
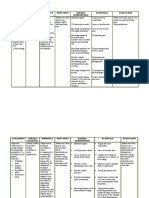
Nursing Care Plan
Nursing Care Plan
You might also like
- NCP Pain HypertensionDocument3 pagesNCP Pain HypertensionEzron Kendrick Duran50% (2)
- CARAGAN, Chantal Herpes Zoster Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Short Term: Independent: Short TermDocument4 pagesCARAGAN, Chantal Herpes Zoster Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Short Term: Independent: Short TermChantal Caragan100% (2)
- Escoton, Kate Angel P (NCP)Document4 pagesEscoton, Kate Angel P (NCP)Kate EscotonNo ratings yet
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- NCP (Acute Pain)Document3 pagesNCP (Acute Pain)Jared Niles SantosNo ratings yet
- NCP PainDocument1 pageNCP PaindwightciderNo ratings yet
- NCP Patient LDocument3 pagesNCP Patient LKyra Lalaine Angub CervantesNo ratings yet
- CAREPLAN For Sickle Cell AnemiaDocument9 pagesCAREPLAN For Sickle Cell AnemiaCecil MonteroNo ratings yet
- Principles of Pathophysiology - Bullock, ShaneDocument2 pagesPrinciples of Pathophysiology - Bullock, ShaneMel Izhra N. MargateNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyDocument2 pagesAssessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyMaria Jessica DumdumNo ratings yet
- Bukidnon State University College of NursingDocument5 pagesBukidnon State University College of NursingAIZA MAE BANGGAY100% (1)
- Nursing Care Plan: Western Mindanao State University College of NursingDocument11 pagesNursing Care Plan: Western Mindanao State University College of NursingPatricia VasquezNo ratings yet
- Nursing-Care-Plan-J P VDocument8 pagesNursing-Care-Plan-J P VMa. Ferimi Gleam BajadoNo ratings yet
- Typhoid Fever NCPDocument46 pagesTyphoid Fever NCPLyra Lustre RN67% (3)
- NCP Group 4Document4 pagesNCP Group 4Chin Villanueva UlamNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- NCP Abdominal PainDocument5 pagesNCP Abdominal PainKingJayson Pacman06No ratings yet
- Nursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisDocument4 pagesNursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisGaming BoyNo ratings yet
- GAYO C. Revised NCPDocument7 pagesGAYO C. Revised NCPCarl LacambraNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanDump AccountNo ratings yet
- Acute PainDocument5 pagesAcute PainEricka MunsayacNo ratings yet
- Nursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument7 pagesNursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationHanz Abbigail Roco100% (1)
- NCPDocument3 pagesNCPHarland EstebanNo ratings yet
- NCP 2Document7 pagesNCP 2Janina Kirsten DevezaNo ratings yet
- Actual NCPDocument10 pagesActual NCPRouie Björn ABrianNo ratings yet
- Colorectal Cancer NCPDocument6 pagesColorectal Cancer NCPAudrie Allyson GabalesNo ratings yet
- Carpal Tunnel PresentationDocument27 pagesCarpal Tunnel PresentationsboNo ratings yet
- S: "Masakit Ang Ulo at Tiyan Niya" As Verbalized byDocument2 pagesS: "Masakit Ang Ulo at Tiyan Niya" As Verbalized bydenise-iceNo ratings yet
- Actual NCP Pt.Document2 pagesActual NCP Pt.Kate WeyganNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Question 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionDocument12 pagesQuestion 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionJoie JoieNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- NCP Montano 2Document3 pagesNCP Montano 2Eduard GarchitorenaNo ratings yet
- NCP For Case Presentation (Acute Pain, Episiotomy)Document3 pagesNCP For Case Presentation (Acute Pain, Episiotomy)Jenny Ajoc100% (2)
- Acute PainDocument3 pagesAcute PainbrianajoyNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- Gouty NCPDocument9 pagesGouty NCPKrishelle Kate PannigNo ratings yet
- نسخة vaginal delieveryDocument4 pagesنسخة vaginal delieveryرهف الرفاعيNo ratings yet
