Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- GIS Training DesignDocument2 pagesGIS Training DesignMarven JuadiongNo ratings yet
- Appendix A.2 Water TWorks Capacity ChecksDocument12 pagesAppendix A.2 Water TWorks Capacity Checksttl153153No ratings yet
- Amadeus TechRef Insurance Pricing 13.1 002Document68 pagesAmadeus TechRef Insurance Pricing 13.1 002Andrei GoguNo ratings yet
- Cut and FillDocument16 pagesCut and FillPongets SorianoNo ratings yet
- Ground Control Points (GCPS) : Automatic GCP DetectionDocument1 pageGround Control Points (GCPS) : Automatic GCP DetectionMarven JuadiongNo ratings yet
- Accident Reporting Procedure 1Document2 pagesAccident Reporting Procedure 1Marven JuadiongNo ratings yet
- Agri ProgrammeDocument2 pagesAgri ProgrammeMarven JuadiongNo ratings yet
- FARM 7 201 FilesDocument24 pagesFARM 7 201 FilesMarven JuadiongNo ratings yet
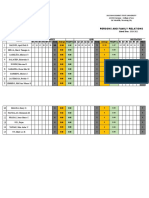
- Input Data Sheet For E-Class Record: Region Division School NameDocument39 pagesInput Data Sheet For E-Class Record: Region Division School NameMarven JuadiongNo ratings yet
- Persons and Family Relations: Sultan Kudarat State UniversityDocument4 pagesPersons and Family Relations: Sultan Kudarat State UniversityMarven JuadiongNo ratings yet
- Creating A Digital Engagement Action Plan: Module No. 3: Designing Positive Digital Engagement Social Media CampaignsDocument6 pagesCreating A Digital Engagement Action Plan: Module No. 3: Designing Positive Digital Engagement Social Media CampaignsMarven JuadiongNo ratings yet
- Municipal Assessor'S Office External ServicesDocument10 pagesMunicipal Assessor'S Office External ServicesMarven JuadiongNo ratings yet
- Entrepreneurship Final Exam Name: - Course & Section: - Date: - ScoreDocument2 pagesEntrepreneurship Final Exam Name: - Course & Section: - Date: - ScoreMarven JuadiongNo ratings yet
- YyyyyyyyyyDocument36 pagesYyyyyyyyyyMarven JuadiongNo ratings yet
- Awareness Towards Implementation of Solid Waste Management in The Coastal AreaDocument22 pagesAwareness Towards Implementation of Solid Waste Management in The Coastal AreaCelmer100% (1)
- Concept, Examples, Characteristics Types of Stress and StrainDocument21 pagesConcept, Examples, Characteristics Types of Stress and StrainAlicia Pereira NetoNo ratings yet
- PV 6702 EnglischDocument13 pagesPV 6702 Englischjopster84No ratings yet
- FAS Systems SystemLevel Diagnostics Guide PDFDocument30 pagesFAS Systems SystemLevel Diagnostics Guide PDFtelhemnosNo ratings yet
- Wavemakers For Physical Models: EquipmentDocument10 pagesWavemakers For Physical Models: Equipmentesmaeil013No ratings yet
- S P S Confined Space Entry: 1. ScopeDocument1 pageS P S Confined Space Entry: 1. Scopeananthu.uNo ratings yet
- Sidomuncul20190313064235169 1 PDFDocument298 pagesSidomuncul20190313064235169 1 PDFDian AnnisaNo ratings yet
- Dispute Management PDFDocument2 pagesDispute Management PDFPritam PatnaikNo ratings yet
- Bioetika Didalam Ilmu Kedokteran Blok 1 UMSUDocument25 pagesBioetika Didalam Ilmu Kedokteran Blok 1 UMSUMuhammad Hafiz MuflihNo ratings yet
- 199307Document87 pages199307vtvuckovicNo ratings yet
- Mangrove 1Document9 pagesMangrove 1Abdul HarisNo ratings yet
- Atmabodh: Paper On A Social NGO Making A Difference in Education For The UnderprivilegedDocument11 pagesAtmabodh: Paper On A Social NGO Making A Difference in Education For The UnderprivilegedSahil100% (2)
- 07 PPC Ch7 Theory of ConstraintsDocument52 pages07 PPC Ch7 Theory of ConstraintsziadatzNo ratings yet
- Laravel 5 Post PDFDocument292 pagesLaravel 5 Post PDFCarlos AnchundiaNo ratings yet
- Heritage Amruth-Senior HealthDocument31 pagesHeritage Amruth-Senior HealthSubhasreeNo ratings yet
- Introduction: Dada, Surrealism, and ColonialismDocument8 pagesIntroduction: Dada, Surrealism, and ColonialismDorota MichalskaNo ratings yet
- NorthStar L3 U3 Reading Writing - Student BookDocument24 pagesNorthStar L3 U3 Reading Writing - Student BookYuraima BustamanteNo ratings yet
- Multi-Criteria Decision MakingDocument22 pagesMulti-Criteria Decision MakingSeema DeviNo ratings yet
- ĐỀ 509Document3 pagesĐỀ 509Dũng HoàngNo ratings yet
- Mayur TidkeDocument2 pagesMayur TidkeNikhil DongareNo ratings yet
- Katana Viewer A Pi Getting Started GuideDocument30 pagesKatana Viewer A Pi Getting Started GuiderendermanuserNo ratings yet
- Chapter 23 Microbial EcosystemsDocument21 pagesChapter 23 Microbial EcosystemsElantikaeNo ratings yet
- 2e Starter Language Focus ReferenceDocument14 pages2e Starter Language Focus ReferenceCami AdornoNo ratings yet
- Finding A Girlfriend: Guide For Finding Your Love .Document26 pagesFinding A Girlfriend: Guide For Finding Your Love .ankit_wadhawanNo ratings yet
- 8automated Assembly SystemsDocument28 pages8automated Assembly SystemsvijayNo ratings yet
- IBM WebSphere Transformation Extender Pack For SWIFTNet FIN DownloadServletDocument4 pagesIBM WebSphere Transformation Extender Pack For SWIFTNet FIN DownloadServletalexpio2kNo ratings yet