Download as docx, pdf, or txt
You might also like
- ExamPreview RN 111722Document148 pagesExamPreview RN 111722jhajj0% (3)
- Abnormal Psychology Perspectives DSM 5 Update 7th Edition Whitbourne Test BankDocument30 pagesAbnormal Psychology Perspectives DSM 5 Update 7th Edition Whitbourne Test Bankformeretdoveshipx9yi8100% (32)
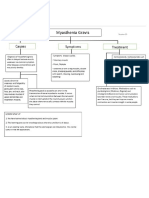
- Lymphedema and Lipedema Nutrition Guide: Foods, Vitamins, Minerals, and Supplements - Chuck EhrlichDocument6 pagesLymphedema and Lipedema Nutrition Guide: Foods, Vitamins, Minerals, and Supplements - Chuck EhrlichmafawepyNo ratings yet
- 2020-Biochem-Activity-17 - CLINICAL CHEMISTRYDocument42 pages2020-Biochem-Activity-17 - CLINICAL CHEMISTRYGabrielle John HernaezNo ratings yet
- Uterine Fibroids Case StudyDocument38 pagesUterine Fibroids Case StudyFiona Cheryl Amsterdam80% (5)
- 17 Habbatus Sauda BenefitsDocument7 pages17 Habbatus Sauda BenefitsDins PutrajayaNo ratings yet
- ANEMIAPPTDocument42 pagesANEMIAPPTLord Allen B. GomezNo ratings yet
- Pathogenesis & LTPDocument9 pagesPathogenesis & LTPFatima Medriza DuranNo ratings yet
- Complete Blood CountDocument5 pagesComplete Blood CountShella CondezNo ratings yet
- Case StudyDocument7 pagesCase StudyJoan Manzon MallariNo ratings yet
- Hematopoietic and LymphaticDocument4 pagesHematopoietic and LymphaticPaul Rageev Mikkhael FulloNo ratings yet
- Week 4 Lo Wo Rabu Fms4Document8 pagesWeek 4 Lo Wo Rabu Fms4KesyaNo ratings yet
- IDA PPT FinalDocument26 pagesIDA PPT FinalYen-yen FaveNo ratings yet
- Exploring Inflammatory SyndromeDocument6 pagesExploring Inflammatory SyndromeEmi ValcovNo ratings yet
- Laboratory and Diagnostic ResultsDocument9 pagesLaboratory and Diagnostic ResultsHaru DogNo ratings yet
- Abnormalities of Haematopoiesis and Blood DisordersDocument51 pagesAbnormalities of Haematopoiesis and Blood DisordersRenad AlharbiNo ratings yet
- Villanueva Adriane Noel Rot1 Chunk 1Document25 pagesVillanueva Adriane Noel Rot1 Chunk 1Adriane VillanuevaNo ratings yet
- PBL Report ThalassemiaDocument10 pagesPBL Report Thalassemiasarah_amigurlz88100% (2)
- List Blood Tests Performed As Part of A CBCDocument9 pagesList Blood Tests Performed As Part of A CBCamiosaNo ratings yet
- N 5315 Advaned Pathophysiology Anemia TranscriptDocument9 pagesN 5315 Advaned Pathophysiology Anemia TranscriptllukelawrenceNo ratings yet
- Hematopoeitic System: Nsoh Fofang Mia Bios 2021 Edited by Laouna Fru Supervised by DR DimitriDocument66 pagesHematopoeitic System: Nsoh Fofang Mia Bios 2021 Edited by Laouna Fru Supervised by DR DimitriVerla MfeerNo ratings yet
- Laboratory Activity 2 (Nd59) Biochemical Assessment of The Nutritional Status in The Clinical Setting Case Study 1Document11 pagesLaboratory Activity 2 (Nd59) Biochemical Assessment of The Nutritional Status in The Clinical Setting Case Study 1LESLIE ANN MESOLISNo ratings yet
- Template UKOOADocument5 pagesTemplate UKOOAFeliciaSetiawanNo ratings yet
- Anemia: Our Lady of Fatima University College of NursingDocument21 pagesAnemia: Our Lady of Fatima University College of NursingPOTENCIANA MAROMANo ratings yet
- Physio PBLDocument13 pagesPhysio PBLCeejhay LeeNo ratings yet