- BERNARDO - Dash 6 (NCP)Document1 pageBERNARDO - Dash 6 (NCP)Aurea Marie PinedaNo ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2gaeLtorvzNo ratings yet
- 5 Hamad Core Comeptencies FinalDocument2 pages5 Hamad Core Comeptencies FinalvhonNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyDocument2 pagesAssessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyMaria Jessica DumdumNo ratings yet
- Nursing Process Care Plan Alteration in Comfort/ PainDocument2 pagesNursing Process Care Plan Alteration in Comfort/ Paintspears8278% (9)
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Nursing Care Plan For Incarcerated Inguinal Hernia RightDocument2 pagesNursing Care Plan For Incarcerated Inguinal Hernia RightTrisha Lapid MatulaNo ratings yet
- NCPDocument4 pagesNCPfairwoods90% (10)
- AssessmentDocument9 pagesAssessmentTawny Antonete LandinginNo ratings yet
- Hospital Duty ReqsDocument16 pagesHospital Duty ReqsRey Jean GarciaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (1)
- NCP Villahermosa CTSDocument6 pagesNCP Villahermosa CTSJv Jore VillahermosaNo ratings yet
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Document10 pagesNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- Problem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020Document2 pagesProblem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020florenzoNo ratings yet
- Problem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METDocument2 pagesProblem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METGwyneth Christine TanNo ratings yet
- Page 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Document3 pagesPage 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Senyorita KHayeNo ratings yet
- NCP Group 4Document4 pagesNCP Group 4Jay VillasotoNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- Ns3a NCP and Drug StudyDocument9 pagesNs3a NCP and Drug StudyANNAMA3 SELMERNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- Drug StudyDocument17 pagesDrug StudyJam CorrosNo ratings yet
- Drug TabulationDocument22 pagesDrug TabulationJam CorrosNo ratings yet
- Skeletal and Skin TractionDocument16 pagesSkeletal and Skin TractionJam Corros100% (2)
- THYROIDECTOMYDocument30 pagesTHYROIDECTOMYJam CorrosNo ratings yet
- SuturesDocument18 pagesSuturesJam CorrosNo ratings yet
- Amputation: Juvie Lie F. Ferren, SNDocument15 pagesAmputation: Juvie Lie F. Ferren, SNJam CorrosNo ratings yet
- AppealDocument3 pagesAppealJam CorrosNo ratings yet
- Final Rerum NovarumDocument2 pagesFinal Rerum NovarumJam CorrosNo ratings yet
- Maribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNDocument46 pagesMaribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNJam CorrosNo ratings yet
- Pleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Document64 pagesPleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Jam CorrosNo ratings yet
- CaneDocument2 pagesCaneJam CorrosNo ratings yet
- St. Anthony College of Roxas CityDocument3 pagesSt. Anthony College of Roxas CityJam CorrosNo ratings yet
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- Assistive Devices: Jam Valles Corros, SNDocument35 pagesAssistive Devices: Jam Valles Corros, SNJam Corros100% (1)
- Bernadeth Lee Chest Trauma Blunt Trauma Penetrating Trauma Pneumothorax Cardiac Tamponade Subcutaneous Emphysema Chest TraumaDocument9 pagesBernadeth Lee Chest Trauma Blunt Trauma Penetrating Trauma Pneumothorax Cardiac Tamponade Subcutaneous Emphysema Chest TraumaJam CorrosNo ratings yet
- NCP & DRUG STUDY Pedia PneumoniaDocument5 pagesNCP & DRUG STUDY Pedia PneumoniaJam CorrosNo ratings yet
- APPENDECTOMYDocument17 pagesAPPENDECTOMYJam CorrosNo ratings yet
- St. Anthony College of Roxas CityDocument5 pagesSt. Anthony College of Roxas CityJam CorrosNo ratings yet
