Download as pdf or txt
You might also like
- China's Toys IndustriesDocument22 pagesChina's Toys IndustriesPathar MayurNo ratings yet
- Waiting Lines and Qeuing Theory ModelDocument29 pagesWaiting Lines and Qeuing Theory ModelMadeline Gamboa De GuzmanNo ratings yet
- Implementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitDocument3 pagesImplementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitJHNo ratings yet
- Prone Position Pressure Sores in The COVID 19 PANDEMIC THE MADRID EXPERIENCEDocument8 pagesProne Position Pressure Sores in The COVID 19 PANDEMIC THE MADRID EXPERIENCEduckjqtNo ratings yet
- Efficiency of Prolonged Prone Positioning For Mechanically Ventilated Patients Infected With COVID-19Document11 pagesEfficiency of Prolonged Prone Positioning For Mechanically Ventilated Patients Infected With COVID-19Riyan NuelNo ratings yet
- Insights From An Interprofessional Post Covid 19 Rehabilitation Unit A Speech and Language Therapy and Respiratory Medicine PerspectiveDocument4 pagesInsights From An Interprofessional Post Covid 19 Rehabilitation Unit A Speech and Language Therapy and Respiratory Medicine PerspectiveValentina VallésNo ratings yet
- Feasibility and Physiological Effects of Prone Positioning in Non-Intubated Patients With Acute Respiratory Failure Due To COVID-19Document10 pagesFeasibility and Physiological Effects of Prone Positioning in Non-Intubated Patients With Acute Respiratory Failure Due To COVID-19Jakeline SilvaNo ratings yet
- Prone For COVID: Are You Awake?: EditorialDocument2 pagesProne For COVID: Are You Awake?: EditorialMahtosurup GodavarthyNo ratings yet
- Year in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsDocument13 pagesYear in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsRicardoNo ratings yet
- Rapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicDocument3 pagesRapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicRicardo BarreraNo ratings yet
- Anest, 12 ChaiwatDocument4 pagesAnest, 12 ChaiwatHainey GayleNo ratings yet
- NIRS in CovidDocument15 pagesNIRS in CovidljiljanarvicNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- Jurnal 2Document8 pagesJurnal 2DelisQurrotaA'yunNo ratings yet
- Proning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewDocument7 pagesProning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewCarlos ZepedaNo ratings yet
- COVID-19 Disease Invasive VentilationDocument8 pagesCOVID-19 Disease Invasive VentilationfikriafisNo ratings yet
- Prolonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and EffectiveDocument3 pagesProlonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and Effectivecarlos_julianNo ratings yet
- Respiratory Medicine Case ReportsDocument3 pagesRespiratory Medicine Case ReportsAzhari BaedlawiNo ratings yet
- Journal Pre-Proof: Journal of Critical CareDocument31 pagesJournal Pre-Proof: Journal of Critical CareMohammed Shuaib AhmedNo ratings yet
- Teman2015 PDFDocument8 pagesTeman2015 PDFAndi sutandiNo ratings yet
- Aerosol-Generating Procedures inDocument5 pagesAerosol-Generating Procedures inHaris WidodoNo ratings yet
- N 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CDocument18 pagesN 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CGeysel SuarezNo ratings yet
- Recommendations For Local-Regional Anesthesia During The COVID-19 PandemicDocument6 pagesRecommendations For Local-Regional Anesthesia During The COVID-19 PandemictitalitaNo ratings yet
- Via Aerea COVID 19Document3 pagesVia Aerea COVID 19zunarodriguezleoNo ratings yet
