Download as pdf or txt
You might also like
- Schizophrenia NCP and DrugstudyDocument11 pagesSchizophrenia NCP and DrugstudyElle Monge100% (3)
- A Comprehensive Update On Treatment of Dementia-2019Document12 pagesA Comprehensive Update On Treatment of Dementia-2019Juan Paredes100% (1)
- 23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25Document5 pages23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25observacionfray23No ratings yet
- Jurnal NorvascDocument8 pagesJurnal NorvascYoung AjjaNo ratings yet
- JKSHP033 01 05Document12 pagesJKSHP033 01 05dennystefanus03No ratings yet
- Caco 2Document17 pagesCaco 2David RamseyNo ratings yet
- Potkin2002 QTP+ Hal Risp Thiridazine RCTDocument10 pagesPotkin2002 QTP+ Hal Risp Thiridazine RCTIulia CiocotisanNo ratings yet
- Groenendaal Vandemeent2016Document11 pagesGroenendaal Vandemeent2016Soshi DaysNo ratings yet
- Rifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersDocument7 pagesRifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersIulia CiocotisanNo ratings yet
- Efficacy of Oral Lycopene in The Treatment of Oral LeukoplakiaDocument6 pagesEfficacy of Oral Lycopene in The Treatment of Oral Leukoplakia2211801733No ratings yet
- Biof C MaxDocument4 pagesBiof C MaxMARIA FERNANDA VIEIRA RIVERANo ratings yet
- Pharmacogenetics and Antipsychotic Treatment ResponseDocument15 pagesPharmacogenetics and Antipsychotic Treatment Responsebruna.c.moscatelNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- On Metabolism inDocument7 pagesOn Metabolism inAndres Felipe Rojas RodriguezNo ratings yet
- Pharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyDocument9 pagesPharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyCurcubeuAuroraNo ratings yet
- NIH Public Access: Author ManuscriptDocument14 pagesNIH Public Access: Author ManuscriptPutri Septiana PratiwiNo ratings yet
- 1 s2.0 S0753332221008386 MainDocument7 pages1 s2.0 S0753332221008386 MainIsaura MendezNo ratings yet
- The Human Pharmacology of Fluticasone PropionateDocument5 pagesThe Human Pharmacology of Fluticasone PropionatePavel MilovNo ratings yet
- Zhou2008 Vis DujDocument47 pagesZhou2008 Vis DujAnAn BanhGaoNo ratings yet
- Hanefeld Et Al-2017-Diabetes, Obesity and MetabolismDocument8 pagesHanefeld Et Al-2017-Diabetes, Obesity and MetabolismKani RapeeNo ratings yet
- Pharmacogenetics and The Concept of Individualized Medicine: BS ShastryDocument6 pagesPharmacogenetics and The Concept of Individualized Medicine: BS Shastrykunalprabhu148No ratings yet
- Ajp.161.10.1837 2Document11 pagesAjp.161.10.1837 2HKANo ratings yet
- Reduced Postprandial Concentrations of Intact Biologically Active Glucagon-Like Peptide 1 in Type 2 Diabetic PatientsDocument5 pagesReduced Postprandial Concentrations of Intact Biologically Active Glucagon-Like Peptide 1 in Type 2 Diabetic PatientsRoger CNo ratings yet
- 6 Robertson - Clinical Drug Interactions - 0Document44 pages6 Robertson - Clinical Drug Interactions - 0Piyush BandelaNo ratings yet
- Paxil CR: (Paroxetine Hydrochloride) Controlled-Release TabletsDocument42 pagesPaxil CR: (Paroxetine Hydrochloride) Controlled-Release TabletsgammasharkNo ratings yet
- Clinical Efficacy of Mycophenolic Acid in The Treatment of Lupus NephritisDocument7 pagesClinical Efficacy of Mycophenolic Acid in The Treatment of Lupus NephritisRabiatul 'raney' AdawiyahNo ratings yet
- Am J Addict 2009 HamiltonDocument6 pagesAm J Addict 2009 HamiltonalvmdNo ratings yet
- Schiavi 2017Document8 pagesSchiavi 2017Naufal NanditaNo ratings yet
- Alpha-Dihydroergocryptine vs. Pramipexole As Adjunct Symptomatic Treatment of Idiopathic Parkinson'sDocument9 pagesAlpha-Dihydroergocryptine vs. Pramipexole As Adjunct Symptomatic Treatment of Idiopathic Parkinson'sRizka Leonita FahmyNo ratings yet
- Effect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientsDocument10 pagesEffect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientstrianaamaliaNo ratings yet
- Jakobsen2016Document11 pagesJakobsen2016caturNo ratings yet
- 10 1089@cap 2016 0178Document2 pages10 1089@cap 2016 0178Maria Helena Pedraza MNo ratings yet
- Clozapin RisperidonDocument7 pagesClozapin RisperidonAnonymous 2LcGdsRNo ratings yet
- Jurnal Inhibitor Enzim AlfaglukosidaseDocument13 pagesJurnal Inhibitor Enzim AlfaglukosidaseMarisa NurlitaNo ratings yet
- Curcumin LNDocument8 pagesCurcumin LNHend MahranNo ratings yet