- Diagnostic Procedure Description of The Procedure Purpose of The Procedure Date of The Procedure Reference Findings ImplicationsDocument7 pagesDiagnostic Procedure Description of The Procedure Purpose of The Procedure Date of The Procedure Reference Findings ImplicationsDizah Faye OsboroNo ratings yet
- Reference/normal Values Result Interpretation What Have Caused The Abnormality/ Purpose/NIDocument5 pagesReference/normal Values Result Interpretation What Have Caused The Abnormality/ Purpose/NIKristian Karl Bautista Kiw-isNo ratings yet
- Blood Disorders 11Document50 pagesBlood Disorders 11Purnendu ParidaNo ratings yet
- Hemeostasis 1Document52 pagesHemeostasis 1Abdo HaiderNo ratings yet
- Physiology of Blood 1Document66 pagesPhysiology of Blood 1Hiruni FernandoNo ratings yet
- Polycythemia VeraDocument4 pagesPolycythemia VeraAllyson VillarNo ratings yet
- Sickle Cell Anemia 2007Document25 pagesSickle Cell Anemia 2007R-o-N-n-e-lNo ratings yet
- Modul6 Lbm2-Aulia SifanaDocument41 pagesModul6 Lbm2-Aulia SifanapademotNo ratings yet
- Complete Blood CountDocument18 pagesComplete Blood CountNazih MominNo ratings yet
- Asynch Act Abi3213 - CelestialDocument4 pagesAsynch Act Abi3213 - Celestialjuliancelestial08No ratings yet
- Blood 2022Document36 pagesBlood 2022Hassan mohamad Al-bayateNo ratings yet
- PDF 20220223 180117 0000Document13 pagesPDF 20220223 180117 0000Ankit YadavNo ratings yet
- Unit Iv Body Fluid AnalysisDocument8 pagesUnit Iv Body Fluid AnalysispriyagerardNo ratings yet
- Laboratory Result Final Na JudDocument11 pagesLaboratory Result Final Na JudMarissa AsimNo ratings yet
- Polycythemia VeraDocument8 pagesPolycythemia VeraSalam ZeeshanNo ratings yet
- Unida-Medical Surgical ExamDocument6 pagesUnida-Medical Surgical ExamAnabel UnidaNo ratings yet
- Why Get Tested?: AnaemiaDocument4 pagesWhy Get Tested?: Anaemiashasha009No ratings yet
- Pathophysiology of NonDocument5 pagesPathophysiology of Nonanonymousanon703No ratings yet
- Case History: PBL 2 Failure To ThriveDocument9 pagesCase History: PBL 2 Failure To ThriveNazratun Choudhury BornyNo ratings yet
- CML GoutDocument14 pagesCML GoutIbby ImyadelnaNo ratings yet
- CBC Lab Results FinalDocument2 pagesCBC Lab Results FinalEunice MañalacNo ratings yet
- Blood Dr. Devesh Palharya FBDocument4 pagesBlood Dr. Devesh Palharya FBAkash MittalNo ratings yet
- Blood Notes PDFDocument13 pagesBlood Notes PDFsyedurrahman855No ratings yet
- ICU LabDocument5 pagesICU Labanne_valencia_3No ratings yet
- Case Study CholelithiasisDocument14 pagesCase Study Cholelithiasisb_faye20No ratings yet
- LaboratoryDocument9 pagesLaboratorymonique_maniquisNo ratings yet
- GRP 5 Hematopoietic System ImlanDocument49 pagesGRP 5 Hematopoietic System ImlanSharie Grace ImlanNo ratings yet
- BloodDocument39 pagesBloodAbdul HafeezNo ratings yet
- 1 Red Blood Cells Anemia and PolycythemiaDocument43 pages1 Red Blood Cells Anemia and PolycythemiaGeevee Naganag VentulaNo ratings yet
- High-Yield Physiology Notes-Points For USMLE Step 1 & FCPS Part 1Document11 pagesHigh-Yield Physiology Notes-Points For USMLE Step 1 & FCPS Part 1SHAKEEL1991No ratings yet
- Assignment 1 CDocument6 pagesAssignment 1 Cu21md1009No ratings yet
- As A Student, How Do You Maintain A Healthy Lifestyle?: Topic 1: Health Care Activity 1Document4 pagesAs A Student, How Do You Maintain A Healthy Lifestyle?: Topic 1: Health Care Activity 1Elijah Mae MundocNo ratings yet
