Download as pdf or txt
You might also like
- Invention and Evolution Design in Nature and EngineeringDocument387 pagesInvention and Evolution Design in Nature and Engineeringphucborso1100% (1)
- Calcium, Phosphate and MagnesiumDocument46 pagesCalcium, Phosphate and Magnesiumkiedd_04100% (3)
- Calcium and PhosphateDocument49 pagesCalcium and Phosphatehaidernadhem57No ratings yet
- What Is The Most Abundant Mineral in The Body?Document33 pagesWhat Is The Most Abundant Mineral in The Body?Niño Española BenedictoNo ratings yet
- Calcium and PhosphateDocument35 pagesCalcium and PhosphateSULEIMAN OMARNo ratings yet
- Endo Lect - ParathyroidDocument25 pagesEndo Lect - ParathyroiddoctorrfarrukhNo ratings yet
- Calcium and Phosphate Metabolism 1Document14 pagesCalcium and Phosphate Metabolism 1samueltoluwabori360No ratings yet
- Parathyroid: Calcium and Vitamin DDocument135 pagesParathyroid: Calcium and Vitamin DPhysiology by Dr Raghuveer100% (1)
- Calcium HomeostasisDocument38 pagesCalcium Homeostasiskelvinmaina9993No ratings yet
- Drugs Affecting Calcium Balance: Harsh Vinayak Roll No. 39 Mbbs 2 Yr Student BATCH 2019 Rdasmc, AyodhyaDocument24 pagesDrugs Affecting Calcium Balance: Harsh Vinayak Roll No. 39 Mbbs 2 Yr Student BATCH 2019 Rdasmc, AyodhyaA2Z GyanNo ratings yet
- 27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFDocument48 pages27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFEITHAR OmarNo ratings yet
- Calcium MetabolismDocument19 pagesCalcium MetabolismShabariNath R NairNo ratings yet
- Lect 9 Parathyroid Gland-1Document30 pagesLect 9 Parathyroid Gland-1warda farooqNo ratings yet
- Learning Objectives Biochemistry of BonesDocument7 pagesLearning Objectives Biochemistry of BonesRaissa GabriellaNo ratings yet
- Calcium MetabolismDocument51 pagesCalcium MetabolismAlan ThomasNo ratings yet
- Regulation of Calcium Parathyroid, Vitamin D & CalcitoninDocument29 pagesRegulation of Calcium Parathyroid, Vitamin D & CalcitoninJessica StewartNo ratings yet
- Calcium, Phos, MGDocument27 pagesCalcium, Phos, MGRiya AktarNo ratings yet
- Renal & Electrolyted Physiology FinalDocument21 pagesRenal & Electrolyted Physiology FinalVondNo ratings yet
- Calcium Phosphorus Metabolic DisordersDocument102 pagesCalcium Phosphorus Metabolic DisordersAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Parathyroid HormonesDocument104 pagesParathyroid Hormonesc96gtf8hkkNo ratings yet
- Calcium HomeostasisDocument37 pagesCalcium Homeostasispolog.jm610No ratings yet
- Calcium Metabolism and Disorders (Hanan)Document169 pagesCalcium Metabolism and Disorders (Hanan)drhananfathyNo ratings yet
- Calcium Balance I 2020Document35 pagesCalcium Balance I 2020Nadun MethwadaneNo ratings yet
- Calcium Metabolism: Presented By-Dr. Chinansha Arya Second Year Postgraduate Department of Conservative and EndodonticsDocument103 pagesCalcium Metabolism: Presented By-Dr. Chinansha Arya Second Year Postgraduate Department of Conservative and EndodonticsmeghaNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- Calcium and PhosporusDocument29 pagesCalcium and PhosporusJoe AjibadeNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismDipak YogiNo ratings yet
- Calcium and Phosphate MetabolismDocument27 pagesCalcium and Phosphate MetabolismIshaq100% (1)
- Study Guide For Calcium and Phosphate MetabolismDocument74 pagesStudy Guide For Calcium and Phosphate MetabolismMohammad MamunuzzamanNo ratings yet
- Mineral 2Document60 pagesMineral 2yixecix709No ratings yet
- Disorders of Calcium, Inorganic Phosphate and Magnesium Metabolism 1Document62 pagesDisorders of Calcium, Inorganic Phosphate and Magnesium Metabolism 1IiiNo ratings yet