- NuclearMedicineMedicalStudents LecturesDocument197 pagesNuclearMedicineMedicalStudents LecturesCosmin ConstantinNo ratings yet
- 536 - Day Care ListDocument6 pages536 - Day Care ListNikhilNo ratings yet
- Benchmark Lab Manual For Medical Students 7-06Document46 pagesBenchmark Lab Manual For Medical Students 7-06jkasfdjkNo ratings yet
- Genital ProlapseDocument40 pagesGenital ProlapseDIPENDRA KUMAR KUSHAWAHANo ratings yet
- Venipuncture: Syringe Draw Procedure Principles of Medical Technology Practice 2 Laboratory Act. 6Document17 pagesVenipuncture: Syringe Draw Procedure Principles of Medical Technology Practice 2 Laboratory Act. 6ALEXANDRA MARIE BUNQUINNo ratings yet
- Original Article Surgical Management of Acne InversaDocument5 pagesOriginal Article Surgical Management of Acne InversaNomi AkramNo ratings yet
- NEHA PerioDocument1 pageNEHA Periorupak biswasNo ratings yet
- Negen Born 2018Document10 pagesNegen Born 2018salyouhaNo ratings yet
- Referat Presbiopia FFPDocument19 pagesReferat Presbiopia FFPPeak a MiaowNo ratings yet
- PaedsDocument17 pagesPaedsmierahNo ratings yet
- Tendinitis Calcificante en Hombro. Comparación Ondas Choque Vs AgujaDocument7 pagesTendinitis Calcificante en Hombro. Comparación Ondas Choque Vs AgujaAJ CésarNo ratings yet
- Goldenhar Syndrome: Current Perspectives: Katarzyna Bogusiak, Aleksandra Puch, Piotr ArkuszewskiDocument11 pagesGoldenhar Syndrome: Current Perspectives: Katarzyna Bogusiak, Aleksandra Puch, Piotr ArkuszewskiDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- 3 2 1 Code It 5th Edition Green Test Bank DownloadDocument8 pages3 2 1 Code It 5th Edition Green Test Bank DownloadelizabethNo ratings yet
- General Surgery NuggetsDocument12 pagesGeneral Surgery Nuggetsamna_badar1No ratings yet
- Courseintheward EBBDocument8 pagesCourseintheward EBBCogie SalvadorNo ratings yet
- Anal GlandsDocument7 pagesAnal GlandsSuraj_Subedi100% (2)
- Guided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexDocument16 pagesGuided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexLalaNo ratings yet
- TECH 19 - UBC ACC Metacam SOP (2016) PDFDocument2 pagesTECH 19 - UBC ACC Metacam SOP (2016) PDFVicentiu PredescuNo ratings yet
- Management of The Colonic Volvulus in 2016Document10 pagesManagement of The Colonic Volvulus in 2016alexandraNo ratings yet
- Inguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)Document18 pagesInguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)GAURAV0% (1)
- Incidence and Clinical Significance of Zygomaticomaxillary Complex Fracture Involving The Temporomandibular Joint With Emphasis On TrismusDocument5 pagesIncidence and Clinical Significance of Zygomaticomaxillary Complex Fracture Involving The Temporomandibular Joint With Emphasis On TrismusBasofi Ashari MappakayaNo ratings yet
- ArticuloDocument10 pagesArticuloluis danielNo ratings yet
- Book List GNM 2nd YearDocument1 pageBook List GNM 2nd YearIndira DebnathNo ratings yet
- ERCP CurriculumDocument17 pagesERCP CurriculumEvangelosNo ratings yet
- Blue Book 2019 2Document173 pagesBlue Book 2019 2MNo ratings yet
- Estenosis AnalDocument5 pagesEstenosis AnalluissparkNo ratings yet
- Chest Tube Critical SeminarDocument7 pagesChest Tube Critical SeminarRuqia Al-matrouk100% (2)
- Prasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyDocument4 pagesPrasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyMinh NguyenNo ratings yet
- Revision LCCK Instrumentation Surgical TechniqueDocument112 pagesRevision LCCK Instrumentation Surgical TechniqueJehannah Dayanara HayudiniNo ratings yet
- 3 Phases of Operating Room Technique: Preoperative Phase Intraoperative Phase Post Operative PhaseDocument76 pages3 Phases of Operating Room Technique: Preoperative Phase Intraoperative Phase Post Operative Phasejamaica cabriga100% (1)










































































































