Download as docx, pdf, or txt
You might also like
- Biochemical Markers of Bone Metabolism PPT LectureDocument89 pagesBiochemical Markers of Bone Metabolism PPT LectureNeil Vincent De AsisNo ratings yet
- Nursing Care Plan (Bowel Elemination)Document8 pagesNursing Care Plan (Bowel Elemination)Rijane Tabonoc Omlang100% (1)
- Vestibular RehabilitationDocument55 pagesVestibular RehabilitationHaniym ZawawiNo ratings yet
- Introd Anti ConvulsantsDocument56 pagesIntrod Anti ConvulsantstheintrovNo ratings yet
- Antiepileptic DrugsDocument65 pagesAntiepileptic DrugsZarish IftikharNo ratings yet
- Anti Epileptic Drugs - The Old and The New 2011Document10 pagesAnti Epileptic Drugs - The Old and The New 20115stringcelloNo ratings yet
- Pharmacology of AntiepilepticDocument36 pagesPharmacology of AntiepilepticManWol JangNo ratings yet
- Antiepileptic Drugs (Anti-Seizure Drugs) - IDocument39 pagesAntiepileptic Drugs (Anti-Seizure Drugs) - Inouramansour235No ratings yet
- Anesthesia Books 2019 Bonica's-5001-6053Document1,053 pagesAnesthesia Books 2019 Bonica's-5001-6053rosangelaNo ratings yet
- Antiepileptics (Autosaved)Document57 pagesAntiepileptics (Autosaved)vishal singhNo ratings yet
- Anti-Convulsants/Antiepileptic Drugs: Prepared By: DR Sana FaheemDocument23 pagesAnti-Convulsants/Antiepileptic Drugs: Prepared By: DR Sana Faheemaziz aliNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Managing Patients Who Have Seizure Disorders Dental and Medical IssuesDocument8 pagesManaging Patients Who Have Seizure Disorders Dental and Medical Issuesvika_asriningrum2563No ratings yet
- Drug InteractionsDocument21 pagesDrug InteractionsPawan Deshmukh100% (1)
- Status EpilepticusDocument42 pagesStatus EpilepticusJesse EstradaNo ratings yet
- Delayed Recovery After AnaesthesiaDocument5 pagesDelayed Recovery After Anaesthesiakoolstarone100% (1)
- Epilepsy: Neurovascular DisordersDocument30 pagesEpilepsy: Neurovascular DisordersNdoo NdooNo ratings yet
- Anti-Epileptic Drugs - A Guide For The Non-NeurologistDocument5 pagesAnti-Epileptic Drugs - A Guide For The Non-NeurologistArgentin2No ratings yet
- AntiepilepticsDocument13 pagesAntiepilepticstbuyinza21apNo ratings yet
- Drug Addiction & The BrainDocument45 pagesDrug Addiction & The BrainGaurav JainNo ratings yet
- Fentanyl - StatPearls - NCBI BookshelfDocument5 pagesFentanyl - StatPearls - NCBI BookshelfIsabel MoraNo ratings yet
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
- Rebound Phenomenon - Important and Ubiquitous inDocument5 pagesRebound Phenomenon - Important and Ubiquitous inCITRA AYU APRILIANo ratings yet
- HaloperidolDocument4 pagesHaloperidolNickol BaylonNo ratings yet
- 7) 13 AntiepilepticsDocument27 pages7) 13 AntiepilepticsKhushboo IkramNo ratings yet
- Anticonvulsants Power PointDocument146 pagesAnticonvulsants Power Pointrossfancy736No ratings yet
- Jurding Neuro ShindyDocument21 pagesJurding Neuro ShindyarifNo ratings yet
- Anticonvulsants WebDocument23 pagesAnticonvulsants WebVictor YaremkoNo ratings yet
- Case Vignette. EpilepsyDocument8 pagesCase Vignette. EpilepsyAizel ManiagoNo ratings yet
- 18.jaladi Himaja Battu Rakesh PDFDocument9 pages18.jaladi Himaja Battu Rakesh PDFFebby da costaNo ratings yet
- Psychiatry AmbossDocument11 pagesPsychiatry Ambosstomisin99gordonNo ratings yet
- Pharmacology Psychiatric MedicationsDocument36 pagesPharmacology Psychiatric Medicationsamasoud96 amasoud96No ratings yet
