Download as pdf or txt
You might also like
- Case 29 Milwaukee Regional Health System - XLSX 3Document14 pagesCase 29 Milwaukee Regional Health System - XLSX 3codyabner1986No ratings yet
- Foot Posture IndexDocument19 pagesFoot Posture IndexSara Barros100% (2)
- Stuxnet and Its Hidden Lessons On The Ethics of CyberweaponsDocument9 pagesStuxnet and Its Hidden Lessons On The Ethics of CyberweaponsprofcameloNo ratings yet
- PNG 2 VssDocument7 pagesPNG 2 VssCarlos CarrilNo ratings yet
- Journal of Foot and Ankle Research: Normative Values For The Foot Posture IndexDocument9 pagesJournal of Foot and Ankle Research: Normative Values For The Foot Posture IndexAnup PednekarNo ratings yet
- Morrison & Ferrari (2009) - Inter-Rater Reliability of The Foot Posture Index (FPI-6) in The Assessment of The Paediatric FootDocument6 pagesMorrison & Ferrari (2009) - Inter-Rater Reliability of The Foot Posture Index (FPI-6) in The Assessment of The Paediatric FootxtraqrkyNo ratings yet
- Foot and Ankle Questions On The Orthopaedic In-Training Examination: Analysis of Content, Reference, and PerformanceDocument10 pagesFoot and Ankle Questions On The Orthopaedic In-Training Examination: Analysis of Content, Reference, and PerformanceZia Ur RehmanNo ratings yet
- Foot and Ankle Questions On The OrthopaedicDocument9 pagesFoot and Ankle Questions On The OrthopaedicichkhuyNo ratings yet
- A Review of The Foot Function Index and The Foot Function Index - RevisedDocument37 pagesA Review of The Foot Function Index and The Foot Function Index - RevisedKSJDLVKDNVNo ratings yet
- 2014 Article 55 PDFDocument19 pages2014 Article 55 PDFvinaNo ratings yet
- 31 PDFDocument4 pages31 PDFMonalisa MeidaniaNo ratings yet
- The Foot Posture Index: Six Item Version FPI-6 User Guide and ManualDocument19 pagesThe Foot Posture Index: Six Item Version FPI-6 User Guide and ManualBryan AlimNo ratings yet
- Reliability and Validity of Foot Posture Index (FPI 6) For Evaluating Foot Posture in Participants With Low Back PainDocument10 pagesReliability and Validity of Foot Posture Index (FPI 6) For Evaluating Foot Posture in Participants With Low Back PainSaheba SafiqueNo ratings yet
- Occupational Risk Factors For Osteoarthritis of The Knee: A Meta-AnalysisDocument11 pagesOccupational Risk Factors For Osteoarthritis of The Knee: A Meta-Analysisfidatahir93No ratings yet
- Group 7 Outcome MeasuresDocument6 pagesGroup 7 Outcome MeasuresANNE RIEN DIGALNo ratings yet
- Rooij Et Al-2016-Arthritis Care & ResearchDocument12 pagesRooij Et Al-2016-Arthritis Care & ResearchJennifer JaneNo ratings yet
- Lee 2018Document7 pagesLee 2018Kings AndrewNo ratings yet
- A 5-Year Review of Statistical Methods Presented in The Journal of Foot & AnkleDocument4 pagesA 5-Year Review of Statistical Methods Presented in The Journal of Foot & AnkleElizabeth CollinsNo ratings yet
- Measurement Properties of OakhqolDocument6 pagesMeasurement Properties of OakhqolRita RahmawatiNo ratings yet
- 8 Aboutorabi A 2017 1Document10 pages8 Aboutorabi A 2017 1Felipe Iturra JaraNo ratings yet
- A Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryDocument10 pagesA Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryRini MaghfirahNo ratings yet
- Ability To Sit and Rise From The Floor As A Predictor of All-Cause MortalityDocument7 pagesAbility To Sit and Rise From The Floor As A Predictor of All-Cause MortalityTainá PerezNo ratings yet
