Download as docx, pdf, or txt
You might also like
- Fast Facts: Clinical Trials in Oncology: The fundamentals of design, conduct and interpretationFrom EverandFast Facts: Clinical Trials in Oncology: The fundamentals of design, conduct and interpretationNo ratings yet
- Routine Blood Results Explained 3/e: A guide for Nurses & Allied Health ProfessionalsFrom EverandRoutine Blood Results Explained 3/e: A guide for Nurses & Allied Health ProfessionalsRating: 3 out of 5 stars3/5 (2)
- Apert Syndrome - Sultan BaroamaimDocument37 pagesApert Syndrome - Sultan BaroamaimsultanNo ratings yet
- Jover Reflection PaperDocument2 pagesJover Reflection PaperGwen Myles JoverNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : A Review of The Clinical ManagementDocument11 pagesChronic Obstructive Pulmonary Disease (COPD) : A Review of The Clinical ManagementAlejandro Kanito Alvarez SNo ratings yet
- Authors: Section Editors: Deputy EditorDocument20 pagesAuthors: Section Editors: Deputy EditorSajal SahaNo ratings yet
- Serum Surfactant Protein D Is Steroid Sensitive and Associated With Exacerbations of COPDDocument8 pagesSerum Surfactant Protein D Is Steroid Sensitive and Associated With Exacerbations of COPDPatrick RamosNo ratings yet
- COPD GOLD Guidelines 2012Document67 pagesCOPD GOLD Guidelines 2012Andreas IoannouNo ratings yet
- Key Learning Points - GOLD COPD 2020 Report - Key Learning Points - Guidelines in PracticeDocument12 pagesKey Learning Points - GOLD COPD 2020 Report - Key Learning Points - Guidelines in PracticeHJ GNo ratings yet
- Stable COPD - Initial Pharmacologic Management - UpToDateDocument32 pagesStable COPD - Initial Pharmacologic Management - UpToDateLiz CampoverdeNo ratings yet
- Copd Exacerbations: Management and Hospital Discharge: ReviewDocument6 pagesCopd Exacerbations: Management and Hospital Discharge: ReviewChristine BelindaNo ratings yet
- Acute Asthma Exacerbations: Phenotypes and Management: Charles B. Cairns, MD TDocument10 pagesAcute Asthma Exacerbations: Phenotypes and Management: Charles B. Cairns, MD TKaren Aguilar PalominoNo ratings yet
- Cap PhilippinesDocument13 pagesCap PhilippinesRaine CentinoNo ratings yet
- Neumonía Grave Del Adulto Adquirida en La Comunidad: Severe Community-Acquired Pneumonia in AdultsDocument6 pagesNeumonía Grave Del Adulto Adquirida en La Comunidad: Severe Community-Acquired Pneumonia in AdultsGaby TreCh ArroyoNo ratings yet
- Rutherford JVS 2000 Venous Severity Scoring AdjunctDocument6 pagesRutherford JVS 2000 Venous Severity Scoring AdjunctMilaNo ratings yet
- Relationship Between Extravascular Lung Water and Severity Categories of Acute Respiratory Distress Syndrome by The Berlin DefinitionDocument9 pagesRelationship Between Extravascular Lung Water and Severity Categories of Acute Respiratory Distress Syndrome by The Berlin DefinitionVictor Euclides Briones MoralesNo ratings yet
- 1193.full DHJSHDDocument9 pages1193.full DHJSHDSharly Ayu PuspitaNo ratings yet
- 12 FullDocument12 pages12 FulljuvvalaNo ratings yet
- Artigo Set 2023Document12 pagesArtigo Set 2023Sofia Adão da FonsecaNo ratings yet
- 2023 Canadian Thoracic Society Guideline On Pharmacotherapy in Patients With Stable COPDDocument25 pages2023 Canadian Thoracic Society Guideline On Pharmacotherapy in Patients With Stable COPDgramachandran186No ratings yet
- COPD Exacerbations - Clinical Manifestations and Evaluation - UpToDateDocument20 pagesCOPD Exacerbations - Clinical Manifestations and Evaluation - UpToDateJúlia PompeuNo ratings yet