- Darwish2012 Qtp+Armodafinil RCTDocument11 pagesDarwish2012 Qtp+Armodafinil RCTIulia CiocotisanNo ratings yet
- 60 - Minocycline Combination Therapy Withfluvoxaminein Moderate-To-Severe Obsessive-Compulsive Disorder, A Placebo-Controlled, Double-Blind, Randomized TrialDocument10 pages60 - Minocycline Combination Therapy Withfluvoxaminein Moderate-To-Severe Obsessive-Compulsive Disorder, A Placebo-Controlled, Double-Blind, Randomized TrialPaula CantalapiedraNo ratings yet
- Pharmacokinetics, Pharmacodynamics, and Safety of Apixaban in Subjects With End-Stage Renal Disease On HemodialysisDocument9 pagesPharmacokinetics, Pharmacodynamics, and Safety of Apixaban in Subjects With End-Stage Renal Disease On HemodialysisAnonymous S8bsuMNo ratings yet
- Commentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisoloneDocument20 pagesCommentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisolonePrisca WicitaNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Dapoxetine Hydrochloride Prescribing InformationDocument17 pagesDapoxetine Hydrochloride Prescribing InformationAdnan TowfiqueNo ratings yet
- Effect of Polymorphisms On The Pharmacokinetics, Pharmacodynamics andDocument32 pagesEffect of Polymorphisms On The Pharmacokinetics, Pharmacodynamics andmijon46No ratings yet
- Jurnal 3Document6 pagesJurnal 3rifahNo ratings yet
- DEPICT 1 - T1D StudyDocument13 pagesDEPICT 1 - T1D StudyGVRNo ratings yet
- Nej Mo A 1412278Document10 pagesNej Mo A 1412278amiralevishNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Reasearch Publication - RJPSDocument4 pagesReasearch Publication - RJPSHamza Muhammad ShethNo ratings yet
- Tirzepatide Versus Semaglutide Once Weekly in Patients With Type 2 DiabetesDocument13 pagesTirzepatide Versus Semaglutide Once Weekly in Patients With Type 2 Diabetesmanish chaudharyNo ratings yet
- Liraglutide Improves Non-Alcoholic Fatty Liver Disease in Diabetic Mice by Modulating in Ammatory Signaling PathwaysDocument10 pagesLiraglutide Improves Non-Alcoholic Fatty Liver Disease in Diabetic Mice by Modulating in Ammatory Signaling PathwaysAndreea Claudia NegrilaNo ratings yet
- Farm A Kogen EtikDocument60 pagesFarm A Kogen Etikrahmad wahyudiNo ratings yet
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Pharmacodynamic Evaluation of Pantoprazole Therapy On Clopidogrel EffectsDocument7 pagesPharmacodynamic Evaluation of Pantoprazole Therapy On Clopidogrel EffectsOk bro I am doneNo ratings yet
- Ghost AuthorDocument13 pagesGhost AuthorjbahalkehNo ratings yet
- Is The Efficacy of Primaquine in Malarial Treatment Affected by The Inhibition of CYP2D6 by Antidepressants?Document5 pagesIs The Efficacy of Primaquine in Malarial Treatment Affected by The Inhibition of CYP2D6 by Antidepressants?ACOME TutoringNo ratings yet
- Mucuna Pruriens in Parkinson's Disease: A Double Blind Clinical and Pharmacological StudyDocument6 pagesMucuna Pruriens in Parkinson's Disease: A Double Blind Clinical and Pharmacological StudygatemNo ratings yet
- Interaction Study Between Digoxin and A Preparation of Hawthorn (Crataegus Oxyacantha)Document6 pagesInteraction Study Between Digoxin and A Preparation of Hawthorn (Crataegus Oxyacantha)veeramaniNo ratings yet
- Sambiloto PDFDocument7 pagesSambiloto PDFMarselina SattuNo ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- 1 s2.0 S0168822714003143 MainDocument7 pages1 s2.0 S0168822714003143 MaindesyNo ratings yet
- Endoxifen A New Treatment Option For Mania A Double Blind Active Controlled Trial Demonstrates The Antimanic Efficacy of EndoxifenDocument8 pagesEndoxifen A New Treatment Option For Mania A Double Blind Active Controlled Trial Demonstrates The Antimanic Efficacy of EndoxifenchintanNo ratings yet
- The Effects of Andrographis Paniculata (Burm.f.) Nees On The Pharmacokinetics and Pharmacodynamics of Midazolam in Healthy VolunteersDocument7 pagesThe Effects of Andrographis Paniculata (Burm.f.) Nees On The Pharmacokinetics and Pharmacodynamics of Midazolam in Healthy VolunteersAdquinta Wulandini PutriNo ratings yet
- Histopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationFrom EverandHistopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationNo ratings yet
- Potkin2002 QTP+ Hal Risp Thiridazine RCTDocument10 pagesPotkin2002 QTP+ Hal Risp Thiridazine RCTIulia CiocotisanNo ratings yet
- Nemoto2012 Apz+ Paroxetina RCTDocument5 pagesNemoto2012 Apz+ Paroxetina RCTIulia CiocotisanNo ratings yet
