Download as docx, pdf, or txt
You might also like
- Patient Privacy PolicyDocument2 pagesPatient Privacy PolicyKharisma RosaNo ratings yet
- Chat GPTDocument13 pagesChat GPTsuly maniyahNo ratings yet
- Journal of Accounting Education: Ken H. Guo, Brenda L. EschenbrennerDocument10 pagesJournal of Accounting Education: Ken H. Guo, Brenda L. EschenbrennerCandel0% (1)
- Clinical Focus MAM Melba Alano NCM 112Document6 pagesClinical Focus MAM Melba Alano NCM 112Melba Alano100% (1)
- Policy - Co-2-034 Independent Double Check High Alert MedicationsDocument8 pagesPolicy - Co-2-034 Independent Double Check High Alert MedicationsTravel JunkyNo ratings yet
- Moh-Uae Pharmacy Federal Law in English1Document23 pagesMoh-Uae Pharmacy Federal Law in English1Dr-Usman Khan100% (1)
- Pharmacy Policy and ProceduresDocument15 pagesPharmacy Policy and ProcedureswilliamNo ratings yet
- Security Bank Sample Loan App FormDocument1 pageSecurity Bank Sample Loan App FormJennifer DeleonNo ratings yet
- IsolationDocument5 pagesIsolationapi-394727583No ratings yet
- Consent For Dialysis FormDocument4 pagesConsent For Dialysis FormBalayet HossenNo ratings yet
- Job Description, Duties and Responsibilities of Regulatory Compliance Officer v2040622Document1 pageJob Description, Duties and Responsibilities of Regulatory Compliance Officer v2040622Meycauayan DialysisNo ratings yet
- Memorandum, Assignment #4Document1 pageMemorandum, Assignment #4wsilversNo ratings yet
- Project SynopsisDocument15 pagesProject SynopsisVigneshNo ratings yet
- Barcode Pharmaceutical System Main Project Work Isiyaku AuwaluDocument30 pagesBarcode Pharmaceutical System Main Project Work Isiyaku Auwalumustapha muhammad AuwalNo ratings yet
- Post Activity Report - Area 2Document7 pagesPost Activity Report - Area 2Irene P. MartinezNo ratings yet
- Standard Operating ProceduresDocument12 pagesStandard Operating ProceduresakumaraoNo ratings yet
- Electronic PrescribingDocument5 pagesElectronic PrescribingWally RedsNo ratings yet
- Online Doctor's Appointment: Project ProposalDocument8 pagesOnline Doctor's Appointment: Project ProposalR -BrotHERsNo ratings yet
- Pharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010Document85 pagesPharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010James LindonNo ratings yet
- Use Case Diagram For Pharmacy Management SystemDocument3 pagesUse Case Diagram For Pharmacy Management SystemAnand Krishna100% (1)
- Prescription ModelDocument7 pagesPrescription ModelAbhijeet PatilNo ratings yet
- Proper Disposal of Expired or Unwanted DrugsDocument9 pagesProper Disposal of Expired or Unwanted Drugscarramrod2No ratings yet
- Mewa Hospital Software SystemDocument163 pagesMewa Hospital Software SystemAlmutwafy AbdulrehmanNo ratings yet
- Merits and DemeritsDocument2 pagesMerits and Demeritssyeda zee100% (1)
- OLGMS Covid 19 GuidelinesDocument23 pagesOLGMS Covid 19 Guidelinesιωαναθαν ρααγασNo ratings yet
- INTEGRATED APPLICATION FORM - BIO PROCARE With DataDocument4 pagesINTEGRATED APPLICATION FORM - BIO PROCARE With Datakim roqueNo ratings yet
- DOH AO No. 56 S. 1989Document10 pagesDOH AO No. 56 S. 1989attysteveNo ratings yet
- Scope of Tele-Pharmacists in A Pandemic PDFDocument7 pagesScope of Tele-Pharmacists in A Pandemic PDFjahangirNo ratings yet
- Ra 9502Document22 pagesRa 9502Are Pee EtcNo ratings yet
- Srs0263 Pharmacy Practice 1: Topic 2: Writing PrescriptionDocument17 pagesSrs0263 Pharmacy Practice 1: Topic 2: Writing PrescriptionMohammad Badrul AminNo ratings yet