- San Pedro College: A Case Study inDocument15 pagesSan Pedro College: A Case Study inKyla ValenciaNo ratings yet
- Ezra M. Darubday NCP Sample Surgical WardDocument9 pagesEzra M. Darubday NCP Sample Surgical WardEzra Miguel DarundayNo ratings yet
- Aubf EeDocument26 pagesAubf EeAlleah MancillaNo ratings yet
- White Blood Cells and Differential: Normal Value Purpose and IndicationDocument1 pageWhite Blood Cells and Differential: Normal Value Purpose and IndicationKyla CasugaNo ratings yet
- BloodDocument18 pagesBloodMichael HabibNo ratings yet
- Paroxysmal Nocturnal Hemoglobinuria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParoxysmal Nocturnal Hemoglobinuria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Polycythemia Vera, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPolycythemia Vera, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Drugstudy Case1Document10 pagesDrugstudy Case1jovan teopizNo ratings yet
- Case Study 2Document12 pagesCase Study 2jovan teopizNo ratings yet
- For The Student Learning Activity4Document1 pageFor The Student Learning Activity4jovan teopizNo ratings yet
- For The Student Learning Activity3Document1 pageFor The Student Learning Activity3jovan teopizNo ratings yet
- Essay On Readiness For Exercise, Goals Setting, Prioritizing, ControllingDocument2 pagesEssay On Readiness For Exercise, Goals Setting, Prioritizing, Controllingjovan teopizNo ratings yet
- For The Student Learning Activity2Document2 pagesFor The Student Learning Activity2jovan teopizNo ratings yet
- For The Student Learning Activity1Document1 pageFor The Student Learning Activity1jovan teopizNo ratings yet
- JovannDocument6 pagesJovannjovan teopizNo ratings yet
- Whole Case1 DoneDocument5 pagesWhole Case1 Donejovan teopizNo ratings yet
- Fdar Case 1Document2 pagesFdar Case 1jovan teopizNo ratings yet
- HematomaDocument2 pagesHematomajovan teopizNo ratings yet
- Maternal P1Document18 pagesMaternal P1jovan teopizNo ratings yet
- MODULEDocument12 pagesMODULEjovan teopizNo ratings yet
- Family Nursing Care PlanDocument1 pageFamily Nursing Care Planjovan teopizNo ratings yet
- HK55Document3 pagesHK55jovan teopizNo ratings yet
- Fetal PresentationDocument3 pagesFetal Presentationjovan teopizNo ratings yet
- Maternal 4Document5 pagesMaternal 4jovan teopizNo ratings yet
- CVDocument1 pageCVjovan teopizNo ratings yet
- IiiiiiDocument3 pagesIiiiiijovan teopizNo ratings yet
- Group 6 (Sas 16-20)Document7 pagesGroup 6 (Sas 16-20)jovan teopizNo ratings yet
- mc2 p1 ExamDocument12 pagesmc2 p1 Examjovan teopizNo ratings yet
- FNCP and RankingDocument2 pagesFNCP and Rankingjovan teopizNo ratings yet
- 100 Beats Per Minute. Many DifferentDocument4 pages100 Beats Per Minute. Many Differentjovan teopizNo ratings yet
- CHN Long Quiz 1Document11 pagesCHN Long Quiz 1jovan teopizNo ratings yet
- Community ProfilingDocument2 pagesCommunity Profilingjovan teopizNo ratings yet
- CVDocument1 pageCVjovan teopizNo ratings yet
- CHN Long Quiz 2Document11 pagesCHN Long Quiz 2jovan teopizNo ratings yet
- Cesarean Section CASEDocument32 pagesCesarean Section CASEjovan teopizNo ratings yet
- Community ReflectionDocument2 pagesCommunity Reflectionjovan teopizNo ratings yet
- Cesarean SectionDocument31 pagesCesarean Sectionjovan teopizNo ratings yet
