Download as pdf or txt
You might also like
- End Emotional Eating by Jennifer TaitzDocument229 pagesEnd Emotional Eating by Jennifer TaitzIrena100% (2)
- Pediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDocument6 pagesPediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDiego Vargas LópezNo ratings yet
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (7)
- An Investigation of The Voice Handicap Index WithSpeakers of Portuguese Preliminary DataDocument13 pagesAn Investigation of The Voice Handicap Index WithSpeakers of Portuguese Preliminary DataAlexandraNo ratings yet
- 2016, Behlau Et Al Voice Self-Assessment Protocols Different Trends OD BD in P...Document15 pages2016, Behlau Et Al Voice Self-Assessment Protocols Different Trends OD BD in P...Carol PaesNo ratings yet
- Validation VHI 1997Document6 pagesValidation VHI 1997Sebastian Castro TigheNo ratings yet
- ESV. Moreti Et Al Validation (BR) Version of The VoiSS 2014Document11 pagesESV. Moreti Et Al Validation (BR) Version of The VoiSS 2014Luis SeixasNo ratings yet
- Feeling Normal? Long-Term Follow-Up of Patients With A Cleft Lip - Palate After Rhinoplasty With The Derriford Appearance Scale (DAS-59)Document6 pagesFeeling Normal? Long-Term Follow-Up of Patients With A Cleft Lip - Palate After Rhinoplasty With The Derriford Appearance Scale (DAS-59)Claudia TacuriNo ratings yet
- Conocimientos Cuidados en La VozDocument12 pagesConocimientos Cuidados en La VozJo QuezadaNo ratings yet
- Voice Therapy OutcomeDocument10 pagesVoice Therapy Outcomemajid mirzaeeNo ratings yet
- 2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseDocument9 pages2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseCarol PaesNo ratings yet
- Iief 1997 PDFDocument9 pagesIief 1997 PDFVlad GramaNo ratings yet
- Angadi 2017Document22 pagesAngadi 2017Javiera Paz Rios CarmonaNo ratings yet
- (Factors Predicting Voice Handicap Index) : Acta Otorrinolaringológica Española March 2006Document10 pages(Factors Predicting Voice Handicap Index) : Acta Otorrinolaringológica Española March 2006Truong Ngoc HuyNo ratings yet
- Functional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueseDocument6 pagesFunctional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueserudolfpeterssonNo ratings yet
- Voice-And Swallow-Related Quality of Life in Idiopathic Parkinson's DiseaseDocument7 pagesVoice-And Swallow-Related Quality of Life in Idiopathic Parkinson's DiseaseDiego VásquezNo ratings yet
- 10 1016@j Jvoice 2018 07 007Document6 pages10 1016@j Jvoice 2018 07 007ismail39 orthoNo ratings yet
- Organization of The Referral and Counter-Referral System in A Speech-Language Pathology and Audiology Clinic-SchoolDocument6 pagesOrganization of The Referral and Counter-Referral System in A Speech-Language Pathology and Audiology Clinic-SchoolCarolina UrrutiaNo ratings yet
- Autoavaliacao e Prontidao para Mudanca em PacienteDocument7 pagesAutoavaliacao e Prontidao para Mudanca em PacienteSonia Mercedes Yusty OsorioNo ratings yet
- Svhi 10Document7 pagesSvhi 10Lancelot du Lac100% (1)
- Somatoform Disorders in General Practice: Prevalence, Functional Impairment and Comorbidity With Anxiety and Depressive DisordersDocument17 pagesSomatoform Disorders in General Practice: Prevalence, Functional Impairment and Comorbidity With Anxiety and Depressive Disordersmei-257402No ratings yet
- Are The Acoustic Measurements Reliable in The Assessment ofDocument13 pagesAre The Acoustic Measurements Reliable in The Assessment ofIsabel Monteiro GomesNo ratings yet