- Dental Software: Presented By: Project GuideDocument65 pagesDental Software: Presented By: Project GuideSai KotianNo ratings yet
- Telemedicine Informed ConsentDocument2 pagesTelemedicine Informed ConsentEric Geronimo100% (1)
- Medical Transcription Marketing PlanDocument12 pagesMedical Transcription Marketing PlanMaria Victoria Negru100% (1)
- CPG of PhilhealthDocument31 pagesCPG of PhilhealthMV Davao ToursNo ratings yet
- Chapter 1 PPT 1 (Prescription)Document55 pagesChapter 1 PPT 1 (Prescription)Shumaila QadirNo ratings yet
- BFADDocument4 pagesBFADKc Ganda BNo ratings yet
- UC EC 00 0449 Legal Medical Record PolicyDocument19 pagesUC EC 00 0449 Legal Medical Record PolicyHamss AhmedNo ratings yet
- Generic MedicinesDocument16 pagesGeneric MedicinesAnn Christine C. ChuaNo ratings yet
- Guidelines For Product RecallDocument18 pagesGuidelines For Product RecallSenthamaraiShanmughamNo ratings yet
- VCT ManualDocument70 pagesVCT ManualNay Lin HtikeNo ratings yet
- Project Plan DocumentDocument15 pagesProject Plan DocumentashagrieNo ratings yet
- Pharmacy TechnicianDocument10 pagesPharmacy TechnicianMUHAMMAD IDREESNo ratings yet
- Training and Development Policy - Version 4 - FinalDocument10 pagesTraining and Development Policy - Version 4 - FinalCindy MuladziNo ratings yet
- Hospitals and EconomicsDocument27 pagesHospitals and EconomicsUnivsan Agustin EmployeesunionNo ratings yet
- WWW - Chd11.doh - Gov.ph - Rledweb - Checklist of Reqmt. For RDS - HP - RONPDDocument4 pagesWWW - Chd11.doh - Gov.ph - Rledweb - Checklist of Reqmt. For RDS - HP - RONPDlorraine_cuaNo ratings yet
- Doh Policies and GuidelinesDocument48 pagesDoh Policies and GuidelinesMigz Mendez100% (1)
- Republic Act. 5921 - Pharmacy LawDocument14 pagesRepublic Act. 5921 - Pharmacy LawSunshine_Bacla_4275100% (1)
- Design and Implementation of An Online PDocument14 pagesDesign and Implementation of An Online PRetaj LibyaNo ratings yet
- Dangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFDocument11 pagesDangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFdesmond100% (1)
- Ao 43 S 1999Document92 pagesAo 43 S 1999Ella RivaNo ratings yet
- Standard Operating Procedure of Voluntary Counseling and Testing Services in Community and Mobile ServicesDocument62 pagesStandard Operating Procedure of Voluntary Counseling and Testing Services in Community and Mobile ServicesThomas AJITHNo ratings yet
- Complete Drug FormularyDocument96 pagesComplete Drug FormularyRPh Krishna Chandra JagritNo ratings yet
- TX & RX Sample CodeDocument8 pagesTX & RX Sample CodeMadianita EstradaNo ratings yet
- 05 Sop For Use of Office Inventory and EquipmentDocument3 pages05 Sop For Use of Office Inventory and EquipmentRio Simatupang100% (2)
- Ao2019 0002 PDFDocument17 pagesAo2019 0002 PDFLen SabayNo ratings yet
- P3infection Control PracticesDocument7 pagesP3infection Control Practicesprivate3wardNo ratings yet
- A SepsisDocument5 pagesA SepsisAi KogaNo ratings yet
- Cytotoxic Drug ReconstitutionDocument7 pagesCytotoxic Drug Reconstitutioniqhwan riatNo ratings yet
- Checklist of Standard Precautions For Infection Control in HospitalsDocument2 pagesChecklist of Standard Precautions For Infection Control in HospitalsSanjay KadamNo ratings yet
- Surveillance, Prevention & Control of Infections Standard PrecautionsDocument7 pagesSurveillance, Prevention & Control of Infections Standard Precautionschgl10No ratings yet
- Saliva Collection Covid-19 Precautions 9-2020Document10 pagesSaliva Collection Covid-19 Precautions 9-2020sanaNo ratings yet
