Download as pdf or txt
You might also like
- Nursing Care Plan - Impaired Gas ExchangeDocument3 pagesNursing Care Plan - Impaired Gas ExchangeYum C86% (65)
- Unit - 8Document44 pagesUnit - 8prathibaNo ratings yet
- Emt PosterDocument1 pageEmt PosterDrThant Zin Tun50% (2)
- Perspectives of Women Participating in A Cervical Cancer Screening Campaign With Community-Based HPV Self-Sampling in Rural Western Kenya. A Qualitative StudyDocument10 pagesPerspectives of Women Participating in A Cervical Cancer Screening Campaign With Community-Based HPV Self-Sampling in Rural Western Kenya. A Qualitative StudyAdrián ÁvilaNo ratings yet
- Ijgo 89 S2 2005 04Document9 pagesIjgo 89 S2 2005 04Solihin HasnanNo ratings yet
- Effective Screening25Document3 pagesEffective Screening25ponekNo ratings yet
- Cxca Planning Appro Prog GuideDocument91 pagesCxca Planning Appro Prog GuideYudha Pratama PNo ratings yet
- Evidence-Based, Alternative Cervical Cancer Screening Approaches in Low-Resource SettingsDocument6 pagesEvidence-Based, Alternative Cervical Cancer Screening Approaches in Low-Resource Settingschica_asNo ratings yet
- Improving Intervention Design To Promote Cervical Cancer Screening Among Hard-To-Reach Women Assessing Beliefs and Predicting Individual Attendance Probabilities in Bogotá, ColombiaDocument12 pagesImproving Intervention Design To Promote Cervical Cancer Screening Among Hard-To-Reach Women Assessing Beliefs and Predicting Individual Attendance Probabilities in Bogotá, Colombiaandrea sanabria pedrazaNo ratings yet
- A Comparative Analysis of ClassificationDocument12 pagesA Comparative Analysis of ClassificationSharmi BhatNo ratings yet
- Accelerating Cervical Cancer Prevention and Control in China To Achieve Cervical Cancer Elimination Strategy ObjectivesDocument3 pagesAccelerating Cervical Cancer Prevention and Control in China To Achieve Cervical Cancer Elimination Strategy ObjectivesBillNo ratings yet
- Ket ProposalDocument37 pagesKet ProposalEneyew BirhanNo ratings yet
- Research Paper Cervical CancerDocument5 pagesResearch Paper Cervical Cancergz8bjzmj100% (1)
- Cie 10Document11 pagesCie 10Gabriella MGNo ratings yet
- Factors Influencing Cervical Cancer Re-Screening in A Semi-Rural Health District of Cameroon: A Cohort StudyDocument10 pagesFactors Influencing Cervical Cancer Re-Screening in A Semi-Rural Health District of Cameroon: A Cohort StudyJasmin PutriNo ratings yet
- An Enhanced Ensemble Diagnosis of Cervical Cancer: A Pursuit of Machine Intelligence Towards Sustainable HealthDocument15 pagesAn Enhanced Ensemble Diagnosis of Cervical Cancer: A Pursuit of Machine Intelligence Towards Sustainable HealthMahmudur Rahman27No ratings yet
- Pamj 22 26Document8 pagesPamj 22 26Yosie Yulanda PutraNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleirdaNo ratings yet
- Ca de MamaDocument39 pagesCa de MamaMedicina Lo MejorNo ratings yet
- Breast and Gynecological Cancers - An Integrated Approach For Screening and Early Diagnosis in Developing Countries (PDFDrive)Document365 pagesBreast and Gynecological Cancers - An Integrated Approach For Screening and Early Diagnosis in Developing Countries (PDFDrive)Bharti Pant Gahtori100% (1)
- 5 PDFDocument15 pages5 PDFnorazizah rizkaNo ratings yet
- Breast Cancer Issues in Developing Countries: An Overview of The Breast Health Global InitiativeDocument8 pagesBreast Cancer Issues in Developing Countries: An Overview of The Breast Health Global InitiativeenviNo ratings yet
- Research Article Breast Cancer Screening: Knowledge, Attitudes, and Practices Among Female University Students in The GambiaDocument8 pagesResearch Article Breast Cancer Screening: Knowledge, Attitudes, and Practices Among Female University Students in The GambiaBahredin AbdellaNo ratings yet
- Parts of A ReportDocument12 pagesParts of A ReportVenice De los ReyesNo ratings yet
- Thesis On Breast Cancer DetectionDocument4 pagesThesis On Breast Cancer Detectionafkodkedr100% (2)
- Evaluation of The Effectiveness of High-Risk Human Papilloma Self-Sampling Test For Cervical Cancer Screening in BoliviaDocument9 pagesEvaluation of The Effectiveness of High-Risk Human Papilloma Self-Sampling Test For Cervical Cancer Screening in BoliviaJAIME CLAUDIO VILLARROEL SALINASNo ratings yet
- A Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesDocument17 pagesA Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesYukiko CalimutanNo ratings yet
