Download as pdf or txt
You might also like
- Detroyer2018 Article EffectOfAnInteractiveE-learninDocument9 pagesDetroyer2018 Article EffectOfAnInteractiveE-learninramzan aliNo ratings yet
- Is Video-Based Education An Effective Method in Surgical Education? A Systematic ReviewDocument9 pagesIs Video-Based Education An Effective Method in Surgical Education? A Systematic Reviewmuhikhsan marikharNo ratings yet
- Flexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyDocument9 pagesFlexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyWalisson 5No ratings yet
- Jurnal 1Document9 pagesJurnal 1bella sariNo ratings yet
- Cheng 2020 - PsDocument8 pagesCheng 2020 - PsPriatharsine SeeranganNo ratings yet
- Chatterjee Video Lit Review Revised Oct20 Mmi EditsDocument39 pagesChatterjee Video Lit Review Revised Oct20 Mmi EditsVineeta PatelNo ratings yet
- Evidence-Based Practice Education For Healthcare PDocument6 pagesEvidence-Based Practice Education For Healthcare PAsmarany FauzanNo ratings yet
- Chapter 1 3 ResearchDocument26 pagesChapter 1 3 ResearchAb Staholic BoiiNo ratings yet
- Perceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Document9 pagesPerceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Walisson BarbosaNo ratings yet
- Uso de Tecnología para Mantener La Educación de Los Residentes Durante La Pandemia de COVID-19Document4 pagesUso de Tecnología para Mantener La Educación de Los Residentes Durante La Pandemia de COVID-19Yhonni Zela SancaNo ratings yet
- Jamapediatrics Mazurek 2020 Oi 190112Document9 pagesJamapediatrics Mazurek 2020 Oi 190112Héctor RedondoNo ratings yet
- Randomized Controlled Trial On The Effect of YouTube Surgical Videos On Procedural Knowledge and Perceived Self-EDocument17 pagesRandomized Controlled Trial On The Effect of YouTube Surgical Videos On Procedural Knowledge and Perceived Self-EVlarah Alondra LiponNo ratings yet
- A Resource For Teaching Emergency Care Communication: Clinical and Communication SkillsDocument6 pagesA Resource For Teaching Emergency Care Communication: Clinical and Communication SkillsAsihworo AnggraeniNo ratings yet
- Patient Safety Education For Undergraduate Medical Students: A Systematic ReviewDocument8 pagesPatient Safety Education For Undergraduate Medical Students: A Systematic ReviewNovaamelia jesicaNo ratings yet
- Blended Learning of Radiology Improves Medical Students 2ep7j3we0gDocument12 pagesBlended Learning of Radiology Improves Medical Students 2ep7j3we0gAKUMBOLE EZEKIELNo ratings yet
- Palliative CareDocument11 pagesPalliative CareCiocan AlexandraNo ratings yet
- Entrevistas TCCDocument37 pagesEntrevistas TCCBelen StrangeNo ratings yet
- 1 s2.0 S0738399121001701 MainDocument8 pages1 s2.0 S0738399121001701 MainYaumil FauziahNo ratings yet
- A Non-Randomised Trial of Video and Written Educational Adjuncts in Undergraduate OphthalmologyDocument8 pagesA Non-Randomised Trial of Video and Written Educational Adjuncts in Undergraduate OphthalmologyEwa JedrkowiakNo ratings yet
- Aot 9999 0Document12 pagesAot 9999 0NataliaNo ratings yet
- 1 s2.0 S2772628223000365 MainDocument9 pages1 s2.0 S2772628223000365 MainmarliivitorinoNo ratings yet
- MBE en El Currículo Médico Actual GuyattDocument3 pagesMBE en El Currículo Médico Actual GuyattmedicabrujaNo ratings yet