- Chronic Obstructive Pulmonary Disease: Patient Population: ObjectivesDocument28 pagesChronic Obstructive Pulmonary Disease: Patient Population: Objectivesdoni anandaNo ratings yet
- 2020 REPORT: Global Strategy For The Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseDocument53 pages2020 REPORT: Global Strategy For The Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseManoj GhimireNo ratings yet
- Executive Summary: Supplement ArticleDocument65 pagesExecutive Summary: Supplement ArticleLeo F ForeroNo ratings yet
- Pneumonia Severity, Comorbidity and 1-YearDocument6 pagesPneumonia Severity, Comorbidity and 1-YearGandri Ali Ma'suNo ratings yet
- Applications of Minimally Invasive Cardiac Output Monitors: Review Open AccessDocument9 pagesApplications of Minimally Invasive Cardiac Output Monitors: Review Open AccessGilbertLiemNo ratings yet
- FAQs About The GOLD 2011 Assessment Proposal of COPD - A Comparative Analysis of Four Different CohortsDocument11 pagesFAQs About The GOLD 2011 Assessment Proposal of COPD - A Comparative Analysis of Four Different CohortsDejan ŽujovićNo ratings yet
- Classification of Surgical ComplicationsDocument18 pagesClassification of Surgical ComplicationsLourdes de la GándaraNo ratings yet
- ContentServer 13 PDFDocument10 pagesContentServer 13 PDFFerdy LainsamputtyNo ratings yet
- ContentServer 13 PDFDocument10 pagesContentServer 13 PDFFerdy LainsamputtyNo ratings yet
- Predictive Value of Red Blood Cell Distribution Width in ChronicDocument8 pagesPredictive Value of Red Blood Cell Distribution Width in ChronicAndreea MoalesNo ratings yet
- Evaluacion Pulmonar PreoperatoriaDocument15 pagesEvaluacion Pulmonar Preoperatorialuis castillejosNo ratings yet
- Artificial Intelligence Techniques in Chronic Condition Lung DiseaseDocument14 pagesArtificial Intelligence Techniques in Chronic Condition Lung DiseaseNexgen TechnologyNo ratings yet
- Risk Stratification in Lung ResectionDocument9 pagesRisk Stratification in Lung ResectionBarbara Daniela Gonzalez EspinozaNo ratings yet
- Management of PulmonaryDocument6 pagesManagement of Pulmonaryopick128No ratings yet
- A Risk Prediction Model For Heart Failure Hospitalization JuroanlDocument20 pagesA Risk Prediction Model For Heart Failure Hospitalization JuroanljamesboendNo ratings yet
- COPD - Diagnosis and ManagementDocument12 pagesCOPD - Diagnosis and ManagementfallenczarNo ratings yet
- Low Body Mass Index, Airflow Obstruction, and Dyspnoea in A Primary Care COPD Patient PopulationDocument6 pagesLow Body Mass Index, Airflow Obstruction, and Dyspnoea in A Primary Care COPD Patient PopulationArizal AbdullahNo ratings yet
- Methacholine1 21Document21 pagesMethacholine1 21Mihaela Dudau100% (1)
- JCOPDF 2015 0172 BerryDocument13 pagesJCOPDF 2015 0172 BerrydhilaidrisNo ratings yet
- Choque HipovolemicoDocument9 pagesChoque HipovolemicoVictor Hugo VillalpandoNo ratings yet
- 2 General Principles of Research Design and AnalysisDocument6 pages2 General Principles of Research Design and AnalysisMohamed Elprince AdelNo ratings yet
- Be Bold With GOLD - An Update From The Late 2011: Where Do The Staging and Handling Go From Here?Document39 pagesBe Bold With GOLD - An Update From The Late 2011: Where Do The Staging and Handling Go From Here?sintinNo ratings yet
- Relationship of Hyperlipidemia To Comorbidities and Lung Function in COPD: Results of The COSYCONET CohortDocument12 pagesRelationship of Hyperlipidemia To Comorbidities and Lung Function in COPD: Results of The COSYCONET CohortwecytriaNo ratings yet