- A Protocol For A Cluster Randomized Controlled Trial of A Self Help Psycho Education Programme To Reduce Diagnosis Delay in Women With Breast Cancer Symptoms in IndonesiaDocument8 pagesA Protocol For A Cluster Randomized Controlled Trial of A Self Help Psycho Education Programme To Reduce Diagnosis Delay in Women With Breast Cancer Symptoms in Indonesiaflorentina dianNo ratings yet
- AndersonDocument4 pagesAndersonCreativ PinoyNo ratings yet
- Effective Screening14Document9 pagesEffective Screening14ponekNo ratings yet
- Deep Learning MamaDocument29 pagesDeep Learning MamaPJ GsNo ratings yet
- 2020 Article 668Document11 pages2020 Article 668MilliNo ratings yet
- Research ArticleDocument14 pagesResearch ArticleShubhaDavalgiNo ratings yet
- UntitledDocument12 pagesUntitledLauren FavelaNo ratings yet
- Nurses and Midwives Knowledge Attitudes and AcceDocument11 pagesNurses and Midwives Knowledge Attitudes and AcceGeorge Junior AdomakoNo ratings yet
- The Pregnancy and FertilityDocument11 pagesThe Pregnancy and FertilityLussi IndahNo ratings yet
- Carol Langley On USG Support For Addressing Cervical CancerDocument19 pagesCarol Langley On USG Support For Addressing Cervical CancerJhpiego100% (1)
- Colorectal Cancer Screening: It Is Not Time For A Radical ShiftDocument2 pagesColorectal Cancer Screening: It Is Not Time For A Radical Shiftm_manuela2002No ratings yet
- Breast Cancer ReflectionDocument4 pagesBreast Cancer ReflectionCAJES NOLINo ratings yet
- Patient Education and Counseling: Joelle I. Rosser, Betty Njoroge, Megan J. HuchkoDocument6 pagesPatient Education and Counseling: Joelle I. Rosser, Betty Njoroge, Megan J. HuchkoTrysna Ayu SukardiNo ratings yet
- World Journal of Surgical OncologyDocument9 pagesWorld Journal of Surgical OncologyNikita BowmanNo ratings yet
- Research Paper About Cervical CancerDocument4 pagesResearch Paper About Cervical Cancergw1357jx100% (1)
- Research ArticleDocument10 pagesResearch ArticleSrideviRaviNo ratings yet
- Colorectal Cancer Screening and Quality MeasuresDocument10 pagesColorectal Cancer Screening and Quality MeasuresmnovemberNo ratings yet
- Klafke 2015Document22 pagesKlafke 2015Irna SulistiyaniNo ratings yet
- The Feasibility of Community Level Interventions For Pre-Eclampsia in South Asia and Sub-Saharan Africa: A Mixed-Methods DesignDocument15 pagesThe Feasibility of Community Level Interventions For Pre-Eclampsia in South Asia and Sub-Saharan Africa: A Mixed-Methods DesignjohariyahNo ratings yet
- ManuscriptDocument18 pagesManuscriptfxbukenyaNo ratings yet
- Summary Recommendations of IFCPC 2021 Consensus Satellite Meeting On 25th JuneDocument7 pagesSummary Recommendations of IFCPC 2021 Consensus Satellite Meeting On 25th JuneVijay KumarNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptYosua_123No ratings yet
- Knowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Women Visiting Primary Health Care Centres in BahrainDocument6 pagesKnowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Women Visiting Primary Health Care Centres in BahrainAnonymous N74eaOhdfkNo ratings yet
- EBM2Document8 pagesEBM2ica ssNo ratings yet
- Developing A Web-Based Shared Decision-Making Tool For Fertility Preservation Among Reproductive-Age Women With Breast CancerDocument10 pagesDeveloping A Web-Based Shared Decision-Making Tool For Fertility Preservation Among Reproductive-Age Women With Breast Cancer郭竹瑩No ratings yet
- Correlates of Cervical Cancer Screening Participation, Intention and Self-Efficacy Among Muslim Women in Southern GhanaDocument11 pagesCorrelates of Cervical Cancer Screening Participation, Intention and Self-Efficacy Among Muslim Women in Southern GhanaAdrián ÁvilaNo ratings yet
- Knowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonDocument17 pagesKnowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonEditor IJTSRDNo ratings yet
- Mammography Screening in Switzerland: Limited Evidence From Limited DataDocument13 pagesMammography Screening in Switzerland: Limited Evidence From Limited DataVinuPrakashJ.No ratings yet
- Improving Mammography ScreeningDocument8 pagesImproving Mammography ScreeningsylviaramisNo ratings yet
- Healthpolicy Brief Cervical Cancer Screening PhilippinesDocument13 pagesHealthpolicy Brief Cervical Cancer Screening PhilippinesIya JoyNo ratings yet
- Research 09Document16 pagesResearch 09Nandini SeetharamanNo ratings yet