- Congenital Talipes EquinovarusDocument7 pagesCongenital Talipes EquinovarusSri WidiatmiNo ratings yet
- Confirmatory Factor Analysis of VISA P Scale and Measur 2017 Journal of SporDocument7 pagesConfirmatory Factor Analysis of VISA P Scale and Measur 2017 Journal of SporSisi WeeraNo ratings yet
- Preventive Medicine ReportsDocument9 pagesPreventive Medicine ReportsDzihan NabilahNo ratings yet
- Toe Walking Treatment ReviewDocument13 pagesToe Walking Treatment ReviewJohnNo ratings yet
- Foot Posture Index (Development and Validation, 2006)Document10 pagesFoot Posture Index (Development and Validation, 2006)ximogbNo ratings yet
- Evidence-Based Perspective On CP Rehabilitation, Anttilla, ThesisDocument168 pagesEvidence-Based Perspective On CP Rehabilitation, Anttilla, ThesisAntonio AlvarezNo ratings yet
- Development Process and Psychometric Testing of Foot Health Assessment InstrumentDocument13 pagesDevelopment Process and Psychometric Testing of Foot Health Assessment Instrumentkarin24No ratings yet
- 2017 Article 1388Document10 pages2017 Article 1388MonikaNo ratings yet
- PQ Art 48163-10Document11 pagesPQ Art 48163-10jayadevanNo ratings yet
- Os Suportes Externos Melhoram o Equilíbrio Dinâmico em Pacientes Com Instabilidade Crônica Do Tornozelo - Uma Meta-AnáliseDocument19 pagesOs Suportes Externos Melhoram o Equilíbrio Dinâmico em Pacientes Com Instabilidade Crônica Do Tornozelo - Uma Meta-AnáliseThiago Penna ChavesNo ratings yet
- Amputation 3Document8 pagesAmputation 3Tarushi TanwarNo ratings yet
- KWW 098Document9 pagesKWW 098Sergio AlumendaNo ratings yet
- Do Knee Abnormalities Visualised On MRI Explain Knee Pain in Knee OsteoarthritisDocument9 pagesDo Knee Abnormalities Visualised On MRI Explain Knee Pain in Knee OsteoarthritisRosaneLacerdaNo ratings yet
- Efectiveness of An AFO On Walking in Patients With StrokeDocument12 pagesEfectiveness of An AFO On Walking in Patients With Strokejasoneric0718No ratings yet
- Diagnostic Accuracy of Physical Examination Tests of The Ankle-Foot Complex - A Systematic Review.Document11 pagesDiagnostic Accuracy of Physical Examination Tests of The Ankle-Foot Complex - A Systematic Review.CambriaChicoNo ratings yet
- Effectiveness of The Open Bite Treatment in Growing Children and Adolescents. A Systematic ReviewDocument14 pagesEffectiveness of The Open Bite Treatment in Growing Children and Adolescents. A Systematic ReviewMaria SilvaNo ratings yet
- The Effectiveness of Pre-Operative Exercise PhysiotherapyDocument24 pagesThe Effectiveness of Pre-Operative Exercise PhysiotherapyebookNo ratings yet
- Randomized Controlled Trial Quality in Pediatric Physical TherapyDocument14 pagesRandomized Controlled Trial Quality in Pediatric Physical TherapyMelinda Fila BethaNo ratings yet
- Gait & PostureDocument8 pagesGait & PostureEhrik Javier Huamancaja PalominoNo ratings yet
- Soucie 2010Document8 pagesSoucie 2010AuroraNo ratings yet
- 1 s2.0 S0049017215002310 MainDocument7 pages1 s2.0 S0049017215002310 Maingck85fj8pnNo ratings yet
- Physical Therapy in Sport: Cornelia Neuhaus, Christian Appenzeller-Herzog, Oliver FaudeDocument10 pagesPhysical Therapy in Sport: Cornelia Neuhaus, Christian Appenzeller-Herzog, Oliver FaudeBreechesNo ratings yet
- 6 Sun 2020Document9 pages6 Sun 2020doctor.code2003No ratings yet