- BODEXDocument8 pagesBODEXLindsey KaufmanNo ratings yet
- Optimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe EmergencydepartmentDocument17 pagesOptimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe Emergencydepartmentهادي تركي شنبارةNo ratings yet
- Lary24916 PDFDocument8 pagesLary24916 PDFDara SNo ratings yet
- Jurnal ENT 1Document6 pagesJurnal ENT 1Anastasia SaskiaNo ratings yet
- RCCM 202212-2300ocDocument14 pagesRCCM 202212-2300ocLucas PereiraNo ratings yet
- Cancer de Pulmon Up To DateDocument197 pagesCancer de Pulmon Up To DateFernando HuertasNo ratings yet
- Early Diagnosis CopdDocument8 pagesEarly Diagnosis CopdNurusshiami KhairatiNo ratings yet
- C-Reactive Protein, Severity of Pneumonia and Mortality in Elderly, Hospitalised Patients With Community-Acquired PneumoniaDocument5 pagesC-Reactive Protein, Severity of Pneumonia and Mortality in Elderly, Hospitalised Patients With Community-Acquired PneumoniaLoserlikemeNo ratings yet
- Guru Kashi University: (SESSION-2018-2022)Document34 pagesGuru Kashi University: (SESSION-2018-2022)Shambhoo SwarajNo ratings yet
- Ultrasound in Emergency MedicineDocument17 pagesUltrasound in Emergency MedicineDara Daula MumtazaNo ratings yet
- Criterios EULAR-ACR de AR 2010 PDFDocument11 pagesCriterios EULAR-ACR de AR 2010 PDFMORADOMIANo ratings yet
- Diffusing Capacity of Carbon Monoxide in Assessment of COPD: Original ResearchDocument9 pagesDiffusing Capacity of Carbon Monoxide in Assessment of COPD: Original ResearchKlinikdr RIDHANo ratings yet
- Characteristics and Prognosis of COVID-19 in Patients With COPDDocument11 pagesCharacteristics and Prognosis of COVID-19 in Patients With COPDDiego Armando Bolivar SilvaNo ratings yet
- Syok HopovolemikDocument9 pagesSyok HopovolemikWulansariNo ratings yet
- The Importance of Model Structure in The Cost-Effectiveness Analysis of Primary Care Interventions For The Management of HypertensionDocument13 pagesThe Importance of Model Structure in The Cost-Effectiveness Analysis of Primary Care Interventions For The Management of HypertensionElsa Natia RindianaNo ratings yet
- Retired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialDocument9 pagesRetired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialSarah GlennNo ratings yet
- Clinical Cases in Chronic Thromboembolic Pulmonary HypertensionFrom EverandClinical Cases in Chronic Thromboembolic Pulmonary HypertensionWilliam R. AugerNo ratings yet
- Lab Manual Human physiology-IIDocument32 pagesLab Manual Human physiology-IIAKASHDEEP SINGHNo ratings yet
- Experiment 8 Manual General Medicine &paedDocument2 pagesExperiment 8 Manual General Medicine &paedAKASHDEEP SINGHNo ratings yet
- Unit - 3 B. Physiotherapy (Pt201) Subject: Basic of BiomechanicsDocument15 pagesUnit - 3 B. Physiotherapy (Pt201) Subject: Basic of BiomechanicsAKASHDEEP SINGHNo ratings yet
- Unit - 3 Subject: Basic of Biomechanics B. Physiotherapy (Pt201)Document16 pagesUnit - 3 Subject: Basic of Biomechanics B. Physiotherapy (Pt201)AKASHDEEP SINGHNo ratings yet
- University Institute of Applied Health Sciences Physiotherapy DepartmentDocument12 pagesUniversity Institute of Applied Health Sciences Physiotherapy DepartmentAKASHDEEP SINGHNo ratings yet
- NocturiaDocument10 pagesNocturiaKousik AmancharlaNo ratings yet
- Done - EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocolDocument21 pagesDone - EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocolVivencio Pascual JrNo ratings yet