- Airway Management of Patients With COVID-19 by Specialist Tracheal Intubation TeamsDocument8 pagesAirway Management of Patients With COVID-19 by Specialist Tracheal Intubation TeamsFaisal ShamimNo ratings yet
- High Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Document5 pagesHigh Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Cesar C SNo ratings yet
- Retrospective Analysis of High Flow Nasal Therapy Un Covid 19 Related Moderate To Severe Hypoaxemic Respiratory FailureDocument11 pagesRetrospective Analysis of High Flow Nasal Therapy Un Covid 19 Related Moderate To Severe Hypoaxemic Respiratory FailureCesar C SNo ratings yet
- Redefining ARDS: A Paradigm Shift: Perspective Open AccessDocument7 pagesRedefining ARDS: A Paradigm Shift: Perspective Open Accesseyobhabtamu3No ratings yet
- Pi Is 0099176720304220Document10 pagesPi Is 0099176720304220yasintameganabilaNo ratings yet
- Comparison NIV and HFNCDocument7 pagesComparison NIV and HFNCRestu TriwulandaniNo ratings yet
- Optimizing Nursing Workload in The Intensive Care Unit During The COVID-19 Pandemic: Planning Prone PositioningDocument5 pagesOptimizing Nursing Workload in The Intensive Care Unit During The COVID-19 Pandemic: Planning Prone PositioningSiti NurjanahNo ratings yet
- Retrospective Analysis of High Flow Nasal Therapy in COVID-19-related Moderate - To - Severe Hypoxaemic Respiratory FailureDocument11 pagesRetrospective Analysis of High Flow Nasal Therapy in COVID-19-related Moderate - To - Severe Hypoxaemic Respiratory FailureJulieta EvangelistaNo ratings yet
- 2021 Article 63Document7 pages2021 Article 63RianNo ratings yet
- Outcomes Following Tracheostomy 2023Document10 pagesOutcomes Following Tracheostomy 2023ctsakalakisNo ratings yet
- Application of High-Fow Nasal CannulaDocument7 pagesApplication of High-Fow Nasal CannulaCLAUDIANo ratings yet
- Jurding KLP A Anes 3Document18 pagesJurding KLP A Anes 3mreza26No ratings yet
- Sancho2021 Article TracheostomyInPatientsWithCOVIDocument9 pagesSancho2021 Article TracheostomyInPatientsWithCOVIJavier BlancNo ratings yet
- Papazian2022 Article PronePositionInMechanicallyVenDocument4 pagesPapazian2022 Article PronePositionInMechanicallyVenA. RaufNo ratings yet
- Journal Appraisal 2Document14 pagesJournal Appraisal 2Norjetalexis Maningo CabreraNo ratings yet
- TQT Temprana en Covid 19Document31 pagesTQT Temprana en Covid 19Santiago GarcíaNo ratings yet
- Awake Prone Positioning in Acute Hypoxaemic Respiratory FailureDocument17 pagesAwake Prone Positioning in Acute Hypoxaemic Respiratory FailurePaulaNo ratings yet
- Sedation, Analgesia, and Paralysis in COVID-19 Patients in The Setting of Drug ShortagesDocument18 pagesSedation, Analgesia, and Paralysis in COVID-19 Patients in The Setting of Drug ShortagesPriscila Navarro MedinaNo ratings yet
- Heat and Moisture Exchanging Filter Pada Pasien COVID-19 YangDocument11 pagesHeat and Moisture Exchanging Filter Pada Pasien COVID-19 YangPerwiraNo ratings yet
- Heat and Moisture Exchanging Filter Pada Pasien COVID-19 YangDocument11 pagesHeat and Moisture Exchanging Filter Pada Pasien COVID-19 YangPerwiraNo ratings yet
- Research Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailureDocument7 pagesResearch Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailurewiwiNo ratings yet
- COVID-19 Management in HongKongDocument1 pageCOVID-19 Management in HongKongShahzad KamranNo ratings yet
- 3 DC 3Document8 pages3 DC 3astutikNo ratings yet
