectanaNo ratings yet
- Drug Study AtropineDocument3 pagesDrug Study AtropineAerron Severus Secano ShuldbergNo ratings yet
- Health Threat 1Document8 pagesHealth Threat 1Armand CabonitaNo ratings yet
- Agn NCPDocument6 pagesAgn NCPJewel AnneNo ratings yet
- NCP For Ulnar SurgeryDocument5 pagesNCP For Ulnar SurgeryjiloNo ratings yet
- Subjective: Objective: Short Term: Independent: Independent: Short TermDocument2 pagesSubjective: Objective: Short Term: Independent: Independent: Short TermJohn Patrick CuencoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intervention Rationale EvaluationFranz RolfNo ratings yet
- Physical AssessmentDocument4 pagesPhysical AssessmentAj Ann VillapazNo ratings yet
- 13 Areas of AssessmentDocument4 pages13 Areas of Assessmentnusdhockey0% (1)
- Sleep Pattern DisturbanceDocument1 pageSleep Pattern DisturbanceNik Rose ElNo ratings yet
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- Pathophysiology / Explanation of The ProblemDocument1 pagePathophysiology / Explanation of The ProblemArian May MarcosNo ratings yet
- Physical Assessment: Appeara Nce and Mental Status Actual Findings Normal Findings AnalysisDocument6 pagesPhysical Assessment: Appeara Nce and Mental Status Actual Findings Normal Findings AnalysisiammaiaNo ratings yet
- Burn - Daily Physical AssessmentDocument8 pagesBurn - Daily Physical AssessmentkrishcelNo ratings yet
- Learning Feedback g2Document8 pagesLearning Feedback g2Darwin DaveNo ratings yet
- NCP Hip FractureDocument5 pagesNCP Hip FractureCherry Ann BalagotNo ratings yet
- Hospital ParaphernaliaDocument2 pagesHospital ParaphernaliaMhOt AmAdNo ratings yet
- Drug Study PDFDocument7 pagesDrug Study PDFMarissa AsimNo ratings yet
- DOH Approved Medicinal PlantsDocument15 pagesDOH Approved Medicinal PlantsRENSON HERMOGINONo ratings yet
- PYOMYOSITISDocument6 pagesPYOMYOSITISChristine CoridoNo ratings yet
- NCP AnxietyDocument3 pagesNCP AnxietyclrssNo ratings yet
- Social Investigation Report FormDocument10 pagesSocial Investigation Report FormPpd Pmo ZamboangaNo ratings yet
- Bea Case StudyDocument19 pagesBea Case StudyBea Flor Rapisura-PegadNo ratings yet
- Healthcare - Drug Study Worksheet - Penicillin G SodiumDocument2 pagesHealthcare - Drug Study Worksheet - Penicillin G SodiumBenjamin CañalitaNo ratings yet
- 11 Form DR Write Up Rev July 2013.doc Revised 7 29 16Document1 page11 Form DR Write Up Rev July 2013.doc Revised 7 29 16Illya AnnesyNo ratings yet
- Community Health Nursing: Family Assessment Guide FormDocument8 pagesCommunity Health Nursing: Family Assessment Guide FormReese Gayle AvelinoNo ratings yet
- Impaired Physical MobilityDocument3 pagesImpaired Physical MobilityCharmaine ChuaNo ratings yet
- FractureDocument4 pagesFractureRaveen mayiNo ratings yet
- Potts DiseaseDocument8 pagesPotts Diseaseaimeeros0% (2)
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentCheska YsabelleNo ratings yet
- 1Document2 pages1jana whiteNo ratings yet
- Purposive CommunicationDocument19 pagesPurposive CommunicationYza Grace S. PayangdoNo ratings yet
- Narrative RepportDocument3 pagesNarrative RepportYza Grace S. PayangdoNo ratings yet
- Theoretical Foundation of NursingDocument7 pagesTheoretical Foundation of NursingYza Grace S. PayangdoNo ratings yet
- ReviewerDocument15 pagesReviewerYza Grace S. PayangdoNo ratings yet
- History Taking ActivityDocument6 pagesHistory Taking ActivityYza Grace S. PayangdoNo ratings yet
- Activity For The Reproductive SystemDocument1 pageActivity For The Reproductive SystemYza Grace S. PayangdoNo ratings yet