- VR Training in Health Care PDFDocument8 pagesVR Training in Health Care PDFthidayat15No ratings yet
- Children 10 00058Document13 pagesChildren 10 00058saludablemente conectadosNo ratings yet
- SimulationDocument9 pagesSimulationKaren Joyce Costales MagtanongNo ratings yet
- Introducción Al CursoDocument3 pagesIntroducción Al CursoFer45No ratings yet
- Benefits of A Bilingual Web-Based Anatomy Atlas For Nursing Students in Learning AnatomyDocument13 pagesBenefits of A Bilingual Web-Based Anatomy Atlas For Nursing Students in Learning AnatomyKenan GalijaševićNo ratings yet
- Medethex Online: A Computer-Based Learning Program in Medical Ethics and Communication SkillsDocument12 pagesMedethex Online: A Computer-Based Learning Program in Medical Ethics and Communication SkillsdrsrikanthreddyNo ratings yet
- Feedback 2 PDFDocument8 pagesFeedback 2 PDFMaría Francisca Rauch GajardoNo ratings yet
- Efficacy of Virtual Reality Simulation in Teaching Basic Life Support and Its Retention at 6 MonthsDocument9 pagesEfficacy of Virtual Reality Simulation in Teaching Basic Life Support and Its Retention at 6 Monthsputujunidtd13No ratings yet
- Overcoming Challenges Posed byDocument5 pagesOvercoming Challenges Posed byBley SolanoNo ratings yet
- Content ServerDocument11 pagesContent ServerMona AL-FaifiNo ratings yet
- Evaluation of The Feasibility of A Video-Transmitted Surgical Ward Round: A Proof of Concept StudyDocument7 pagesEvaluation of The Feasibility of A Video-Transmitted Surgical Ward Round: A Proof of Concept StudyRonald TrinidadNo ratings yet
- Applying Interprofessional Team-Based Learning in Patient Safety: A Pilot Evaluation StudyDocument9 pagesApplying Interprofessional Team-Based Learning in Patient Safety: A Pilot Evaluation StudyRhey RYNNo ratings yet
- UntitledDocument12 pagesUntitledDella ANo ratings yet
- TA - Kishore at Al. 2022Document10 pagesTA - Kishore at Al. 2022noratheseceditecNo ratings yet
- Jurnal 1Document11 pagesJurnal 1izal yusufNo ratings yet
- Introduction and Objectives: Ophthalmoscopy Is A CoreDocument6 pagesIntroduction and Objectives: Ophthalmoscopy Is A CoreWalisson BarbosaNo ratings yet
- Medu 14194Document2 pagesMedu 14194ZoeNo ratings yet
- Developing A Viva Exam To Assess ClinicalDocument9 pagesDeveloping A Viva Exam To Assess ClinicalROGERNo ratings yet
- John Et Al. Translating Patient Education Theory Into Practice.Document5 pagesJohn Et Al. Translating Patient Education Theory Into Practice.Rodrigo Miguel Rojas AndradeNo ratings yet
- Virtual Patient Simulations in Health Professions Education: Systematic Review and Meta-Analysis by The Digital Health Education CollaborationDocument20 pagesVirtual Patient Simulations in Health Professions Education: Systematic Review and Meta-Analysis by The Digital Health Education CollaborationManh Tien NgoNo ratings yet
- The Blacksmith Approach A Strategy For Teaching AnDocument14 pagesThe Blacksmith Approach A Strategy For Teaching AnSamuel BrunNo ratings yet
- The Effectiveness of Blended Learning in Basic Life Support Training Among Nursing Students: A Systematic ReviewDocument13 pagesThe Effectiveness of Blended Learning in Basic Life Support Training Among Nursing Students: A Systematic ReviewElaine Frances IlloNo ratings yet