- Qhse Documents-Heat Stress - A Summertime Hazard Toolbox TalksDocument3 pagesQhse Documents-Heat Stress - A Summertime Hazard Toolbox TalksLawrence adeleke OmisakinNo ratings yet
- Nejmcpc 1909624Document10 pagesNejmcpc 1909624SrivarrdhiniNo ratings yet
- Heart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureDocument12 pagesHeart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureAshutosh SinghNo ratings yet
- Test Bank For Exceptional Learners An Introduction To Special Education 12 e 12th Edition Daniel P Hallahan James M Kauffman Paige C PullenDocument31 pagesTest Bank For Exceptional Learners An Introduction To Special Education 12 e 12th Edition Daniel P Hallahan James M Kauffman Paige C PullenPeter Fleming100% (32)
- English 19033 NurhikmahDocument2 pagesEnglish 19033 Nurhikmahnur hikmah hasanahNo ratings yet
- Neurotransmitters What They Are, Functions & TypesDocument13 pagesNeurotransmitters What They Are, Functions & TypesIncognito 000No ratings yet
- The Spread of Coronavirus (Covid-19) .Document1 pageThe Spread of Coronavirus (Covid-19) .KashifntcNo ratings yet
- Introductory ConceptDocument5 pagesIntroductory ConceptYanyan CainongNo ratings yet
- First Description of TVD in Basset HoundDocument4 pagesFirst Description of TVD in Basset HoundFlorencia SeneseNo ratings yet
- Viral Hepatitis: References: Harrisons Infectious Disease 2 Ed., Oxford Handbook of Microbiology and IdDocument58 pagesViral Hepatitis: References: Harrisons Infectious Disease 2 Ed., Oxford Handbook of Microbiology and IdMohammad Emad Al MadadhaNo ratings yet
- Periodontal Problems in ChildrenDocument21 pagesPeriodontal Problems in ChildrenEslam HafezNo ratings yet
- Bull Fertility: The Importance of The Bull in Herd FertilityDocument5 pagesBull Fertility: The Importance of The Bull in Herd FertilitySaad JavedNo ratings yet
- Journal of Infection and Chemotherapy: Case ReportDocument4 pagesJournal of Infection and Chemotherapy: Case ReportEllese SayNo ratings yet
- Bornstein, M. M., Cionca, N., & Mombelli, A. (2009)Document17 pagesBornstein, M. M., Cionca, N., & Mombelli, A. (2009)tefaNo ratings yet
- Unseen PassageDocument7 pagesUnseen PassageVinay OjhaNo ratings yet
- برزنتيشن هديك١Document22 pagesبرزنتيشن هديك١Abdallah AlquranNo ratings yet
- Reconocimiento Del Acv CLINISC 2012Document21 pagesReconocimiento Del Acv CLINISC 2012Camilo GomezNo ratings yet
- Covid 19Document42 pagesCovid 19ok100% (3)
- DRUG STUDY (Ceftriaxone)Document2 pagesDRUG STUDY (Ceftriaxone)Avianna CalliopeNo ratings yet
- Study Guide 1-INTRODUCTION TO MYCOLOGYDocument6 pagesStudy Guide 1-INTRODUCTION TO MYCOLOGYAna Vanissa BendolNo ratings yet
- Ob ToDocument2 pagesOb TotycheNo ratings yet
- Antibiotic Guidelines For AdultsDocument9 pagesAntibiotic Guidelines For AdultsVarshini Tamil SelvanNo ratings yet
- TRINTELLIX Product Monograph EnglishDocument45 pagesTRINTELLIX Product Monograph EnglishEstmar ValentinoNo ratings yet
- Rectosigmoid Carcinoma: Department of SurgeryDocument19 pagesRectosigmoid Carcinoma: Department of SurgeryHana FauziNo ratings yet
- The Case History Scheme: Kyiv State Hospital Pediatric Department 1Document8 pagesThe Case History Scheme: Kyiv State Hospital Pediatric Department 1Fatemeh BemanaNo ratings yet
- Hemşirelik Bölümü Ders İçerikleri (İngilizce)Document52 pagesHemşirelik Bölümü Ders İçerikleri (İngilizce)teomanbilimNo ratings yet