- Bone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsDocument5 pagesBone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsmuklisrivaiNo ratings yet
- 2017 Rationale For Prescription, and Effectiveness Of, Upper Limb Orthotic Intervention For Children With Cerebral Palsy - A Systematic ReviewDocument12 pages2017 Rationale For Prescription, and Effectiveness Of, Upper Limb Orthotic Intervention For Children With Cerebral Palsy - A Systematic ReviewJulian Caro MorenoNo ratings yet
- The Effect of Different Dephts of Medial Heel Skive On Plantar PressuresDocument10 pagesThe Effect of Different Dephts of Medial Heel Skive On Plantar PressuresAlberto Jesús CamposNo ratings yet
- Applied Sciences: Gait Kinematics Analysis of Flatfoot AdultsDocument11 pagesApplied Sciences: Gait Kinematics Analysis of Flatfoot AdultsdhirenNo ratings yet
- La Relación Entre La Postura Del Pie y La Cinemática de Las Extremidades Inferiores Durante LaDocument10 pagesLa Relación Entre La Postura Del Pie y La Cinemática de Las Extremidades Inferiores Durante LaDayana SánchezNo ratings yet
- The Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewDocument7 pagesThe Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewIJAR JOURNALNo ratings yet
- Hes Sari 2012Document6 pagesHes Sari 2012bbvnrsh279No ratings yet
- 5 The Pattern and Technique in The Clinical Evaluation of The Adult Hip The Common Physical Examination Tests of Hip Specialists 1353528420Document12 pages5 The Pattern and Technique in The Clinical Evaluation of The Adult Hip The Common Physical Examination Tests of Hip Specialists 1353528420César ArveláezNo ratings yet
- Gulle H. 2023. Prediciting Outcome Plantar Heel Pain. Systematic Review Prognostic FactorsDocument13 pagesGulle H. 2023. Prediciting Outcome Plantar Heel Pain. Systematic Review Prognostic FactorsJavier MartinNo ratings yet
- Children 09 00531 v2Document10 pagesChildren 09 00531 v2Jam Ali PakistanNo ratings yet
- Exercise and Progressive Supranuclear Palsy: The Need For Explicit Exercise ReportingDocument9 pagesExercise and Progressive Supranuclear Palsy: The Need For Explicit Exercise ReportingNathaly CantorNo ratings yet
- Jer 17 4 226Document8 pagesJer 17 4 226Magno FilhoNo ratings yet
- Foot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDocument18 pagesFoot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDonna KrawczykNo ratings yet
- Psychometric Properties of Four Common Clinical Tests For Assessing Hamstring Flexibility in Young Adults.Document8 pagesPsychometric Properties of Four Common Clinical Tests For Assessing Hamstring Flexibility in Young Adults.Santiago Mondragon RiosNo ratings yet
- The Effectiveness of Shoe Insoles For The Prevention and Treatment of Low BackDocument19 pagesThe Effectiveness of Shoe Insoles For The Prevention and Treatment of Low BackhasNo ratings yet
- 8 Bookshelf - NBK493367-1 PDFDocument175 pages8 Bookshelf - NBK493367-1 PDFandi dirhanNo ratings yet
- Concise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersFrom EverandConcise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersNo ratings yet
- 2018-09-01 Classic Land RoverDocument100 pages2018-09-01 Classic Land RovergufffNo ratings yet
- ACCNTNGDocument6 pagesACCNTNGJarren BasilanNo ratings yet
- 4 Types of Essay WritingDocument2 pages4 Types of Essay WritingkikiNo ratings yet