- PMLS Lec Lesson 1Document53 pagesPMLS Lec Lesson 1Janna EchavezNo ratings yet
- Otprotocols 140307000050 Phpapp02Document76 pagesOtprotocols 140307000050 Phpapp02Melba AlanoNo ratings yet
- Policies and Procedures On Isolation of Nosocomial InfectionDocument8 pagesPolicies and Procedures On Isolation of Nosocomial InfectionMelba AlanoNo ratings yet
- Chapter 6 WoundhealingDocument41 pagesChapter 6 WoundhealingMelba AlanoNo ratings yet
- Berea College B Ed FP Teaching SubmissionDocument520 pagesBerea College B Ed FP Teaching SubmissionGbengaNo ratings yet
- Tri 21 DMP 002Document3 pagesTri 21 DMP 002adi sihombingNo ratings yet
- Material Safety Data Sheet: J218 Breaker J218Document8 pagesMaterial Safety Data Sheet: J218 Breaker J218sajad gohariNo ratings yet
- COCOMO II ExampleDocument26 pagesCOCOMO II ExampleQuốc ĐạiNo ratings yet
- Red Hat Jboss Enterprise Application Platform 7.1: Getting Started GuideDocument61 pagesRed Hat Jboss Enterprise Application Platform 7.1: Getting Started Guidesomanath padhyNo ratings yet
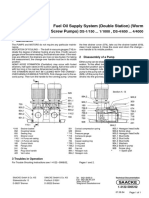
- Fuel Oil Supply System (Double Station) (Worm Screw Pumps) : DS 1/150 ... 1/1000, DS 4/650 ... 4/4000Document1 pageFuel Oil Supply System (Double Station) (Worm Screw Pumps) : DS 1/150 ... 1/1000, DS 4/650 ... 4/4000徐玉坤No ratings yet
- Conclusion and Future EnhancementDocument2 pagesConclusion and Future EnhancementHelloprojectNo ratings yet
- Barangay CertificateDocument4 pagesBarangay CertificateMark Vincent SolisNo ratings yet
- Accounting Q&ADocument6 pagesAccounting Q&AIftikharNo ratings yet
- Anaesthetic Considerations in Polytrauma PatientsDocument8 pagesAnaesthetic Considerations in Polytrauma PatientsMileidys LopezNo ratings yet
- All About Me WorkbookDocument18 pagesAll About Me WorkbookYssa Camarillas100% (1)
- Analysing Mouse and Pen Flick GesturesDocument6 pagesAnalysing Mouse and Pen Flick GesturesHarini RaoNo ratings yet
- NJM072B/082B/072/082: Dual J-Fet Input Operational AmplifierDocument5 pagesNJM072B/082B/072/082: Dual J-Fet Input Operational Amplifieryuni supriatinNo ratings yet
- Salen WWE Offer LetterDocument3 pagesSalen WWE Offer LetterHeel By NatureNo ratings yet
- READMEDocument25 pagesREADMENate ClarkNo ratings yet
- United States Court of Appeals, Eleventh CircuitDocument12 pagesUnited States Court of Appeals, Eleventh CircuitScribd Government DocsNo ratings yet
- Cable Incendio 2X18 Awg S/P: UL1424FPLRDocument1 pageCable Incendio 2X18 Awg S/P: UL1424FPLR04143510504gallucciNo ratings yet
- New York City Subway: THE BronxDocument1 pageNew York City Subway: THE BronxPrincesa LizNo ratings yet
- 001 2012 4 b-3Document114 pages001 2012 4 b-3dikahunguNo ratings yet
- Munger Talk at Harvard-WestlakeDocument10 pagesMunger Talk at Harvard-WestlakeSantangel's Review100% (7)
- SDL 11Document14 pagesSDL 11Sharmila BalaNo ratings yet
- Curriculum VitaeDocument3 pagesCurriculum Vitaenotapernota101100% (2)
- Criminal Law II - Quasi OffensesDocument2 pagesCriminal Law II - Quasi OffensesJanine Prelle DacanayNo ratings yet
- KickStart 19Document2 pagesKickStart 19Venu GopalNo ratings yet
- Temidayo Cybercrime ReportDocument13 pagesTemidayo Cybercrime ReportMAYOWA ADEBAYONo ratings yet
- CA ProjectDocument21 pagesCA Projectkalaswami100% (1)
- Answer Script - ISDocument21 pagesAnswer Script - ISanishjoseph007No ratings yet
- VLANS and Other HardwareDocument20 pagesVLANS and Other HardwareVishal KushwahaNo ratings yet
- MarxismDocument13 pagesMarxismFelicia AtmadjaNo ratings yet