Download as docx, pdf, or txt
You might also like
- NCP Pain HypertensionDocument3 pagesNCP Pain HypertensionEzron Kendrick Duran50% (2)
- CARAGAN, Chantal Herpes Zoster Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Short Term: Independent: Short TermDocument4 pagesCARAGAN, Chantal Herpes Zoster Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Short Term: Independent: Short TermChantal Caragan100% (2)
- Escoton, Kate Angel P (NCP)Document4 pagesEscoton, Kate Angel P (NCP)Kate EscotonNo ratings yet
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- NCP (Acute Pain)Document3 pagesNCP (Acute Pain)Jared Niles SantosNo ratings yet
- NCP PainDocument1 pageNCP PaindwightciderNo ratings yet
- NCP Patient LDocument3 pagesNCP Patient LKyra Lalaine Angub CervantesNo ratings yet
- CAREPLAN For Sickle Cell AnemiaDocument9 pagesCAREPLAN For Sickle Cell AnemiaCecil MonteroNo ratings yet
- Principles of Pathophysiology - Bullock, ShaneDocument2 pagesPrinciples of Pathophysiology - Bullock, ShaneMel Izhra N. MargateNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyDocument2 pagesAssessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyMaria Jessica DumdumNo ratings yet
- Bukidnon State University College of NursingDocument5 pagesBukidnon State University College of NursingAIZA MAE BANGGAY100% (1)
- Nursing Care Plan: Western Mindanao State University College of NursingDocument11 pagesNursing Care Plan: Western Mindanao State University College of NursingPatricia VasquezNo ratings yet
- Nursing-Care-Plan-J P VDocument8 pagesNursing-Care-Plan-J P VMa. Ferimi Gleam BajadoNo ratings yet
- Typhoid Fever NCPDocument46 pagesTyphoid Fever NCPLyra Lustre RN67% (3)
- NCP Group 4Document4 pagesNCP Group 4Chin Villanueva UlamNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- NCP Abdominal PainDocument5 pagesNCP Abdominal PainKingJayson Pacman06No ratings yet
- Nursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisDocument4 pagesNursing Care Plan: Patient Name: James Japitana AGE:28 Sex:Male DiagnosisGaming BoyNo ratings yet
- GAYO C. Revised NCPDocument7 pagesGAYO C. Revised NCPCarl LacambraNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanDump AccountNo ratings yet
- Acute PainDocument5 pagesAcute PainEricka MunsayacNo ratings yet
- Nursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument7 pagesNursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationHanz Abbigail Roco100% (1)
- NCPDocument3 pagesNCPHarland EstebanNo ratings yet
- NCP 2Document7 pagesNCP 2Janina Kirsten DevezaNo ratings yet
- Actual NCPDocument10 pagesActual NCPRouie Björn ABrianNo ratings yet
- Colorectal Cancer NCPDocument6 pagesColorectal Cancer NCPAudrie Allyson GabalesNo ratings yet
- Carpal Tunnel PresentationDocument27 pagesCarpal Tunnel PresentationsboNo ratings yet
- S: "Masakit Ang Ulo at Tiyan Niya" As Verbalized byDocument2 pagesS: "Masakit Ang Ulo at Tiyan Niya" As Verbalized bydenise-iceNo ratings yet
- Actual NCP Pt.Document2 pagesActual NCP Pt.Kate WeyganNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Question 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionDocument12 pagesQuestion 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionJoie JoieNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- NCP Montano 2Document3 pagesNCP Montano 2Eduard GarchitorenaNo ratings yet
- NCP For Case Presentation (Acute Pain, Episiotomy)Document3 pagesNCP For Case Presentation (Acute Pain, Episiotomy)Jenny Ajoc100% (2)
- Acute PainDocument3 pagesAcute PainbrianajoyNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- Gouty NCPDocument9 pagesGouty NCPKrishelle Kate PannigNo ratings yet
- نسخة vaginal delieveryDocument4 pagesنسخة vaginal delieveryرهف الرفاعيNo ratings yet