- English - X - Set - 2 - QPDocument10 pagesEnglish - X - Set - 2 - QPpassion and commitmentNo ratings yet
- Project Utthaan: A Leprosy Awareness InitiativeDocument6 pagesProject Utthaan: A Leprosy Awareness InitiativeAmaayaNo ratings yet
- Incredible 5-Second Water-Hack Kills Food CravingsDocument4 pagesIncredible 5-Second Water-Hack Kills Food CravingsSteeven MartínezNo ratings yet
- Emdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureDocument4 pagesEmdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureMohammed NabeelNo ratings yet
- LEC8 OncologyDocument19 pagesLEC8 Oncologymian gNo ratings yet
- Superficial Vein Thrombosis - 29aug2020Document5 pagesSuperficial Vein Thrombosis - 29aug2020Luis octavio carranzaNo ratings yet
- Fundus Fluorescein Angiography: Division of Clinical SciencesDocument5 pagesFundus Fluorescein Angiography: Division of Clinical SciencesPREM2KUMARNo ratings yet
- M. Khare - Air Pollution - Monitoring, MDLG., Health and Control-Intech (2012)Document264 pagesM. Khare - Air Pollution - Monitoring, MDLG., Health and Control-Intech (2012)B18EI007SINDHUVYSHNAVINo ratings yet
- The Effect of The Pandemic Caused by COVID19 To The Philippine EconomyDocument5 pagesThe Effect of The Pandemic Caused by COVID19 To The Philippine EconomyYna WenceslaoNo ratings yet
- Complete Micronutrient NestleDocument214 pagesComplete Micronutrient NestleChika SabaNo ratings yet
- Charles Brownlow - Texas Court of Criminal Appeals Opinion, Feb. 12, 2020Document54 pagesCharles Brownlow - Texas Court of Criminal Appeals Opinion, Feb. 12, 2020inForney.comNo ratings yet
- The Tokyo Subway Sarin Attack - Acute and Delayed HealthDocument9 pagesThe Tokyo Subway Sarin Attack - Acute and Delayed HealthDFNo ratings yet
- A Guide For Grandparents of Children With CancerDocument24 pagesA Guide For Grandparents of Children With CancerVanessa SilvaNo ratings yet
- Blood Research and DisordersDocument5 pagesBlood Research and Disordersdr_joe23No ratings yet
- Bootcamp's Step 1 Study ScheduleDocument8 pagesBootcamp's Step 1 Study ScheduleGlorivy E. Mora GonzalezNo ratings yet
- Basic Trauma Life SupportDocument40 pagesBasic Trauma Life Supportyunita murfhiNo ratings yet
- Parkinson Treatment Exercises-2Document20 pagesParkinson Treatment Exercises-2n&t3000No ratings yet
- Dr. Fahmi KhanDocument258 pagesDr. Fahmi KhanNasser Albaddai100% (2)
- Nami ResourceDocument1 pageNami Resourceapi-578365819No ratings yet
- Review of Literature On Diabetes Mellitus in IndiaDocument6 pagesReview of Literature On Diabetes Mellitus in Indiaafmztsqbdnusia100% (1)
- Antimicrobial Activity of Different Herbal Plants Extracts: A ReviewDocument38 pagesAntimicrobial Activity of Different Herbal Plants Extracts: A ReviewKima MadNo ratings yet
- Syndromic Management of Sexually Transmitable Infections Reference Manual (2) - 1Document116 pagesSyndromic Management of Sexually Transmitable Infections Reference Manual (2) - 1Keneni100% (1)
- BSN 3F 2B Ectopic Pregnancy PIH Case PresDocument47 pagesBSN 3F 2B Ectopic Pregnancy PIH Case PresKenji ToleroNo ratings yet
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Congenital Deformities: Gay G. Crisostomo-San Antonio, PTRP, MDDocument46 pagesCongenital Deformities: Gay G. Crisostomo-San Antonio, PTRP, MDJulia SalvioNo ratings yet
- Queen Siwes ReportDocument45 pagesQueen Siwes ReportAyodele OlorunfemiNo ratings yet
- Journey From Panic To Peace: Your Pathway To Taming Anxiety and Transforming It Into StrengthDocument212 pagesJourney From Panic To Peace: Your Pathway To Taming Anxiety and Transforming It Into StrengthMihai DubanNo ratings yet