- Development and Validation of The Quality of Life.39 PDFDocument5 pagesDevelopment and Validation of The Quality of Life.39 PDFTeiza NabilahNo ratings yet
- The "Lechol Nefesh" Project: Intensive and Long Term Psychoanalytic Psychotherapy in Public Mental Health CentersDocument15 pagesThe "Lechol Nefesh" Project: Intensive and Long Term Psychoanalytic Psychotherapy in Public Mental Health CentersPierreNo ratings yet
- Ppa 8 727Document28 pagesPpa 8 727Devhy MazrianiNo ratings yet
- Artículo Misofonía TratamientoDocument26 pagesArtículo Misofonía TratamientomanoliNo ratings yet
- Acoustic and Facial Features From ClinicalDocument16 pagesAcoustic and Facial Features From ClinicalDa CuNo ratings yet
- Literature Review of Facial PalsyDocument4 pagesLiterature Review of Facial Palsyfvet7q93100% (1)
- Lorangeretal IntlPDExam 1994 PDFDocument11 pagesLorangeretal IntlPDExam 1994 PDFlakshmi shankarNo ratings yet
- Lorangeretal IntlPDExam 1994 PDFDocument11 pagesLorangeretal IntlPDExam 1994 PDFlakshmi shankarNo ratings yet
- JurnalDocument18 pagesJurnalHerfanus DuhaNo ratings yet
- Jurnal - 2Document15 pagesJurnal - 2ristytegarNo ratings yet
- Guideline Adherence in Speech and Language Therapy in Stroke Aftercare. A Health Insurance Claims Data AnalysisDocument19 pagesGuideline Adherence in Speech and Language Therapy in Stroke Aftercare. A Health Insurance Claims Data AnalysisErika GalvisNo ratings yet
- RODRIGUES ET AL 2021 - Traumatic Spinal Injury - JoVDocument10 pagesRODRIGUES ET AL 2021 - Traumatic Spinal Injury - JoVLuis SeixasNo ratings yet
- Gasparini Et Al - Validação QVV - 2009Document6 pagesGasparini Et Al - Validação QVV - 2009Luis SeixasNo ratings yet
- Zane Llo 2014Document10 pagesZane Llo 2014djokopri07No ratings yet
- The International Personality Disorder Examination.: Archives of General Psychiatry January 1994Document11 pagesThe International Personality Disorder Examination.: Archives of General Psychiatry January 1994Irisha AnandNo ratings yet
- Dysphagia Handicap Index, Development and ValidationDocument7 pagesDysphagia Handicap Index, Development and ValidationWlf OoNo ratings yet
- 15 Castelli, Heeb, Gulfi, Gutjahr (2015)Document9 pages15 Castelli, Heeb, Gulfi, Gutjahr (2015)Pablo Ferrer GonzalezNo ratings yet
- A Voice Rehabilitation Protocol With The SOVMDocument8 pagesA Voice Rehabilitation Protocol With The SOVMRachelNo ratings yet
- Validation of PRISM (Pictorial Representation of Illness and Self Measure) As A Novel Visual Assessment Tool For The Burden of Suffering in Tinnitus PatientsDocument9 pagesValidation of PRISM (Pictorial Representation of Illness and Self Measure) As A Novel Visual Assessment Tool For The Burden of Suffering in Tinnitus PatientsPabloNo ratings yet
- Association of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyDocument8 pagesAssociation of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyQuentin LISANNo ratings yet
- Hyperacusis 3Document22 pagesHyperacusis 3FuninganaNo ratings yet
- Defining A Bobath ClinicalDocument2 pagesDefining A Bobath ClinicalAlicia HernandezNo ratings yet
- A Voice Rehabilitation Protocol With The SemioccludedDocument8 pagesA Voice Rehabilitation Protocol With The SemioccludedlksrangelNo ratings yet
- 1.patient EducationDocument7 pages1.patient EducationstuckinbedNo ratings yet
- Carroll 2Document19 pagesCarroll 2Anonymous JonAFVUi4No ratings yet
