Download as pdf or txt
You might also like
- AMPATH Nepal RFP 2024Document12 pagesAMPATH Nepal RFP 2024hamrovisionnewsNo ratings yet
- Ebook PDF Twenty Lessons in Environmental Sociology 2nd PDFDocument41 pagesEbook PDF Twenty Lessons in Environmental Sociology 2nd PDFalicia.mclaughlin973100% (38)
- Healing Lyme: Buhner Core Protocol (Unofficial) PDFDocument4 pagesHealing Lyme: Buhner Core Protocol (Unofficial) PDFSteluța DrâmbuNo ratings yet
- OptiOne Service & Parts-EDocument334 pagesOptiOne Service & Parts-EDavid Vera100% (1)
- Material Safety Data Sheet: KOMATSU Supercoolant AF-NAC (50/50 Pre-Diluted)Document5 pagesMaterial Safety Data Sheet: KOMATSU Supercoolant AF-NAC (50/50 Pre-Diluted)Thais Roberta CamposNo ratings yet
- BPCL Case StudyDocument10 pagesBPCL Case StudyRimjhim ShrivastavaNo ratings yet
- LA Metro MapDocument1 pageLA Metro MapAlbert Barba0% (1)
- SSP 540 The Passat 2015 SCR and AdBlueDocument40 pagesSSP 540 The Passat 2015 SCR and AdBluekiki50% (2)
- CG Weight and Body Fat Standards Program ManualDocument189 pagesCG Weight and Body Fat Standards Program ManualcarneyjillNo ratings yet
- Wiley - Abnormal Psychology - The Science and Treatment of Psychological Disorders, 14th Edition - 978-1-119-36228-9Document3 pagesWiley - Abnormal Psychology - The Science and Treatment of Psychological Disorders, 14th Edition - 978-1-119-36228-9Freelancing WorkNo ratings yet
- SiddhaStandardTreatmentGuidelines PDFDocument654 pagesSiddhaStandardTreatmentGuidelines PDFBalakrishna Gopinath100% (3)
- 2018.10 International QuestionsDocument52 pages2018.10 International QuestionsHuseynaga AbasovNo ratings yet
- 2018.11 US QuestionsDocument67 pages2018.11 US QuestionsHuseynaga AbasovNo ratings yet
- Handrail Blocking InstructionsDocument1 pageHandrail Blocking InstructionsAlejandro Bravo CastilloNo ratings yet
- Fast Reroute For Triple Play Networks: Building Smart Broadband NetworksDocument21 pagesFast Reroute For Triple Play Networks: Building Smart Broadband NetworkspowenjeNo ratings yet
- Fed Grad Rate Category 2122Document27 pagesFed Grad Rate Category 2122Chris WolfNo ratings yet
- OLX (OLX Praca) : ProblemDocument1 pageOLX (OLX Praca) : ProblemjulkaluksaNo ratings yet
- B1AIP30 - ProjectplanDocument21 pagesB1AIP30 - ProjectplanArwin SomoNo ratings yet
- Pareto AnalysisDocument2 pagesPareto AnalysisAJITPALNo ratings yet
- Common Core State StandardsDocument2 pagesCommon Core State StandardsMary MaxwellNo ratings yet
- Sub-Soil Investigation For Bridge Structure and Approach RoadDocument1 pageSub-Soil Investigation For Bridge Structure and Approach Roadshafiq_05No ratings yet
- Product Collection: THE Asia PacificDocument32 pagesProduct Collection: THE Asia PacificarotechjabarNo ratings yet
- SW USB Pro Series - Setup Guide: Extron Cable Cubby 100Document4 pagesSW USB Pro Series - Setup Guide: Extron Cable Cubby 100Iqbal TelkomNo ratings yet
- D4B80405EF4-ODIS Service IntroductionDocument6 pagesD4B80405EF4-ODIS Service IntroductionNestor LucianiNo ratings yet
- Zone 5: Adah Stadium Al Nahda Dubai A Irpor TFZ Usais Etisala TDocument1 pageZone 5: Adah Stadium Al Nahda Dubai A Irpor TFZ Usais Etisala Tpareen9No ratings yet
- Gea Membrane Filtration Brochure For Dairy IndustryDocument24 pagesGea Membrane Filtration Brochure For Dairy Industryjoaquincasaklen50% (2)
- Resin Solutions: 3formDocument2 pagesResin Solutions: 3formheshamNo ratings yet
- Amco Meva 825Document2 pagesAmco Meva 825Juan BonottiNo ratings yet
- VACCPDocument21 pagesVACCPSherylNo ratings yet
