Download as docx, pdf, or txt
You might also like
- Iep Performance TemplateDocument26 pagesIep Performance Templateapi-546335180100% (3)
- Megan Sanders Iep Performance TemplateDocument25 pagesMegan Sanders Iep Performance Templateapi-551429736100% (2)
- Iep Form 09 StaticDocument15 pagesIep Form 09 StaticAllehsiad Zenitram100% (1)
- SPD 490B IEP Performance TemplateDocument23 pagesSPD 490B IEP Performance TemplateTami GoddardNo ratings yet
- RSDB Update 20190620Document1 pageRSDB Update 20190620Oana Durst100% (1)
- Market Research Survey Sample QuestionnaireDocument4 pagesMarket Research Survey Sample QuestionnaireKhenan James Narisma100% (1)
- Mekton Zeta Errata 1-1Document3 pagesMekton Zeta Errata 1-1syNo ratings yet
- IEP Performance Template Steps 2-7Document29 pagesIEP Performance Template Steps 2-7Jacqueline Medina100% (2)
- Laker UDD 301v4 TrainingDocument182 pagesLaker UDD 301v4 Trainingkk kkNo ratings yet
- Individualized Education Program (Iep) : Page 1 of 21 April 2014Document21 pagesIndividualized Education Program (Iep) : Page 1 of 21 April 2014api-454875755No ratings yet
- Cassarolaura IepDocument21 pagesCassarolaura Iepapi-549821510No ratings yet
- Dahlia Prose IfspDocument9 pagesDahlia Prose Ifspapi-282677206No ratings yet
- Iep Example Fall11Document13 pagesIep Example Fall11api-242533667No ratings yet
- ProblemSet Sampling With SolutionsDocument12 pagesProblemSet Sampling With SolutionsAkhil GargNo ratings yet
- IEP Sample FormatDocument16 pagesIEP Sample FormatAsh DeibNo ratings yet
- Standard 2-4Document7 pagesStandard 2-4Amie McCormickNo ratings yet
- IEP Performance TemplateDocument29 pagesIEP Performance Templatesusie100% (1)
- Iep EvieDocument21 pagesIep Evieapi-504429100No ratings yet
- Iep Performance TemplateDocument25 pagesIep Performance Templateapi-687812867No ratings yet
- Individualized Education Program (Iep) School Age: Student's Name: ElliotDocument24 pagesIndividualized Education Program (Iep) School Age: Student's Name: Elliotapi-424939253No ratings yet
- Edu 347 Iep Anna This OneDocument30 pagesEdu 347 Iep Anna This Oneapi-537525579No ratings yet
- Iep RevisionDocument27 pagesIep Revisionapi-730523401No ratings yet
- 2F5.Application For ScholarshipDocument2 pages2F5.Application For ScholarshipnymphetamineleiNo ratings yet
- Iep Performance Template DoneDocument20 pagesIep Performance Template Doneapi-631448823No ratings yet
- Iep FinalDocument31 pagesIep Finalapi-443892331No ratings yet
- Boyle Final IepDocument25 pagesBoyle Final Iepapi-536990981No ratings yet
- Herrmann IepDocument20 pagesHerrmann Iepapi-302642159No ratings yet
- Iep Project ModDocument22 pagesIep Project Modapi-340955572No ratings yet
- Iep AssignmentDocument23 pagesIep Assignmentapi-561196792No ratings yet
- Jay Jones IepDocument20 pagesJay Jones Iepapi-709040597No ratings yet
- Hannah IepDocument28 pagesHannah Iepapi-521335305No ratings yet
- Edu 347 Bogosian IepDocument23 pagesEdu 347 Bogosian Iepapi-345962925No ratings yet
- Edu 347 John IepDocument23 pagesEdu 347 John Iepapi-467842024No ratings yet
- Spe 269 IepDocument15 pagesSpe 269 IepAmanda EvansNo ratings yet
- Stateiepform 1Document12 pagesStateiepform 1api-321851345No ratings yet
- Iep Performance Template RhiaDocument28 pagesIep Performance Template Rhiaapi-700597971No ratings yet
- IBDP Application FormDocument4 pagesIBDP Application FormYunzcho GhaleNo ratings yet
- ARD Form EPISD 2009 Revised Version 4Document46 pagesARD Form EPISD 2009 Revised Version 4setrayloNo ratings yet
- Adam Erickson IepDocument16 pagesAdam Erickson Iepapi-316863938No ratings yet
- Individualized Education Program (Iep) : Page 1 of 26 April 2014Document26 pagesIndividualized Education Program (Iep) : Page 1 of 26 April 2014api-535946620No ratings yet
- IEPDocument27 pagesIEPlawamandaNo ratings yet
- Individualized Education Program (Iep) : As Documented byDocument24 pagesIndividualized Education Program (Iep) : As Documented byapi-473349564No ratings yet
- Individualized Education Program (Iep)Document20 pagesIndividualized Education Program (Iep)api-302050301No ratings yet
- Iep BlankDocument20 pagesIep Blankapi-743634481No ratings yet
- Wc-Sed Iep FinalDocument22 pagesWc-Sed Iep Finalapi-246210596No ratings yet
- CCID Application 2011-2012Document5 pagesCCID Application 2011-2012saqibafridiNo ratings yet
- Taylor IepDocument27 pagesTaylor Iepapi-452780864No ratings yet
- IEPDocument14 pagesIEPAndrea BarrosoNo ratings yet
- Individualized Education Program (IEP) : Student Name: Michael Smith IEP Date: 3/6/2019 ID: 123456789Document6 pagesIndividualized Education Program (IEP) : Student Name: Michael Smith IEP Date: 3/6/2019 ID: 123456789Natalie ShaldaNo ratings yet