- Define Personal Safety Protocol, Dehydration, Overexertion, Hypo and HyperthermiaDocument1 pageDefine Personal Safety Protocol, Dehydration, Overexertion, Hypo and HyperthermiaReina PeloniaNo ratings yet
- Guyabano - 10,000X Stronger Than Chemo (GOOD FOR Our Health)Document4 pagesGuyabano - 10,000X Stronger Than Chemo (GOOD FOR Our Health)Susie GarridoNo ratings yet
- Soapie 3 - HivDocument3 pagesSoapie 3 - HivMicaela CrisostomoNo ratings yet
- Pharmacologic Management: BleomycinDocument1 pagePharmacologic Management: BleomycinKim ApuradoNo ratings yet
- Qualitative ResearchDocument6 pagesQualitative Researchtoshiro lazarteNo ratings yet
- Ratio - MusculoskeletalDocument28 pagesRatio - MusculoskeletalAccey RamirezNo ratings yet
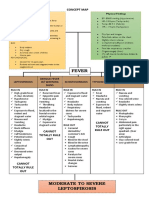
- IM - Leptospirosis Concept MapDocument3 pagesIM - Leptospirosis Concept MapTrisNo ratings yet
- Coccidioidomycosis and Histoplasmosis in Immunocompetent PersonsDocument12 pagesCoccidioidomycosis and Histoplasmosis in Immunocompetent PersonsLeiniker NavarroNo ratings yet
- RLE-MODULE - Traumatic Brain InjuryDocument21 pagesRLE-MODULE - Traumatic Brain InjuryIvy Joy PistolaNo ratings yet
- Chronic Kidney Disease in ChildrenDocument29 pagesChronic Kidney Disease in ChildrenAlvin OmondiNo ratings yet
- Firt Aid 1-9 TranscriptDocument9 pagesFirt Aid 1-9 TranscriptXia AlliaNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- Demodicosis Caused by Demodex Canis and Demodex Cornei in DogsDocument4 pagesDemodicosis Caused by Demodex Canis and Demodex Cornei in DogsAdriansyah RamadhanNo ratings yet
- Divine Intervention Episode 5 Cardio A Physiology1Document18 pagesDivine Intervention Episode 5 Cardio A Physiology1Swisskelly1No ratings yet
- Part4 Evidence1 CozineDocument2 pagesPart4 Evidence1 Cozineapi-286143658No ratings yet
- NCM 107 Intro 1Document34 pagesNCM 107 Intro 1Riegne Chiara Fay AcuzarNo ratings yet
- Medical Exam Revision: Over 58,000 Practice Questions. We'll Help You Pass Your Exam TodayDocument2 pagesMedical Exam Revision: Over 58,000 Practice Questions. We'll Help You Pass Your Exam TodayDocSam048No ratings yet
- Common Sign and Symptoms of Neuro Disease1Document3 pagesCommon Sign and Symptoms of Neuro Disease1gotcurry08No ratings yet
- Lecture BAU LungsDocument131 pagesLecture BAU LungsMohamed HefnyNo ratings yet
- BFO-Review of Pathology AFODocument32 pagesBFO-Review of Pathology AFOnovitaNo ratings yet
- Breast ExaminationDocument4 pagesBreast ExaminationOlamide FeyikemiNo ratings yet
- Psoriasis - WikipediaDocument170 pagesPsoriasis - WikipediaEndhy Wisnu NovindraNo ratings yet
- Occupational Rhinitis Due To Steel Welding Fumes: SS 2014 Wiley Periodicals, IncDocument4 pagesOccupational Rhinitis Due To Steel Welding Fumes: SS 2014 Wiley Periodicals, IncIin Sakinah DewiNo ratings yet
- Total Calcanectomy For The Treatment of Calcaneal OsteomyelitisDocument4 pagesTotal Calcanectomy For The Treatment of Calcaneal OsteomyelitisCleff FlowersNo ratings yet
- Case in Point Monica Teenage PregnancyDocument3 pagesCase in Point Monica Teenage PregnancyElisha Grace Gumal-inNo ratings yet
- Sample Gordon's Functional Health Pattern: Intestinal Obstruction Powerpoint PresentationDocument3 pagesSample Gordon's Functional Health Pattern: Intestinal Obstruction Powerpoint PresentationCharlene Grace ReginoNo ratings yet
- What Is Outpatient Treatment ProgramDocument3 pagesWhat Is Outpatient Treatment ProgramSharon DikirrNo ratings yet