- The Effect of Knowledge On Uptake of Breast Cancer Prevention Modalities Among Women in Kyadondo County, UgandaDocument8 pagesThe Effect of Knowledge On Uptake of Breast Cancer Prevention Modalities Among Women in Kyadondo County, Ugandalailatus sakinahNo ratings yet
- Using Blended-Learning Approach To Improve Education On Clinical Pathways For Breast Cancer Management in Nigeria: A Research ProtocolDocument5 pagesUsing Blended-Learning Approach To Improve Education On Clinical Pathways For Breast Cancer Management in Nigeria: A Research ProtocolasclepiuspdfsNo ratings yet
- s12905 018 0701 2Document12 pagess12905 018 0701 2Erisha Mae BalagbaganNo ratings yet
- Cancer Screening in the Developing World: Case Studies and Strategies from the FieldFrom EverandCancer Screening in the Developing World: Case Studies and Strategies from the FieldMadelon L. FinkelNo ratings yet
- Conium MacDocument3 pagesConium MacSur E JahanNo ratings yet
- Stroke 2013 Qureshi S67 9Document4 pagesStroke 2013 Qureshi S67 9Herlinda Dwi NingrumNo ratings yet
- UntitledDocument47 pagesUntitledJi CaratNo ratings yet
- Use of Antibiotics For Acute Respiratory Infection (ARI) in Puskesmas Karang Rejo, TarakanDocument7 pagesUse of Antibiotics For Acute Respiratory Infection (ARI) in Puskesmas Karang Rejo, TarakanAugust WattimenaNo ratings yet
- 21-CoV10069-Ruslan Bin HashimDocument1 page21-CoV10069-Ruslan Bin HashimHERU EKO PRAYOGONo ratings yet
- Bethesda SystemDocument186 pagesBethesda SystemJoyce Pardo FernandezNo ratings yet
- NURSING CARE PLAN - CholeraDocument2 pagesNURSING CARE PLAN - Choleraderic87% (30)
- Treatment MGRDocument12 pagesTreatment MGRMod AntbugNo ratings yet
- Proximal Femur Fractures: Sulita Turaganiwai s130364Document26 pagesProximal Femur Fractures: Sulita Turaganiwai s130364Wālē NandNo ratings yet
- Esthetic Management of Space and Soft Tissue Deficiencies in Implant Therapy Combined Orthodontic-Mucogingival ApproachDocument16 pagesEsthetic Management of Space and Soft Tissue Deficiencies in Implant Therapy Combined Orthodontic-Mucogingival Approachfloressam2000No ratings yet
- 1NUR8 ABRIO Summative AssessmentDocument3 pages1NUR8 ABRIO Summative AssessmentKYRA CHEYENNE NICHOLLE ABRIO100% (1)
- DiphtheriaDocument30 pagesDiphtheriaBinayaNo ratings yet
- Venous Thromboembolism (VTE) : Quality DepartmentDocument28 pagesVenous Thromboembolism (VTE) : Quality DepartmentDIGITAL 143No ratings yet
- Continuous EEG Monitoring in The Intensive Care UnDocument7 pagesContinuous EEG Monitoring in The Intensive Care UnSara MendesNo ratings yet
- DM Self AssessmentDocument6 pagesDM Self AssessmentruguNo ratings yet
- Surgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRDocument6 pagesSurgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRIuliana MoiseNo ratings yet
- Diagnosis and Treatment of Vulvar Precancerous Lesions and CancerDocument4 pagesDiagnosis and Treatment of Vulvar Precancerous Lesions and CancerSyahril FauziNo ratings yet
- Foundation of Nursing Practice Exam For Nursing Process Physical and Health Assessment and Routine ProceduresDocument24 pagesFoundation of Nursing Practice Exam For Nursing Process Physical and Health Assessment and Routine ProceduresAdrian Miguel100% (1)
- Tacrolimus in DermatologyDocument4 pagesTacrolimus in DermatologyDimas PrajagoptaNo ratings yet
- Paracetamol - Infusion: Presentation DoseDocument2 pagesParacetamol - Infusion: Presentation Dosecupri yantiNo ratings yet
- Final Case Study 3rd EditionDocument50 pagesFinal Case Study 3rd EditionKrizhel Mirja CawasNo ratings yet
- Drug Study JrodDocument8 pagesDrug Study JrodGaez ﭢ UlpindoNo ratings yet
- Pertemuan 9 Arista PDFDocument12 pagesPertemuan 9 Arista PDFNi Putu aristaNo ratings yet
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Document10 pagesDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiNo ratings yet
- (English (Auto-Generated) ) Vaccines Vs Reality Dr. Andrew Kaufman (DownSub - Com)Document133 pages(English (Auto-Generated) ) Vaccines Vs Reality Dr. Andrew Kaufman (DownSub - Com)Indira MaycellaNo ratings yet
- Research Proposal First Draft (Adamu Moti)Document25 pagesResearch Proposal First Draft (Adamu Moti)ODAA TUBENo ratings yet
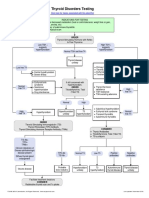
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Quick Guide For OTs People Recovering From COVID-19Document17 pagesQuick Guide For OTs People Recovering From COVID-19Mihaela SerbanNo ratings yet