- 2016, Pedrosa Et Al, The Effectiveness of Comprehensive Voice, J VoiceDocument9 pages2016, Pedrosa Et Al, The Effectiveness of Comprehensive Voice, J VoiceCarol PaesNo ratings yet
- TimingVoiceTherapy PDFDocument7 pagesTimingVoiceTherapy PDFluxmansrikanthaNo ratings yet
- Rowena, Orig Article Effects of Type 3 ThyroplastyDocument5 pagesRowena, Orig Article Effects of Type 3 ThyroplastyLydia C JNo ratings yet
- Exposure Combined With Psychotherapy: A Treatment For Public Speaking AnxietyDocument19 pagesExposure Combined With Psychotherapy: A Treatment For Public Speaking AnxietyKayla LordNo ratings yet
- Exposure Combined With Psychotherapy: A Treatment For Public Speaking AnxietyDocument18 pagesExposure Combined With Psychotherapy: A Treatment For Public Speaking AnxietyKayla LordNo ratings yet
- Psicoterapia Online PDFDocument21 pagesPsicoterapia Online PDFCecilia Paulina Concha Gonzalez.No ratings yet
- Description of Patients Consulting The Voice Clinic Regarding Gender, Age, Occupational Status, and DiagnosisDocument20 pagesDescription of Patients Consulting The Voice Clinic Regarding Gender, Age, Occupational Status, and DiagnosisCarolina UrrutiaNo ratings yet
- Effectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDocument19 pagesEffectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDANIELA IGNACIA FERNÁNDEZ LEÓNNo ratings yet
- Detect Depression From Communication How Computer Vision Signal Processing and Sentiment Analysis Join ForcesDocument14 pagesDetect Depression From Communication How Computer Vision Signal Processing and Sentiment Analysis Join ForcesPaul HeatchoteNo ratings yet
- Literature Review Example Mental HealthDocument4 pagesLiterature Review Example Mental Healthea6mkqw2100% (1)
- THE Communication of Mental Health Information: A Comparison Opinions of Experts and Public With Mass Media Presentations'Document9 pagesTHE Communication of Mental Health Information: A Comparison Opinions of Experts and Public With Mass Media Presentations'Liridon1804No ratings yet
- Articulo 2Document24 pagesArticulo 2Daniela Rojas ramirezNo ratings yet
- Emotional Effects of SSRIsDocument8 pagesEmotional Effects of SSRIsteddypolNo ratings yet
- Jurnal 3Document8 pagesJurnal 3Alvi HarisdiwanaNo ratings yet
- Dimensional PsychopathologyFrom EverandDimensional PsychopathologyMassimo BiondiNo ratings yet
- Voice Therapy in The Context of The Covid-19Document44 pagesVoice Therapy in The Context of The Covid-19Isabel Monteiro GomesNo ratings yet
- Mecanismos Betabolicos de Fadiga VocalDocument11 pagesMecanismos Betabolicos de Fadiga VocalIsabel Monteiro GomesNo ratings yet
- Protocolo de ANLISE ESPCTOGRAFICADocument12 pagesProtocolo de ANLISE ESPCTOGRAFICAIsabel Monteiro GomesNo ratings yet
- Perceptual Voice Qualities Database Database CharacteristicsDocument9 pagesPerceptual Voice Qualities Database Database CharacteristicsIsabel Monteiro GomesNo ratings yet
- Are The Acoustic Measurements Reliable in The Assessment ofDocument13 pagesAre The Acoustic Measurements Reliable in The Assessment ofIsabel Monteiro GomesNo ratings yet
- Efeito Da Máscara Facial Na Produção de Voz Durante A Pandemia de COVID-19 Uma Revisão SistemáticaDocument31 pagesEfeito Da Máscara Facial Na Produção de Voz Durante A Pandemia de COVID-19 Uma Revisão SistemáticaIsabel Monteiro GomesNo ratings yet
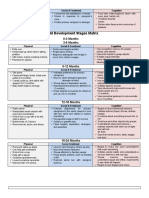
- Child Development Stages Matrix: 0-3 Months 3-6 MonthsDocument6 pagesChild Development Stages Matrix: 0-3 Months 3-6 MonthsJoenard Sadorra CabaelNo ratings yet