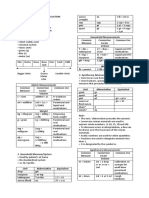
- Metric System Common Measure Conversion Factor Common UseDocument4 pagesMetric System Common Measure Conversion Factor Common UseMarielle ChuaNo ratings yet
- Product Demo Feedback FormDocument1 pageProduct Demo Feedback FormVarunSharmaNo ratings yet
- Building Up Good Mental Health: Guidelines Based On Existing KnowledgeDocument6 pagesBuilding Up Good Mental Health: Guidelines Based On Existing KnowledgerowanpurdyNo ratings yet
- Managed Pressure Drilling Modeling & Simulation (A Case Study)Document8 pagesManaged Pressure Drilling Modeling & Simulation (A Case Study)Mejbahul SarkerNo ratings yet
- 420 Economic Survey Chapter 11 Thalinomics IndiashastraDocument1 page420 Economic Survey Chapter 11 Thalinomics IndiashastraKarambir Singh DhayalNo ratings yet
- University of The Philippines Open University Faculty of Management and Development Studies Master of Management ProgramDocument10 pagesUniversity of The Philippines Open University Faculty of Management and Development Studies Master of Management ProgramRoldan TalaugonNo ratings yet
- Complete Research Ch1 5Document57 pagesComplete Research Ch1 5Angelie Regie J EstorqueNo ratings yet
- Department of Education: Guitnangbayan Elementary SchoolDocument4 pagesDepartment of Education: Guitnangbayan Elementary SchoolGuitnang bayan es 109487100% (1)
- Threshold Heteroskedastic Models: Jean-Michel ZakoianDocument25 pagesThreshold Heteroskedastic Models: Jean-Michel ZakoianLuis Bautista0% (1)
- Perils of PlagiarismDocument3 pagesPerils of Plagiarismapi-306005383No ratings yet
- Emerging Global Trends in Iot: (Internet of Things)Document28 pagesEmerging Global Trends in Iot: (Internet of Things)EkoPandaraNo ratings yet
- UGEB2362 Course Outline 2023-24Document5 pagesUGEB2362 Course Outline 2023-24Suki PunNo ratings yet
- Ethics in Accounting A Decision Making Approach 1St Edition Klein Solutions Manual Full Chapter PDFDocument40 pagesEthics in Accounting A Decision Making Approach 1St Edition Klein Solutions Manual Full Chapter PDFLisaMartinykfz100% (9)
- Zairi 2018Document6 pagesZairi 2018Vinu KohliNo ratings yet
- Multiplexing Demultiplexing PDFDocument7 pagesMultiplexing Demultiplexing PDFمحمد عليNo ratings yet
- General Definition of Sag and Tension in Electrical Transmission LinesDocument11 pagesGeneral Definition of Sag and Tension in Electrical Transmission Linesdskymaximus67% (3)
- Psycholinguistics: What It Is? - Language, Speech and Communication.Document4 pagesPsycholinguistics: What It Is? - Language, Speech and Communication.Edo PrasetiaNo ratings yet
- Feeder Protection REF615: Product GuideDocument40 pagesFeeder Protection REF615: Product Guidenzinga DHA SantralNo ratings yet
- Buying Guide Truck Scales EN v11 Low PDFDocument80 pagesBuying Guide Truck Scales EN v11 Low PDFBồ Công AnhNo ratings yet
- Non CariousDocument4 pagesNon CariousUpasana BhandariNo ratings yet
- Ananya - Visa SopDocument5 pagesAnanya - Visa SopSehnoor KaurNo ratings yet
- Customers Satisfaction On ATMDocument33 pagesCustomers Satisfaction On ATMabdullahi shafiuNo ratings yet
- Chromium Metal: Standard Specification ForDocument2 pagesChromium Metal: Standard Specification ForJerry Bean100% (1)
- Floyd Electrical StatementDocument5 pagesFloyd Electrical Statementshane.ramirez1980No ratings yet