- ADG Lamdaya 2018 RevisiDocument24 pagesADG Lamdaya 2018 RevisiJohnJonhChitNo ratings yet
- WWW Acte in AWS Training in HyderabadDocument18 pagesWWW Acte in AWS Training in Hyderabadsophiamerlin1996No ratings yet
- Manual de Instruções Volkswagen Polo Classic (1996) (513 Páginas)Document2 pagesManual de Instruções Volkswagen Polo Classic (1996) (513 Páginas)ciceroNo ratings yet
- The Golf 2013 Running Gear and Four-Wheel Drive ConceptDocument32 pagesThe Golf 2013 Running Gear and Four-Wheel Drive ConceptAntónio FernandesNo ratings yet
- Educational Booklet EBIDocument9 pagesEducational Booklet EBIEleonice MoreiraNo ratings yet
- Prosp Temperatursensoren B217 GB 19Document28 pagesProsp Temperatursensoren B217 GB 19GonzaloNo ratings yet
- 1.0-l 3-Cylinder TSI Engine: Design and FunctionDocument28 pages1.0-l 3-Cylinder TSI Engine: Design and FunctionAlin Mirea100% (1)
- Using Installed Gain To Improve Valve Selection and Valves & Specialty Metal Materials - CE - October 2010 PDFDocument8 pagesUsing Installed Gain To Improve Valve Selection and Valves & Specialty Metal Materials - CE - October 2010 PDFonizuka-t2263No ratings yet
- LZDZ Issue 3 2017 PDFDocument32 pagesLZDZ Issue 3 2017 PDFLEDOMNo ratings yet
- Volks Fox & Gol G5 - G6 Diagrams Eletrico BCMSM - 28Document369 pagesVolks Fox & Gol G5 - G6 Diagrams Eletrico BCMSM - 28Jonas Dos Santos Andrade0% (1)
- Students Graphics 1Document1 pageStudents Graphics 1Humanist English ManNo ratings yet
- Online Hotel Management SystemDocument49 pagesOnline Hotel Management SystemShibly100% (2)
- Tallest StructuresDocument1 pageTallest StructuresNathia NavamaniNo ratings yet
- Rudrakshi SharmaDocument11 pagesRudrakshi SharmaPrashant A UNo ratings yet
- Epntibgðajdieqvol Edlsßitena Xmutasal Rsuk Ra:L Extþkmbg S WDocument1 pageEpntibgðajdieqvol Edlsßitena Xmutasal Rsuk Ra:L Extþkmbg S WMakarasounNo ratings yet
- OV V5.Xx Operator's (English) LF Branded-A - ENDocument194 pagesOV V5.Xx Operator's (English) LF Branded-A - ENDavid VeraNo ratings yet
- Froyotogo Financial ProjectionDocument2 pagesFroyotogo Financial Projectionapi-381631440No ratings yet
- Baby Bug Nov 17Document1 pageBaby Bug Nov 17RocioDelPilarGilNo ratings yet
- Membrane Filtration in The Dairy IndustryDocument24 pagesMembrane Filtration in The Dairy IndustryPeter IosifidisNo ratings yet
- Graph ReportDocument1 pageGraph ReportYến NhiNo ratings yet
- Graph ReportDocument1 pageGraph Report1wwww1974No ratings yet
- Inst Intl 1Document24 pagesInst Intl 1Josito SegoviaNo ratings yet
- Vessel ScheduleDocument30 pagesVessel SchedulecowokperkasaNo ratings yet
- DiagramaEurovan2 8LDocument18 pagesDiagramaEurovan2 8LJonathan De Jesus Astudillo CanoNo ratings yet
- TH 50AS670 EnglishDocument24 pagesTH 50AS670 EnglishDavidNo ratings yet
- Achievement Chart: Contact Center Services NC IiDocument3 pagesAchievement Chart: Contact Center Services NC IiVei Poblete Toledo-Tiongco0% (1)
- Emission Test VW PDFDocument434 pagesEmission Test VW PDFnicolae_popescu_18No ratings yet
- Central LiveDocument1 pageCentral LiveTina WilliamsNo ratings yet
- Tabula Rasa FrontDocument1 pageTabula Rasa FrontsimpsontabularasaNo ratings yet
- D3E802FEE69-TT 24-08-01 All Models With 1 8T Engine - Pressure Loss Fault Code P1297Document4 pagesD3E802FEE69-TT 24-08-01 All Models With 1 8T Engine - Pressure Loss Fault Code P1297Ondřej PolákNo ratings yet
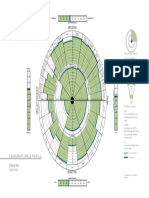
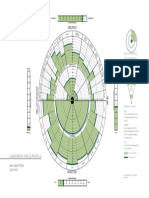