- CCCTM FEN HO Rev T199285Document41 pagesCCCTM FEN HO Rev T199285Malte BreitlowNo ratings yet
- Parathyroid-Hormone Calcium HomeostasisDocument58 pagesParathyroid-Hormone Calcium HomeostasisSudhakar LakavathNo ratings yet
- Share Market Report 6Document13 pagesShare Market Report 6Nithish DevadigaNo ratings yet
- Biochemistry: Dr. Dra. Trini Suryowati, MsDocument49 pagesBiochemistry: Dr. Dra. Trini Suryowati, MsDaud ParluhutanNo ratings yet
- Calcium Homeostasis 23,2,14Document51 pagesCalcium Homeostasis 23,2,14Dr ratna kumariNo ratings yet
- Parathormone, CalcitoninDocument14 pagesParathormone, CalcitoninIbrahimNo ratings yet
- 5 Minute Biochemistry PresentationDocument23 pages5 Minute Biochemistry PresentationPITAGAN, Galda Boy 1-FNo ratings yet
- Mineral Metabolism.Document26 pagesMineral Metabolism.Shivanand MaliNo ratings yet
- 4651226Document20 pages4651226bibisupergirlNo ratings yet
- Calcemic Hormones: Leonard Waite, PHD Dept. of Pharmacology and ToxicologyDocument51 pagesCalcemic Hormones: Leonard Waite, PHD Dept. of Pharmacology and ToxicologyPritesh KuNo ratings yet
- Calcium & Phosphorus DentalDocument48 pagesCalcium & Phosphorus Dentalfathimatezil123No ratings yet
- Bone Mineral HomeostasisDocument22 pagesBone Mineral HomeostasisNur Aisyah ZakiNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Calcium, Phosphate, MagnesiumDocument55 pagesCalcium, Phosphate, MagnesiumUdochukwu EnebeNo ratings yet
- CA and Phosphate Metabolism - PDFXDocument25 pagesCA and Phosphate Metabolism - PDFXObsa AhmedNo ratings yet
- Medical Surgical Nursing Module 7Document18 pagesMedical Surgical Nursing Module 7weissNo ratings yet
- Dyskal em Ia: Rs Hana CharitasDocument11 pagesDyskal em Ia: Rs Hana Charitasdwi nugroho prastowoNo ratings yet
- Calcium Metabolism: DR - Ammar Jawad MBCHB, MPHDocument54 pagesCalcium Metabolism: DR - Ammar Jawad MBCHB, MPHMurali ManiNo ratings yet
- 4 - Parathyroid HormoneDocument20 pages4 - Parathyroid HormonedhenaharcaNo ratings yet
- Vitamin D Calcium and PhosphateDocument26 pagesVitamin D Calcium and Phosphatel,Me & MyselfNo ratings yet
- Medical Surgical Nursing Module 8Document9 pagesMedical Surgical Nursing Module 8weissNo ratings yet
- Carbohydrate Metabolism: Sylvia Rianissa PutriDocument47 pagesCarbohydrate Metabolism: Sylvia Rianissa PutriMeilia AndiniNo ratings yet
- Lecture 3 Urea Cycle DisordersDocument27 pagesLecture 3 Urea Cycle Disordersamjadm2002No ratings yet
- Minerals: Role of Minerals in The BodyDocument12 pagesMinerals: Role of Minerals in The BodyZA IDNo ratings yet
- Substances Affecting Bone Mineral HomeostasisDocument33 pagesSubstances Affecting Bone Mineral Homeostasisanaya khan StudentNo ratings yet
- Parathyroid Hormone, Calcitonin, Calcium andDocument61 pagesParathyroid Hormone, Calcitonin, Calcium andchayChay gapolNo ratings yet
- Calcium and PhosphateDocument26 pagesCalcium and Phosphatekhushichunmun gargNo ratings yet
- Endocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsDocument74 pagesEndocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsOngen AchillesNo ratings yet
- A Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesFrom EverandA Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesNo ratings yet
- 2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiDocument65 pages2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiRaja RuzannaNo ratings yet
- GIT InfectionDocument43 pagesGIT InfectionRaja RuzannaNo ratings yet
- HIV&HepatitisDocument46 pagesHIV&HepatitisRaja RuzannaNo ratings yet
- Cassy's MPATH MMB Guide v1.0 (2022)Document104 pagesCassy's MPATH MMB Guide v1.0 (2022)Raja RuzannaNo ratings yet