- Atypical Antipsychotics in Bipolar Disorder: The Treatment of ManiaDocument9 pagesAtypical Antipsychotics in Bipolar Disorder: The Treatment of ManiaAnonymous L3q7yHhhNo ratings yet
- Adjuvant Analgesics For Pain Management FINAL PARTDocument13 pagesAdjuvant Analgesics For Pain Management FINAL PARTbalamuruganNo ratings yet
- CHAPTER 19: Drugs Used For Seizure DisordersDocument19 pagesCHAPTER 19: Drugs Used For Seizure DisordersAziil LiizaNo ratings yet
- Antiepileptic DrugsDocument24 pagesAntiepileptic Drugsjanemwanza003No ratings yet
- Evaluation of The Clinical Efficacy of Phenytoin in The Treatment of Epileptic Seizures in ChildrenDocument4 pagesEvaluation of The Clinical Efficacy of Phenytoin in The Treatment of Epileptic Seizures in ChildrenAcademic JournalNo ratings yet
- CASE STUDY Chapter 59 (ANTIEMETIC AGENTS)Document4 pagesCASE STUDY Chapter 59 (ANTIEMETIC AGENTS)Kate Angelique RodriguezNo ratings yet
- Anti Epileptic DrugsDocument6 pagesAnti Epileptic DrugsFaria Islam JuhiNo ratings yet
- Therapeutic Effects of Phytochemicals and MedicinaDocument11 pagesTherapeutic Effects of Phytochemicals and MedicinaMd. JubairNo ratings yet
- Anti Epileptic AgentsDocument64 pagesAnti Epileptic AgentsPrincess VanquirayNo ratings yet
- Epilepsy Anesthesia ConsiderationDocument7 pagesEpilepsy Anesthesia ConsiderationEugenius FlavantoNo ratings yet
- 2013 Pharmacology of Balance and DizzinessDocument14 pages2013 Pharmacology of Balance and Dizzinessfono.jcbertolaNo ratings yet
- Fphar 12 604040Document28 pagesFphar 12 604040biblioteka1.mzlNo ratings yet
- Pain Therapy: by Dr. Hesham GhareebDocument52 pagesPain Therapy: by Dr. Hesham GhareebHesham hfghareebNo ratings yet
- Newer Updates in Psychiatry: Focus On Vortioxetine: 10.5005/jp-Journals-10067-0024Document4 pagesNewer Updates in Psychiatry: Focus On Vortioxetine: 10.5005/jp-Journals-10067-0024Imon PaulNo ratings yet
- Eti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaDocument43 pagesEti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaadystiNo ratings yet
- Antiepileptic FullDocument60 pagesAntiepileptic FullBurning DesireNo ratings yet
- Psychoactive DrugsDocument24 pagesPsychoactive DrugsIshaani GargNo ratings yet
- Systemic Effects of Histamine and SerotoninDocument5 pagesSystemic Effects of Histamine and SerotoninibrahimNo ratings yet
- TDM of PhenytoinDocument5 pagesTDM of PhenytoinMounika16 PedamalluNo ratings yet
- Part I. Benzodiazepines-Side Effects, Abuse Risk and AlternativesDocument13 pagesPart I. Benzodiazepines-Side Effects, Abuse Risk and AlternativesPamella Kusuma WerdanieNo ratings yet
- First Generation AntipsychoticDocument4 pagesFirst Generation AntipsychoticPutu Agus Grantika100% (1)
- Anti-Epileptics: Awale YusufDocument42 pagesAnti-Epileptics: Awale Yusufahmed mahamedNo ratings yet
- Anti Epileptic DrugsDocument15 pagesAnti Epileptic DrugsTod KembleNo ratings yet
- EMRAP 2017 12 December Track17 ProceduralSedation SummaryDocument4 pagesEMRAP 2017 12 December Track17 ProceduralSedation Summaryjairo Navia GonzalezNo ratings yet
- Anti Maniac DrugsDocument32 pagesAnti Maniac DrugsMohamad SamirNo ratings yet
- Two Toxicologic Emergencies: Case Studies inDocument4 pagesTwo Toxicologic Emergencies: Case Studies insiddharsclubNo ratings yet
- Pharmacology 2Document37 pagesPharmacology 2jekeri bekeriNo ratings yet
- PharmTest3 StudyGuideDocument9 pagesPharmTest3 StudyGuideTara Bickford ManisNo ratings yet
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionNo ratings yet