- Wong2022 Article CriticalCareUltrasoundDocument3 pagesWong2022 Article CriticalCareUltrasoundA. RaufNo ratings yet
- Asthenopia Among University Students: The Eye of The Digital GenerationDocument12 pagesAsthenopia Among University Students: The Eye of The Digital GenerationNydia OngaliaNo ratings yet
- Nursing Informatics and Nursing EducationDocument3 pagesNursing Informatics and Nursing Educationtrisha100% (1)
- Innovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelDocument3 pagesInnovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelGeysel SuarezNo ratings yet
- 2018 Article 1442 1593517482874Document18 pages2018 Article 1442 1593517482874Icha KristinaNo ratings yet
- Advan 00097 2018Document5 pagesAdvan 00097 2018Walid HassanNo ratings yet
- Levett-Jones Et Al-2018-Journal of Nursing Scholarship1Document10 pagesLevett-Jones Et Al-2018-Journal of Nursing Scholarship1Nande BandeNo ratings yet
- Thistlethwaite 2015 Anatomical Sciences EducationDocument6 pagesThistlethwaite 2015 Anatomical Sciences EducationIkhwanYudaKusumaNo ratings yet
- Healthcare Education With Virtual-World SimulationDocument11 pagesHealthcare Education With Virtual-World SimulationDaniel MelloNo ratings yet
- Research Manuscript Oral DefenseDocument41 pagesResearch Manuscript Oral DefenseAntoinette PeleñaNo ratings yet
- Bioetica en Servicio de PediatriaDocument12 pagesBioetica en Servicio de PediatriaMayra del CarmenNo ratings yet
- Chicoine2021 Article EffectivenessAndExperiencesOfTDocument16 pagesChicoine2021 Article EffectivenessAndExperiencesOfTAldito GlasgowNo ratings yet
- Julian 2018Document9 pagesJulian 2018drdabielmaderacNo ratings yet
- The Impact of Clinical Visits On CommuniDocument7 pagesThe Impact of Clinical Visits On CommuniRS JNo ratings yet
- Yoo, 2010 EnglishDocument9 pagesYoo, 2010 EnglishaminNo ratings yet
- Comprehensive Healthcare Simulation: ECMO Simulation: A Theoretical and Practical GuideFrom EverandComprehensive Healthcare Simulation: ECMO Simulation: A Theoretical and Practical GuideLindsay C. JohnstonNo ratings yet
- Sr. No. Specific Objectives Time Subject Matter Teaching Learning Activities A.V. AidsDocument12 pagesSr. No. Specific Objectives Time Subject Matter Teaching Learning Activities A.V. AidsSanjay SinghNo ratings yet
- Lesson Plan Personality Disorders A Class of Their Own - 0Document9 pagesLesson Plan Personality Disorders A Class of Their Own - 0Sanjay SinghNo ratings yet
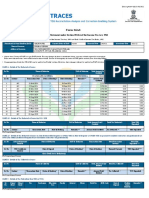
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Sanjay SinghNo ratings yet
- Lesson 4 Formal V70eazDocument7 pagesLesson 4 Formal V70eazSanjay SinghNo ratings yet
- Indian Income Tax Return Acknowledgement 2022-23: Assessment YearDocument1 pageIndian Income Tax Return Acknowledgement 2022-23: Assessment YearSanjay SinghNo ratings yet
- E Admit CardDocument5 pagesE Admit CardSanjay SinghNo ratings yet
- Metabolism Clinical and ExperimentalDocument4 pagesMetabolism Clinical and ExperimentalusingwebNo ratings yet
- Advance Copy 2022 NEGRIHP Final ManuscriptDocument440 pagesAdvance Copy 2022 NEGRIHP Final ManuscriptSchool NursingNo ratings yet
- Saranagathi Enewsletter September 2021Document13 pagesSaranagathi Enewsletter September 2021ramanagopalNo ratings yet