- RW IepDocument26 pagesRW Iepapi-326628660No ratings yet
- Individualized Education Program: School District Name: School District Address: School District Contact Person/Phone #Document8 pagesIndividualized Education Program: School District Name: School District Address: School District Contact Person/Phone #jiosjaNo ratings yet
- Tyler-Transition IepDocument14 pagesTyler-Transition Iepapi-346302593No ratings yet
- Indus International School, Pune Individual Educational Plan (IEP)Document6 pagesIndus International School, Pune Individual Educational Plan (IEP)satyasaiNo ratings yet
- Iep Jonas McdulleyDocument21 pagesIep Jonas Mcdulleyapi-301858064No ratings yet
- Iep Master Form New 1Document7 pagesIep Master Form New 1api-569225521No ratings yet
- LawiepDocument21 pagesLawiepapi-300247066No ratings yet
- Final Tisa Pypself-StudyDocument59 pagesFinal Tisa Pypself-StudyChem DP1No ratings yet
- Iep Meeting 2Document23 pagesIep Meeting 2api-438877205No ratings yet
- PR02 - AdvCertificate in SP TeachingDocument5 pagesPR02 - AdvCertificate in SP TeachingTheoNo ratings yet
- Agosto IepDocument37 pagesAgosto Iepapi-299648141No ratings yet
- Saludes - IEP Format 1Document7 pagesSaludes - IEP Format 1Angela ApolonioNo ratings yet
- IEP Example UpdatedDocument25 pagesIEP Example UpdatedAbbie StorerNo ratings yet
- Transition Planning Document 1Document2 pagesTransition Planning Document 1api-395972621No ratings yet
- The School System Comparison between the United States of America and FinlandFrom EverandThe School System Comparison between the United States of America and FinlandNo ratings yet
- RG - 150 - 400 Varybond Regular Grade Aerosol MSDS (E)Document8 pagesRG - 150 - 400 Varybond Regular Grade Aerosol MSDS (E)LandiheNo ratings yet
- Validation LetterDocument2 pagesValidation LetterChrisper EscotoNo ratings yet
- Houses and Apartments in AustraliaDocument12 pagesHouses and Apartments in Australiazozo torzoNo ratings yet
- DVD Lens ActuatorDocument6 pagesDVD Lens Actuatorp_j_r_mNo ratings yet
- Adverts and Pop Culture - The Clever Tricks of Advertising - WorksheetDocument2 pagesAdverts and Pop Culture - The Clever Tricks of Advertising - WorksheetAmer AlshafieNo ratings yet
- 2022-06-02 Calvert County TimesDocument24 pages2022-06-02 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- BOM100033596 ChasisDocument227 pagesBOM100033596 ChasisFelipe Andrés Camarada SilvaNo ratings yet
- Chaper Three Coordinate Transformation MTUDocument12 pagesChaper Three Coordinate Transformation MTUbirukdese677No ratings yet
- Monday PresentationDocument26 pagesMonday PresentationAlexandraNo ratings yet
- Din 6885Document1 pageDin 6885Riadini Anis Hade50% (2)
- Ratan TataDocument2 pagesRatan TataSandeepBoseNo ratings yet
- Sandhya Vandhanam Procedure - AnanthDocument24 pagesSandhya Vandhanam Procedure - AnanthChaitra AnanthNo ratings yet
- Chufamix Recipe Book EngDocument100 pagesChufamix Recipe Book EnglollibravoNo ratings yet
- Measures of VariabilityDocument7 pagesMeasures of VariabilityAngelica FloraNo ratings yet
- Math 6 - Q4 - Mod1 - DeterminingTheRelationshipOfVolumeBetweenARectangularPrismAndAPyramidACylinderAndAConeACylinderAndSphere - V3Document21 pagesMath 6 - Q4 - Mod1 - DeterminingTheRelationshipOfVolumeBetweenARectangularPrismAndAPyramidACylinderAndAConeACylinderAndSphere - V3Kathlyn PerezNo ratings yet
- Mentum Cell PlannerDocument2 pagesMentum Cell PlannerledhieNo ratings yet
- Balmer Lawrie & Co HRDocument6 pagesBalmer Lawrie & Co HRPraneet TNo ratings yet
- Compliance CalendarDocument12 pagesCompliance CalendarAshish MallickNo ratings yet
- Intalacion de PiezometrosDocument14 pagesIntalacion de Piezometrosjoeldlrosa0No ratings yet
- Digital Image and Video Processing Nov 2022Document5 pagesDigital Image and Video Processing Nov 2022khushiduppalaNo ratings yet
- Final Ma MaDocument30 pagesFinal Ma MaKUMARAGURU PONRAJNo ratings yet
- 1701722483.roksim Alone in Space and No Suits at AllDocument28 pages1701722483.roksim Alone in Space and No Suits at AlllolyeetwutNo ratings yet
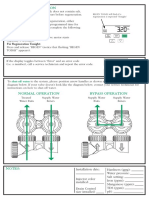
- Manual Regeneration: Shut-Off Water Bypass OperationDocument2 pagesManual Regeneration: Shut-Off Water Bypass OperationcaroNo ratings yet
- LS 5 Understanding The Self and Society 3Document70 pagesLS 5 Understanding The Self and Society 3Rotary Club Of Cubao SunriseNo ratings yet
- Teacher Answer Key What Is My Adaptation WorksheetsDocument2 pagesTeacher Answer Key What Is My Adaptation Worksheetssteffielisa12No ratings yet