- BERNARDO - Dash 6 (NCP)Document1 pageBERNARDO - Dash 6 (NCP)Aurea Marie PinedaNo ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2gaeLtorvzNo ratings yet
- 5 Hamad Core Comeptencies FinalDocument2 pages5 Hamad Core Comeptencies FinalvhonNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyDocument2 pagesAssessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyMaria Jessica DumdumNo ratings yet
- Nursing Process Care Plan Alteration in Comfort/ PainDocument2 pagesNursing Process Care Plan Alteration in Comfort/ Paintspears8278% (9)
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Nursing Care Plan For Incarcerated Inguinal Hernia RightDocument2 pagesNursing Care Plan For Incarcerated Inguinal Hernia RightTrisha Lapid MatulaNo ratings yet
- NCPDocument4 pagesNCPfairwoods90% (10)
- AssessmentDocument9 pagesAssessmentTawny Antonete LandinginNo ratings yet
- Hospital Duty ReqsDocument16 pagesHospital Duty ReqsRey Jean GarciaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (1)
- NCP Villahermosa CTSDocument6 pagesNCP Villahermosa CTSJv Jore VillahermosaNo ratings yet
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Document10 pagesNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- Problem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020Document2 pagesProblem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020florenzoNo ratings yet
- Problem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METDocument2 pagesProblem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METGwyneth Christine TanNo ratings yet
- Page 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Document3 pagesPage 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Senyorita KHayeNo ratings yet
- NCP Group 4Document4 pagesNCP Group 4Jay VillasotoNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- Ns3a NCP and Drug StudyDocument9 pagesNs3a NCP and Drug StudyANNAMA3 SELMERNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- Drug StudyDocument17 pagesDrug StudyJam CorrosNo ratings yet
- Drug TabulationDocument22 pagesDrug TabulationJam CorrosNo ratings yet
- Skeletal and Skin TractionDocument16 pagesSkeletal and Skin TractionJam Corros100% (2)
- THYROIDECTOMYDocument30 pagesTHYROIDECTOMYJam CorrosNo ratings yet
- SuturesDocument18 pagesSuturesJam CorrosNo ratings yet
- Amputation: Juvie Lie F. Ferren, SNDocument15 pagesAmputation: Juvie Lie F. Ferren, SNJam CorrosNo ratings yet
- AppealDocument3 pagesAppealJam CorrosNo ratings yet
- Final Rerum NovarumDocument2 pagesFinal Rerum NovarumJam CorrosNo ratings yet
- Maribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNDocument46 pagesMaribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNJam CorrosNo ratings yet
- Pleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Document64 pagesPleurisy, Pleural Effusion, Emphysema, Pulmonary Edema and ARS (CORROS)Jam CorrosNo ratings yet
- CaneDocument2 pagesCaneJam CorrosNo ratings yet
- St. Anthony College of Roxas CityDocument3 pagesSt. Anthony College of Roxas CityJam CorrosNo ratings yet
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- Assistive Devices: Jam Valles Corros, SNDocument35 pagesAssistive Devices: Jam Valles Corros, SNJam Corros100% (1)
- Bernadeth Lee Chest Trauma Blunt Trauma Penetrating Trauma Pneumothorax Cardiac Tamponade Subcutaneous Emphysema Chest TraumaDocument9 pagesBernadeth Lee Chest Trauma Blunt Trauma Penetrating Trauma Pneumothorax Cardiac Tamponade Subcutaneous Emphysema Chest TraumaJam CorrosNo ratings yet
- NCP & DRUG STUDY Pedia PneumoniaDocument5 pagesNCP & DRUG STUDY Pedia PneumoniaJam CorrosNo ratings yet
- APPENDECTOMYDocument17 pagesAPPENDECTOMYJam CorrosNo ratings yet
- St. Anthony College of Roxas CityDocument5 pagesSt. Anthony College of Roxas CityJam CorrosNo ratings yet