- HK MJ 208944Document3 pagesHK MJ 208944Bianca CaterinalisendraNo ratings yet
- Pzaa 175Document7 pagesPzaa 175RicardoNo ratings yet
- Perrone 2020 Operating Room Setup How To ImproveDocument5 pagesPerrone 2020 Operating Room Setup How To ImproveMahadi Hasan KhanNo ratings yet
- Possible Formation of Pulmonary Microthrombi in The Early Puerperium... Covid 19Document5 pagesPossible Formation of Pulmonary Microthrombi in The Early Puerperium... Covid 19Gerson OlivaresNo ratings yet
- 10 4187@respcare 07688Document21 pages10 4187@respcare 07688Hector VillamarinNo ratings yet
- An Intermediate Respiratory Care Unit in Every - 2023 - Archivos de BronconeumoDocument3 pagesAn Intermediate Respiratory Care Unit in Every - 2023 - Archivos de BronconeumoJuan Manuel Claros BustosNo ratings yet
- Safe Tracheostomy For Patients Severe Acute Respiratory: With SyndromeDocument3 pagesSafe Tracheostomy For Patients Severe Acute Respiratory: With SyndromeKenjiNo ratings yet
- High Flow Oxygen Therapy V Standard Care in InfantsDocument5 pagesHigh Flow Oxygen Therapy V Standard Care in InfantsJaque ArandaNo ratings yet
- Mechanical Ventilition COVID GuidelinesDocument7 pagesMechanical Ventilition COVID Guidelinesheba abuhelwaNo ratings yet
- A Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualDocument5 pagesA Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualMartha OktaviaNo ratings yet
- Prolonged Prone Position Ventilation Is Associated With ReducedDocument10 pagesProlonged Prone Position Ventilation Is Associated With ReducedFabiano CabralNo ratings yet
- Current Problems in Diagnostic Radiology 50 (2021) 284 287Document4 pagesCurrent Problems in Diagnostic Radiology 50 (2021) 284 287Leonard AcsinteNo ratings yet
- AnnalsATS 202007-803OCDocument9 pagesAnnalsATS 202007-803OCRianNo ratings yet
- Basics and modern practice of nasal high-flow therapyFrom EverandBasics and modern practice of nasal high-flow therapyRating: 5 out of 5 stars5/5 (1)
- Lung Transplantation: Evolving Knowledge and New HorizonsFrom EverandLung Transplantation: Evolving Knowledge and New HorizonsGanesh RaghuNo ratings yet
- Osteoarthritis and Cartilage OpenDocument9 pagesOsteoarthritis and Cartilage OpenJimena Vásquez RodríguezNo ratings yet
- Motor Imagery and Action Observation Following Immobilization-Induced Hypoactivity: A Narrative ReviewDocument7 pagesMotor Imagery and Action Observation Following Immobilization-Induced Hypoactivity: A Narrative ReviewJimena Vásquez RodríguezNo ratings yet
- International Immunopharmacology: Mohammad Shah Alam, Daniel M. Czajkowsky, Md. Aminul Islam, Md. Ataur RahmanDocument12 pagesInternational Immunopharmacology: Mohammad Shah Alam, Daniel M. Czajkowsky, Md. Aminul Islam, Md. Ataur RahmanJimena Vásquez RodríguezNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument6 pagesIntensive & Critical Care Nursing: Research ArticleJimena Vásquez RodríguezNo ratings yet
- Biomedicine & Pharmacotherapy: Danbi Jo, Gwangho Yoon, Oh Yoen Kim, Juhyun SongDocument8 pagesBiomedicine & Pharmacotherapy: Danbi Jo, Gwangho Yoon, Oh Yoen Kim, Juhyun SongJimena Vásquez RodríguezNo ratings yet
- Install Oracle RAC Database 12c R1 On Oracle Linux 6.4Document14 pagesInstall Oracle RAC Database 12c R1 On Oracle Linux 6.4hendrydatabaseNo ratings yet
- Albinoni-Tomaso-Adagio - Albinoni PDFDocument2 pagesAlbinoni-Tomaso-Adagio - Albinoni PDFTalise DoanNo ratings yet
- Notes MT Module I - KTUDocument47 pagesNotes MT Module I - KTURagesh Dudu100% (1)