- Leadership Circle ReportDocument1 pageLeadership Circle ReportTyler WoodwardNo ratings yet
- Lampiran Contoh Sediaan KhususDocument36 pagesLampiran Contoh Sediaan Khusus9014salsabila bilaNo ratings yet
- Living Things in Coral Reefs: Inquiry ActivityDocument2 pagesLiving Things in Coral Reefs: Inquiry ActivityDiyanira CastilloNo ratings yet
- Healthy PlateDocument4 pagesHealthy PlateJessica ArvizuNo ratings yet
- In Bed with the Word: Reading, Spirituality, and Cultural PoliticsFrom EverandIn Bed with the Word: Reading, Spirituality, and Cultural PoliticsNo ratings yet
- A History of Medical Device Regulation & Oversight in The United States - FDADocument7 pagesA History of Medical Device Regulation & Oversight in The United States - FDAHector Tinoco GarciaNo ratings yet
- Applied Biopharmacy Exercises by MteDocument19 pagesApplied Biopharmacy Exercises by MteMINANI TheobaldNo ratings yet
- Diesel - Ultra Low Sulphur MSDS PDFDocument3 pagesDiesel - Ultra Low Sulphur MSDS PDFMansyur NasutionNo ratings yet
- Taislim Shake - : Clinically Proven, Tastes Delicious!Document5 pagesTaislim Shake - : Clinically Proven, Tastes Delicious!rhonda_robinson63No ratings yet
- Lesson 4 - Psychological Perspective of The SelfDocument31 pagesLesson 4 - Psychological Perspective of The Selfsusanna rose labastillaNo ratings yet
- Basic Life Suppor T: Monalyn B. La-Ao, RN Keverne Colas, RNDocument51 pagesBasic Life Suppor T: Monalyn B. La-Ao, RN Keverne Colas, RNAudi Kyle SaydovenNo ratings yet
- Marketing-Plan-Ken Andrei L.Document4 pagesMarketing-Plan-Ken Andrei L.Kyle LapuzNo ratings yet
- Stage 8 - Chapter 3 WorksheetsDocument3 pagesStage 8 - Chapter 3 WorksheetsMoath AlsaidNo ratings yet
- MSDS, Nitric-Methanol Nital Etch SolutionDocument4 pagesMSDS, Nitric-Methanol Nital Etch SolutionSeleccion Tecnico IndustrialNo ratings yet
- Obg Unit - 4Document55 pagesObg Unit - 4Preeti ChouhanNo ratings yet
- "I'm So Glad He Waited.": Case StudyDocument3 pages"I'm So Glad He Waited.": Case StudyJermaine Randeeh DelfinNo ratings yet
- Mental Health and WellnessDocument31 pagesMental Health and WellnessLynn RamirezNo ratings yet
- 3i Mixed StudyDocument74 pages3i Mixed StudyJustin Jade AlmerezNo ratings yet
- The Truth About Cocaine and CrackDocument15 pagesThe Truth About Cocaine and Crackapi-616433899No ratings yet
- CH 4 HRM Job Analysis and The Talent Management ProcessDocument26 pagesCH 4 HRM Job Analysis and The Talent Management ProcessOMAR SAMIRNo ratings yet
- Career Evaluation - Neonatal NurseDocument5 pagesCareer Evaluation - Neonatal Nurseapi-533958917No ratings yet
- Base Line Reform Updated MahideremariamDocument2 pagesBase Line Reform Updated MahideremariamDebrie YalewNo ratings yet
- Principles of Fish NutritionDocument21 pagesPrinciples of Fish NutritionAndi Keyen50% (2)
- Vivo 65 Users Manual: Doc. 006088 En-US U-1bDocument228 pagesVivo 65 Users Manual: Doc. 006088 En-US U-1bNandhini SivakumarNo ratings yet
- Creative Writing Vs Technical WritingDocument23 pagesCreative Writing Vs Technical WritingJOY MARIE DOMINGO - SALACUPNo ratings yet
- Health EquityDocument3 pagesHealth EquityExanan TedNo ratings yet
- DLL P.E. Q3 Week 1&2Document3 pagesDLL P.E. Q3 Week 1&2Vernadette HidalgoNo ratings yet
- Concierge Services Training ResedaDocument54 pagesConcierge Services Training ResedaRafiq AhmedNo ratings yet
- Eis35-Safety in Electrical Testing Servicing and Repair of Domestic AppliancesDocument3 pagesEis35-Safety in Electrical Testing Servicing and Repair of Domestic AppliancesYassin SajidNo ratings yet