- Serum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationDocument4 pagesSerum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationIulia CiocotisanNo ratings yet
- Effects of Escitalopram On Plasma Concentrations of Aripiprazole and Its Active Metabolite, Dehydroaripiprazole, in Japanese PatientsDocument5 pagesEffects of Escitalopram On Plasma Concentrations of Aripiprazole and Its Active Metabolite, Dehydroaripiprazole, in Japanese PatientsIulia CiocotisanNo ratings yet
- Rifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersDocument7 pagesRifampin, A Cytochrome P450 3A Inducer, Decreases Plasma Concentrations of Antipsychotic Risperidone in Healthy VolunteersIulia CiocotisanNo ratings yet
- The Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineDocument9 pagesThe Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineIulia CiocotisanNo ratings yet
- Darwish2012 Qtp+Armodafinil RCTDocument11 pagesDarwish2012 Qtp+Armodafinil RCTIulia CiocotisanNo ratings yet
- The Jere Beasley Report, May 2008Document52 pagesThe Jere Beasley Report, May 2008Beasley AllenNo ratings yet
- 175 Anaesthesia and Psychiatric Drugs Part 2 Mood Stabilisers and Antipsychotics PDFDocument6 pages175 Anaesthesia and Psychiatric Drugs Part 2 Mood Stabilisers and Antipsychotics PDFWahyu Permata LisaNo ratings yet
- Bipolar DisorderDocument3 pagesBipolar Disordermuhammad_hanis97No ratings yet
- Psychiatry Dr. Osama Mahmoud PDFDocument59 pagesPsychiatry Dr. Osama Mahmoud PDFRaouf Ra'fat SolimanNo ratings yet
- Template Aging Obat Jan 24Document654 pagesTemplate Aging Obat Jan 24fennyrahmaNo ratings yet
- AntipsychoticsDocument29 pagesAntipsychoticsTyler Lawrence Coye100% (5)
- Stuttering Treatment and Its PharmacologyDocument8 pagesStuttering Treatment and Its Pharmacologybaba ababNo ratings yet
- Psychiatric Emergencies and Nursing ManagementDocument40 pagesPsychiatric Emergencies and Nursing Managementavanthikasathiya29No ratings yet
- UPTODATE Management of Neuropsychiatric Symptoms of Dementia - UpToDateDocument32 pagesUPTODATE Management of Neuropsychiatric Symptoms of Dementia - UpToDateQwerty QwertyNo ratings yet
- Clozapine For Schizophrenia - Life-Threatening or Life-Saving TreatmentDocument8 pagesClozapine For Schizophrenia - Life-Threatening or Life-Saving TreatmentAnonymous teh3Gj5TabNo ratings yet
- Zyprexa: Olanzapine TabletsDocument32 pagesZyprexa: Olanzapine TabletsnalgatoreNo ratings yet
- Advisory On Reiteration of Ao 2021 0012 Implementing Guidelines On The Medicine Access Program For Health 2Document7 pagesAdvisory On Reiteration of Ao 2021 0012 Implementing Guidelines On The Medicine Access Program For Health 2ncd.bulacanNo ratings yet
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- Why The NHS Must ChangeDocument2 pagesWhy The NHS Must ChangeMark HayesNo ratings yet
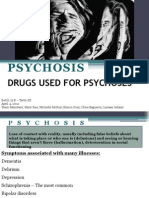
- Psychosis: Drugs Used For PsychosesDocument53 pagesPsychosis: Drugs Used For PsychosesLarissa SabsayNo ratings yet
- The Successful ConcurrentDocument5 pagesThe Successful ConcurrentShevamykolayovychshevchenko MilaniztyonlymilanelloNo ratings yet
- NLE Exam Drill 4 (Q Only 100)Document13 pagesNLE Exam Drill 4 (Q Only 100)Epaphras Joel Militar0% (1)
- Psychiatric Nursing Notes: Psych MedsDocument59 pagesPsychiatric Nursing Notes: Psych Medssurviving nursing schoolNo ratings yet
- Antipsychotic: Antipsychotics, Also Known As NeurolepticsDocument28 pagesAntipsychotic: Antipsychotics, Also Known As NeurolepticsJussel Vazquez MarquezNo ratings yet
- NDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813Document8 pagesNDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813twahyuningsih_16No ratings yet
- Bipolar Disorder PDFDocument108 pagesBipolar Disorder PDFMaica LectanaNo ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentMuhammad Haris Khan KhattakNo ratings yet
- Update On Therapeutics: Shehan Williams and Thilini RajapakseDocument3 pagesUpdate On Therapeutics: Shehan Williams and Thilini RajapakseAnjula KumarasingheNo ratings yet
- Drug StudyDocument4 pagesDrug StudyJenny YenNo ratings yet
- About This List DosingDocument15 pagesAbout This List DosingAla AbushehabNo ratings yet
- Drug StudyDocument3 pagesDrug StudyHarland EstebanNo ratings yet
- Quick Reference Guide April 2019 PDFDocument2 pagesQuick Reference Guide April 2019 PDFAaron ShokarNo ratings yet