- NuclearMedicineMedicalStudents LecturesDocument197 pagesNuclearMedicineMedicalStudents LecturesCosmin ConstantinNo ratings yet
- 536 - Day Care ListDocument6 pages536 - Day Care ListNikhilNo ratings yet
- Benchmark Lab Manual For Medical Students 7-06Document46 pagesBenchmark Lab Manual For Medical Students 7-06jkasfdjkNo ratings yet
- Genital ProlapseDocument40 pagesGenital ProlapseDIPENDRA KUMAR KUSHAWAHANo ratings yet
- Venipuncture: Syringe Draw Procedure Principles of Medical Technology Practice 2 Laboratory Act. 6Document17 pagesVenipuncture: Syringe Draw Procedure Principles of Medical Technology Practice 2 Laboratory Act. 6ALEXANDRA MARIE BUNQUINNo ratings yet
- Original Article Surgical Management of Acne InversaDocument5 pagesOriginal Article Surgical Management of Acne InversaNomi AkramNo ratings yet
- NEHA PerioDocument1 pageNEHA Periorupak biswasNo ratings yet
- Negen Born 2018Document10 pagesNegen Born 2018salyouhaNo ratings yet
- Referat Presbiopia FFPDocument19 pagesReferat Presbiopia FFPPeak a MiaowNo ratings yet
- PaedsDocument17 pagesPaedsmierahNo ratings yet
- Tendinitis Calcificante en Hombro. Comparación Ondas Choque Vs AgujaDocument7 pagesTendinitis Calcificante en Hombro. Comparación Ondas Choque Vs AgujaAJ CésarNo ratings yet
- Goldenhar Syndrome: Current Perspectives: Katarzyna Bogusiak, Aleksandra Puch, Piotr ArkuszewskiDocument11 pagesGoldenhar Syndrome: Current Perspectives: Katarzyna Bogusiak, Aleksandra Puch, Piotr ArkuszewskiDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- 3 2 1 Code It 5th Edition Green Test Bank DownloadDocument8 pages3 2 1 Code It 5th Edition Green Test Bank DownloadelizabethNo ratings yet
- General Surgery NuggetsDocument12 pagesGeneral Surgery Nuggetsamna_badar1No ratings yet
- Courseintheward EBBDocument8 pagesCourseintheward EBBCogie SalvadorNo ratings yet
- Anal GlandsDocument7 pagesAnal GlandsSuraj_Subedi100% (2)
- Guided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexDocument16 pagesGuided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexLalaNo ratings yet
- TECH 19 - UBC ACC Metacam SOP (2016) PDFDocument2 pagesTECH 19 - UBC ACC Metacam SOP (2016) PDFVicentiu PredescuNo ratings yet
- Management of The Colonic Volvulus in 2016Document10 pagesManagement of The Colonic Volvulus in 2016alexandraNo ratings yet
- Inguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)Document18 pagesInguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)GAURAV0% (1)
- Incidence and Clinical Significance of Zygomaticomaxillary Complex Fracture Involving The Temporomandibular Joint With Emphasis On TrismusDocument5 pagesIncidence and Clinical Significance of Zygomaticomaxillary Complex Fracture Involving The Temporomandibular Joint With Emphasis On TrismusBasofi Ashari MappakayaNo ratings yet
- ArticuloDocument10 pagesArticuloluis danielNo ratings yet
- Book List GNM 2nd YearDocument1 pageBook List GNM 2nd YearIndira DebnathNo ratings yet
- ERCP CurriculumDocument17 pagesERCP CurriculumEvangelosNo ratings yet
- Blue Book 2019 2Document173 pagesBlue Book 2019 2MNo ratings yet
- Estenosis AnalDocument5 pagesEstenosis AnalluissparkNo ratings yet
- Chest Tube Critical SeminarDocument7 pagesChest Tube Critical SeminarRuqia Al-matrouk100% (2)
- Prasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyDocument4 pagesPrasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyMinh NguyenNo ratings yet
- Revision LCCK Instrumentation Surgical TechniqueDocument112 pagesRevision LCCK Instrumentation Surgical TechniqueJehannah Dayanara HayudiniNo ratings yet
- 3 Phases of Operating Room Technique: Preoperative Phase Intraoperative Phase Post Operative PhaseDocument76 pages3 Phases of Operating Room Technique: Preoperative Phase Intraoperative Phase Post Operative Phasejamaica cabriga100% (1)