- Hepatitis VirusesDocument35 pagesHepatitis VirusesRaja RuzannaNo ratings yet
- HIV&HepatitisDocument100 pagesHIV&HepatitisRaja RuzannaNo ratings yet
- Donor Demographics 2015Document13 pagesDonor Demographics 2015Raja RuzannaNo ratings yet
- Recommended TextbooksDocument8 pagesRecommended TextbooksShi Lin Lau0% (1)
- Full Download Holes Human Anatomy and Physiology 15th Edition Shier Solutions ManualDocument35 pagesFull Download Holes Human Anatomy and Physiology 15th Edition Shier Solutions Manualbarovert.o87w100% (33)
- Stan DigestiveDocument3 pagesStan Digestivejoanna carrenNo ratings yet
- Homeostasis Activity - MARY SHESHIRADocument3 pagesHomeostasis Activity - MARY SHESHIRASheshira Reddy YeruvaNo ratings yet
- MODULE-4 Understanding Harmony in The Nature and Existence - WholeDocument9 pagesMODULE-4 Understanding Harmony in The Nature and Existence - WholeTECHNO YASHNo ratings yet
- Mold and Mildew QA Understanding Mold in Your HousevnoznDocument3 pagesMold and Mildew QA Understanding Mold in Your Housevnoznliftvision70No ratings yet
- EcoCRM A Recombinant CRM197 Carrier ProteinDocument1 pageEcoCRM A Recombinant CRM197 Carrier ProteinRamakrishnaNo ratings yet
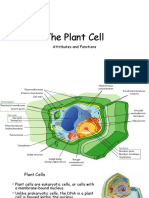
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- GCLP Guidelines 2020 FinalDocument78 pagesGCLP Guidelines 2020 FinalGyanuNo ratings yet
- Epigenetic Age Clock Test Sample ReportDocument78 pagesEpigenetic Age Clock Test Sample ReportHIMMAT SINGHNo ratings yet
- Bio-FIT Book EN PDFDocument256 pagesBio-FIT Book EN PDFCesar Augusto Colorado RamirezNo ratings yet
- Genei Affinity Chromatography Teaching Kit ManualDocument9 pagesGenei Affinity Chromatography Teaching Kit ManualHemant Kawalkar100% (1)
- Anti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractDocument9 pagesAnti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractIJAR JOURNALNo ratings yet
- Biology Photosynthesis CourseworkDocument7 pagesBiology Photosynthesis Courseworkbdg72wjj100% (2)
- Jeffrey Moss, DDS, CNS, DACBN Jeffrey Moss, DDS, CNS, DACBN 413 413 - 530 530 - 0858 (Cell) 0858 (Cell)Document31 pagesJeffrey Moss, DDS, CNS, DACBN Jeffrey Moss, DDS, CNS, DACBN 413 413 - 530 530 - 0858 (Cell) 0858 (Cell)LukasNo ratings yet
- Tenebrio MolitorDocument9 pagesTenebrio Molitorじょしら フィアンナNo ratings yet
- Experiment 12 (Synthesis of Acetylsalicylic Acid)Document8 pagesExperiment 12 (Synthesis of Acetylsalicylic Acid)Cheng Bauzon100% (1)
- Histogenesis of Salivary Gland NeoplasmsDocument18 pagesHistogenesis of Salivary Gland Neoplasmsporkodi sudhaNo ratings yet
- Life Process - Biology MCQDocument3 pagesLife Process - Biology MCQJASMINE VIDHYANo ratings yet
- Psychic DevelopmentDocument13 pagesPsychic DevelopmentCult of Amon Ra100% (2)
- General Biology - Chapter IDocument10 pagesGeneral Biology - Chapter IG.k. Vinnan Rao100% (2)
- 2014 MBAA Chris White Yeast ManagementDocument30 pages2014 MBAA Chris White Yeast ManagementAdrián LampazziNo ratings yet
- The Evolution of Synthetic Thought: Takshashila EssayDocument42 pagesThe Evolution of Synthetic Thought: Takshashila EssayLINDYLL PONO100% (1)
- Food Chemistry: SciencedirectDocument11 pagesFood Chemistry: Sciencedirectratri nurNo ratings yet
- EMBL-EBI Train OnlineDocument19 pagesEMBL-EBI Train OnlineThyagoNo ratings yet
- WDR-Weaver Dice RulebookDocument29 pagesWDR-Weaver Dice RulebookAzazelNo ratings yet
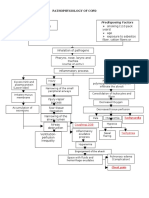
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- B 10 VRV 2042Document36 pagesB 10 VRV 2042api-283593849No ratings yet
- Caplan Deron 201808 PHD CannabisDocument158 pagesCaplan Deron 201808 PHD CannabisMihai SimionNo ratings yet