- Saja Drug Store Price List - 19!05!2024Document36 pagesSaja Drug Store Price List - 19!05!2024Sowrya Tej SunkaraNo ratings yet
- Exposing The Gender Lie - SM CP - 2023Document74 pagesExposing The Gender Lie - SM CP - 2023ElenaNo ratings yet
- Monitoring and Evaluation ME PlanDocument12 pagesMonitoring and Evaluation ME PlanMirAfghan GhulamiPoorNo ratings yet
- Johnson & Johnson Innovation Event Nov 23Document2 pagesJohnson & Johnson Innovation Event Nov 23Alessandro PedrioliNo ratings yet
- Pulsed Electro Magnetic Energy (PEME)Document9 pagesPulsed Electro Magnetic Energy (PEME)NATARAJAN KAVITHANo ratings yet
- Assessment of Orphan and Vulnerable Children Education Support in Nigeria (Document51 pagesAssessment of Orphan and Vulnerable Children Education Support in Nigeria (jamessabraham2No ratings yet
- Sthpatna1@yahoo Co inDocument6 pagesSthpatna1@yahoo Co inPramod JoshiNo ratings yet
- Facility ReadinDocument46 pagesFacility ReadinHabtamu Adare Habtamu AdareNo ratings yet
- The Role of The Anterior Region of The Medial Basal Hypothalamus in The Control of Ovulation and Sexual Behavior in SheepDocument12 pagesThe Role of The Anterior Region of The Medial Basal Hypothalamus in The Control of Ovulation and Sexual Behavior in SheepAh MagdyNo ratings yet
- Emergency Department PolicyDocument18 pagesEmergency Department PolicyKumar Gavali Suryanarayana100% (1)
- Nursing Research Test Bank (20 Questions) - Nurseslabs 2Document25 pagesNursing Research Test Bank (20 Questions) - Nurseslabs 2Danta Bien-AimeNo ratings yet
- PEWS Training Slides March2017Document36 pagesPEWS Training Slides March2017Altama L. Sidarta100% (1)
- Emotional Intelligence Digital Workbook - Class VersionDocument38 pagesEmotional Intelligence Digital Workbook - Class VersionmanickajaminNo ratings yet
- 7 Ways To Treat A Fever Naturally - Reader ModeDocument14 pages7 Ways To Treat A Fever Naturally - Reader Modeedward nodzoNo ratings yet
- The 10 Most Common Questions About HijamaDocument16 pagesThe 10 Most Common Questions About HijamaVashdev ValasaiNo ratings yet
- Skills Tests Units 1-10 A Answer Keys + Audio ScriptsDocument16 pagesSkills Tests Units 1-10 A Answer Keys + Audio ScriptsOla NiedźwiedzkaNo ratings yet
- Media Bulletin 11.07.2020 27 Pages English 491 KBDocument27 pagesMedia Bulletin 11.07.2020 27 Pages English 491 KBKathirasan RamalingamNo ratings yet
- Migmar Tsering (Mike) S ResumeDocument3 pagesMigmar Tsering (Mike) S Resumeapi-284044370No ratings yet
- NursalamDocument2 pagesNursalamAdipar AadNo ratings yet
- How Social Workers WomanDocument22 pagesHow Social Workers WomanSheroze DogerNo ratings yet
- 1119GB en Tip Top Heating Solution STL-RF4 Free of 0056Document7 pages1119GB en Tip Top Heating Solution STL-RF4 Free of 0056Guang ChenzNo ratings yet
- Tle10 - Afa - Agricropprod - q4 - Mod4 - Performing Housekeeping (2) - v4 (22 Pages)Document22 pagesTle10 - Afa - Agricropprod - q4 - Mod4 - Performing Housekeeping (2) - v4 (22 Pages)Manilyn Magdaraog100% (1)
- Manuscript 2 FinalDocument60 pagesManuscript 2 FinalKape Ka BaNo ratings yet
- Mona NasrallahDocument1 pageMona NasrallahWa3d HalabiNo ratings yet
- Psychology For UPSC MainsDocument16 pagesPsychology For UPSC Mainssske08No ratings yet
- 2 Gordons NCP Diagnostic Examination Lesson Plan FormatDocument9 pages2 Gordons NCP Diagnostic Examination Lesson Plan FormatKn VelasquezNo ratings yet