- Research Method: Sampling DesignDocument3 pagesResearch Method: Sampling DesignNoelle CaballeraNo ratings yet
- Perfect Booty Program Guide PDFDocument55 pagesPerfect Booty Program Guide PDFYenny Parra GaticaNo ratings yet
- Head To Head: Should All Advertising of Cosmetic Surgery Be Banned? YesDocument2 pagesHead To Head: Should All Advertising of Cosmetic Surgery Be Banned? YesLIM YIN SHENG / UPMNo ratings yet
- 211 1395 1 PBDocument6 pages211 1395 1 PBHreeneke EmerentiaNo ratings yet
- M1 Lesson 2Document4 pagesM1 Lesson 2Mary Grace Ferolino CañedaNo ratings yet
- Basic First Aid TrainingDocument109 pagesBasic First Aid TrainingFarrukh AhmedNo ratings yet
- Cinematic Environs - Desert WastesDocument28 pagesCinematic Environs - Desert WastesPhilmore Pockets100% (1)
- Blood Flukes: Richelle D. Sales, RMTDocument20 pagesBlood Flukes: Richelle D. Sales, RMTZairah PascuaNo ratings yet
- Full Download PDF of Test Bank For Psychiatric Mental Health Nursing 9th by Townsend All ChapterDocument41 pagesFull Download PDF of Test Bank For Psychiatric Mental Health Nursing 9th by Townsend All Chaptersetderofis100% (2)
- Principles and Practices of Behavioral AssessmentDocument8 pagesPrinciples and Practices of Behavioral AssessmentDavid Miranda RicoNo ratings yet
- Safety Data Sheet: (SDS) No. Bm-Msds 011ADocument5 pagesSafety Data Sheet: (SDS) No. Bm-Msds 011AChou JoeNo ratings yet
- CKD PDFDocument15 pagesCKD PDFJendrale SudirmanNo ratings yet
- Basic Medical Instrumentation System:-: Amitshanu - inDocument5 pagesBasic Medical Instrumentation System:-: Amitshanu - inÃmît ShâñúNo ratings yet
- Step by Step Guide To Critiquing Research Part 2Document7 pagesStep by Step Guide To Critiquing Research Part 2michael ndlovuNo ratings yet
- MJPJAY Procedures 996Document58 pagesMJPJAY Procedures 996bhushan adhariNo ratings yet
- Sort Set in Shine StandardizeDocument3 pagesSort Set in Shine StandardizeJan Bryan EslavaNo ratings yet
- Roll of Successful Examinees in The OCCUPATIONAL THERAPISTS LICENSURE EXAMINATIONDocument3 pagesRoll of Successful Examinees in The OCCUPATIONAL THERAPISTS LICENSURE EXAMINATIONRapplerNo ratings yet
- Radiation Safety SOP: Scope/PurposeDocument4 pagesRadiation Safety SOP: Scope/Purposezen AlkaffNo ratings yet
- Phctlab - Topic 1 - PrelimsDocument5 pagesPhctlab - Topic 1 - PrelimsasdfdjfeonaNo ratings yet
- Biomechanics of Open Bite TreatmentDocument40 pagesBiomechanics of Open Bite TreatmentMaitreye PriyadarshiniNo ratings yet
- Wenaas CatalogueDocument29 pagesWenaas CatalogueAnonymous 1dCz409sNo ratings yet
- Comparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediaDocument6 pagesComparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediafatinfatharaniNo ratings yet
- Transcultural Nursing - Sas 6Document3 pagesTranscultural Nursing - Sas 6Allyza Jane SartigaNo ratings yet
- MyBenefits - Program Brochure (FY21-22)Document27 pagesMyBenefits - Program Brochure (FY21-22)Manan ChaniyaraNo ratings yet
- SEOT JSA For Energizing Site DBDocument3 pagesSEOT JSA For Energizing Site DBArchana SoorajNo ratings yet
- RRT PT AssessmentDocument39 pagesRRT PT AssessmentRam NasaluddinNo ratings yet
- Week 8 TheoristsDocument8 pagesWeek 8 TheoristsHeleana Iris SulitNo ratings yet