- Fast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonFrom EverandFast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonNo ratings yet
- John's Case StudyDocument8 pagesJohn's Case StudySky KaurNo ratings yet
- ASSESSMENT 3 (Peer-Review) : Section A (Highlight or Bold Your Response)Document3 pagesASSESSMENT 3 (Peer-Review) : Section A (Highlight or Bold Your Response)Sky KaurNo ratings yet
- Task One AssissgnmentDocument22 pagesTask One AssissgnmentSky KaurNo ratings yet
- BSBLDR502 Tajinder AssignmentDocument61 pagesBSBLDR502 Tajinder AssignmentSky KaurNo ratings yet
- SOP Neonatal SepsisDocument3 pagesSOP Neonatal SepsisEidi IdhamNo ratings yet
- 3.3 Integrated Management of Childhood Illness PDFDocument11 pages3.3 Integrated Management of Childhood Illness PDFVernonDimalNo ratings yet
- Well-Built Clinical QuestionDocument29 pagesWell-Built Clinical QuestionsdghyNo ratings yet
- Gigfolfiri ProtocolDocument6 pagesGigfolfiri ProtocolNurfarah BilqisNo ratings yet
- Anesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaDocument3 pagesAnesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaJhevilin RMNo ratings yet
- Malaria in Pregnancy 1Document12 pagesMalaria in Pregnancy 1api-3705046No ratings yet
- 5 PyatakDocument21 pages5 PyatakJust HelpingNo ratings yet
- HHFB Endowment Tri-FoldDocument2 pagesHHFB Endowment Tri-FoldStephanie Martin HarmonNo ratings yet
- b9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDocument63 pagesb9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDaud ParluhutanNo ratings yet
- AmiodaroneDocument2 pagesAmiodaroneEmmil BernardoNo ratings yet
- Anti Protozoal AgentsDocument37 pagesAnti Protozoal AgentsGunjan YadavNo ratings yet
- Surgery Eng Sirius 200 MCQ KDocument51 pagesSurgery Eng Sirius 200 MCQ KALok Kumar100% (1)
- CBC Hilot (Wellness Massage) NC IIDocument3 pagesCBC Hilot (Wellness Massage) NC IIWynnZhruhMatulina100% (2)
- Temblor de HolmesDocument7 pagesTemblor de HolmesIan Luis Flores SaavedraNo ratings yet
- Grabovoi Healing NumbersDocument34 pagesGrabovoi Healing NumbersTwonNo ratings yet
- Renal UltrasoundDocument179 pagesRenal UltrasoundJuhar AhamedNo ratings yet
- Think Right Now! - I Am Healed NowDocument3 pagesThink Right Now! - I Am Healed NowvaltroduoNo ratings yet
- Ultra Low Dose CT Vs Chest X Ray in Non Traumatic Emergency D 2023 EClinicaDocument14 pagesUltra Low Dose CT Vs Chest X Ray in Non Traumatic Emergency D 2023 EClinicaronaldquezada038No ratings yet
- Lung Cancer Molecular BiologyDocument58 pagesLung Cancer Molecular BiologyRobert NicolaeNo ratings yet
- 14-06-2021 HMB EnglishDocument40 pages14-06-2021 HMB EnglishKiran SNNo ratings yet
- Elarde, Sylvia Somodio 2440010207Document3 pagesElarde, Sylvia Somodio 2440010207Jenn ElardeNo ratings yet
- Ciaa 889Document24 pagesCiaa 889jocely matheus de moraes netoNo ratings yet
- Effects of Dry Needling On Calf Muscle in Case of Myofascial Trigger Point With Mild Restriction of Knee Joint Movement: A Case StudyDocument4 pagesEffects of Dry Needling On Calf Muscle in Case of Myofascial Trigger Point With Mild Restriction of Knee Joint Movement: A Case StudyIJAR JOURNALNo ratings yet
- EeeeeeDocument8 pagesEeeeeeLSG ApprenticeNo ratings yet
- Retromolar Embryonal Rhabdomyosarcoma: A CaseDocument6 pagesRetromolar Embryonal Rhabdomyosarcoma: A CaseNabila RizkikaNo ratings yet
- Severe Mini-Mental State Examination PDFDocument1 pageSevere Mini-Mental State Examination PDFKelly YoungNo ratings yet
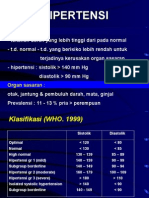
- HipertensiDocument28 pagesHipertensidokteraanNo ratings yet