- LAB 6 7-ElectroMechanical PneumaticDocument9 pagesLAB 6 7-ElectroMechanical PneumaticBien MedinaNo ratings yet
- OTC107207 OptiX NG WDM Optical Layer Data Configuration ISSUE 1Document28 pagesOTC107207 OptiX NG WDM Optical Layer Data Configuration ISSUE 1ARMAND NGUETSA SONKENGNo ratings yet
- API 686-Suction Line Slopes and ReducersDocument1 pageAPI 686-Suction Line Slopes and ReducersjpalauguillemNo ratings yet
- Harminder Singh SAP ID-500073564: Social BondsDocument5 pagesHarminder Singh SAP ID-500073564: Social Bondsharminder singhNo ratings yet
- Managing Organisation Case-Study-QuestionDocument4 pagesManaging Organisation Case-Study-QuestionFazida SalimNo ratings yet
- Sensex Rolling ReturnsDocument1 pageSensex Rolling Returnsmaheshtech76No ratings yet
- NFLDocument18 pagesNFLANIMESH JAINNo ratings yet
- Apt. Didik, Peluang Jasa Profesi ApotekerDocument22 pagesApt. Didik, Peluang Jasa Profesi ApotekerYudha PrasetyaNo ratings yet
- MuseScore4 Keyboard Shortcuts v1.0b Black WhiteDocument1 pageMuseScore4 Keyboard Shortcuts v1.0b Black WhiteJacob MorganNo ratings yet
- Beginners Guide To Prop Making V1-3Document22 pagesBeginners Guide To Prop Making V1-3Eduardo Nogales100% (5)
- Joy A. Gimeno, Complainant, vs. Atty. Paul Centillas Zaide, RespondentDocument3 pagesJoy A. Gimeno, Complainant, vs. Atty. Paul Centillas Zaide, RespondentLyleThereseNo ratings yet
- DO - s2009 - 54 - PTA GUIDELINES - RecognizedDocument11 pagesDO - s2009 - 54 - PTA GUIDELINES - RecognizedArthur AguilarNo ratings yet
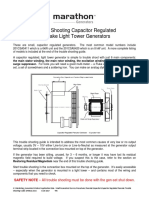
- Trouble Shooting Capacitor Regulated Pancake Light Tower GeneratorsDocument7 pagesTrouble Shooting Capacitor Regulated Pancake Light Tower GeneratorsBilly MecanizadoNo ratings yet
- DP CardReader 15065 DriversDocument1,068 pagesDP CardReader 15065 DriversGonzales Navarro100% (1)
- Submitted By-Rashmi Parmar (8601) Trisha Sinha Roy (8629) Sanchari Mohanta (8631) Raunak Shirali (8609) Karan Khot (8615) Swapnil Kulkarni (8625)Document38 pagesSubmitted By-Rashmi Parmar (8601) Trisha Sinha Roy (8629) Sanchari Mohanta (8631) Raunak Shirali (8609) Karan Khot (8615) Swapnil Kulkarni (8625)Vipul PartapNo ratings yet
- 01 Concept of ProbabilityDocument3 pages01 Concept of ProbabilityThapaa Lila0% (1)
- Performance of Recron-3s Fiber On Black Cotton SoilDocument6 pagesPerformance of Recron-3s Fiber On Black Cotton SoilInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Basic Electrical, Automation, and Instrumentation.Document4 pagesBasic Electrical, Automation, and Instrumentation.Foaad HawarNo ratings yet
- Missile Guidance LawsDocument10 pagesMissile Guidance LawsAkanksha221291No ratings yet
- The Dual in LPDocument17 pagesThe Dual in LPShreeyesh MenonNo ratings yet
- Foundation Lecture (Abdulhafiz)Document4 pagesFoundation Lecture (Abdulhafiz)desigandNo ratings yet
- Academic Year 2020/2021 Term 3Document3 pagesAcademic Year 2020/2021 Term 3braa haririNo ratings yet
- (Vacancies May Increase (Or) Decrease at The Time of Recruitment) Eligibility: For Assistant Professors in Ap Medical Education ServicesDocument4 pages(Vacancies May Increase (Or) Decrease at The Time of Recruitment) Eligibility: For Assistant Professors in Ap Medical Education ServicesseravanakumarNo ratings yet
- Diesel Power Plant PresentationDocument30 pagesDiesel Power Plant Presentationjlaguilar67% (3)
- GBS Project Service Center: Financial Process Monthly Reporting (IPPF)Document16 pagesGBS Project Service Center: Financial Process Monthly Reporting (IPPF)smgalloNo ratings yet