Download as pdf or txt
You might also like
- Medical Transport Business Plan ExampleDocument49 pagesMedical Transport Business Plan ExampleJoseph QuillNo ratings yet
- Short Cases Article 2014Document2 pagesShort Cases Article 2014DrSajid BuzdarNo ratings yet
- Dermatology Mini-OSCEDocument322 pagesDermatology Mini-OSCEMarrkNo ratings yet
- SurgeryDocument14 pagesSurgeryVinit ChoudharyNo ratings yet
- 11th Teacher, 2nd EditionDocument213 pages11th Teacher, 2nd EditionNadhirah ZulkifliNo ratings yet
- UlcerDocument135 pagesUlcerMahir RathodNo ratings yet
- Sinus, FistulaDocument46 pagesSinus, Fistulaalia0% (1)
- Station 5 CluesDocument41 pagesStation 5 CluesSagit Nauman81No ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- OSCE DermaDocument8 pagesOSCE DermaameerabestNo ratings yet
- Surgery Sheet SchemeDocument51 pagesSurgery Sheet SchemeReem E.MNo ratings yet
- C/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromDocument5 pagesC/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromarsohgahNo ratings yet
- Skin LesionsDocument40 pagesSkin LesionsMizrab NadeemNo ratings yet
- Pancoast TumorDocument26 pagesPancoast TumorDhanis HastinNo ratings yet
- Surgery BookDocument95 pagesSurgery BookKhaled Mahmud100% (1)
- Andre Tan - Surgery (2019)Document456 pagesAndre Tan - Surgery (2019)Lim HuiverNo ratings yet
- Surgery 1. 3-Way Foley Catheter (Latex/silicon) : TherapeuticDocument5 pagesSurgery 1. 3-Way Foley Catheter (Latex/silicon) : TherapeuticMalvinder Singh DhillonNo ratings yet
- Superior Vena Cava ObstructionDocument33 pagesSuperior Vena Cava ObstructionDerek TsangNo ratings yet
- Surgery by HamzaDocument87 pagesSurgery by Hamzasaadalotaibi31No ratings yet
- Diagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020Document16 pagesDiagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Oncologic Emergencies Critical CareDocument11 pagesOncologic Emergencies Critical CareWlad PaCa100% (1)
- OSCE Must Knows For All SubjectsDocument8 pagesOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNo ratings yet
- Corrosive Injury 20061227-1Document23 pagesCorrosive Injury 20061227-1ostaz2000No ratings yet
- Oncological Emergencies-2018Document8 pagesOncological Emergencies-2018CamiloRada100% (1)
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- An Updated Review of Cystic Hepatic LesionsDocument8 pagesAn Updated Review of Cystic Hepatic LesionsMayerlin CalvacheNo ratings yet
- Rokh 2e ST4 PDFDocument141 pagesRokh 2e ST4 PDFMahmud DipuNo ratings yet
- Necrosis and Apoptosis Short Notes For PathologyDocument3 pagesNecrosis and Apoptosis Short Notes For PathologyAlias AliquidNo ratings yet
- Rmu Surgery OspesDocument110 pagesRmu Surgery OspesHumna YounisNo ratings yet
- Hernia Examination SchemeDocument4 pagesHernia Examination Schemeatribecalledquest20No ratings yet
- Comment On Dressing or Bandages and Take Them Down, Comment On ScarsDocument4 pagesComment On Dressing or Bandages and Take Them Down, Comment On ScarsGNo ratings yet
- Pearls of MRCP Part 2 PastestDocument111 pagesPearls of MRCP Part 2 PastestS TNo ratings yet
- Precancerous Conditions of Oral CavityDocument80 pagesPrecancerous Conditions of Oral Cavitylarisabrinza12No ratings yet
- Thyroidectomy Morbidities:: Preventions & InterventionsDocument52 pagesThyroidectomy Morbidities:: Preventions & InterventionsAlfonso DanacNo ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- PRINCIPLES OF SURGERY (James R. Hupp Chapter 3 Notes) : 1. Develop A Surgical DiagnosisDocument5 pagesPRINCIPLES OF SURGERY (James R. Hupp Chapter 3 Notes) : 1. Develop A Surgical DiagnosisSonia LeeNo ratings yet
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- CVS Mini CEX 2Document3 pagesCVS Mini CEX 2Daniel LimNo ratings yet
- Assem Draz: Neurological DisordersDocument26 pagesAssem Draz: Neurological DisordersxuexueNo ratings yet
- C 1+ 2 Surgicl Pathology of OesophagusDocument91 pagesC 1+ 2 Surgicl Pathology of OesophagusSayuridark5No ratings yet
- Systemic Surgery NuggetsDocument17 pagesSystemic Surgery NuggetsAhmad UsmanNo ratings yet
- DD ScrotumDocument4 pagesDD ScrotumAy HaanNo ratings yet
- Matary Swellings 01Document23 pagesMatary Swellings 01toolsdesk1No ratings yet
- Surgery PancreasDocument11 pagesSurgery PancreasMATTHEW EARL MALUMAYNo ratings yet
- Acute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolDocument48 pagesAcute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolNinaNo ratings yet
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- Case of Obstructive JaundiceDocument38 pagesCase of Obstructive JaundiceadiNo ratings yet
- Kidney Part 1Document5 pagesKidney Part 1sarguss14No ratings yet
- Surgery - Principle of Wound Healing and ManagementDocument39 pagesSurgery - Principle of Wound Healing and Managementjue_mardhiahNo ratings yet
- Safe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalDocument4 pagesSafe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalJerahmeel Sombilon GenillaNo ratings yet
- Distal To Ligament of Treitz: CausesDocument8 pagesDistal To Ligament of Treitz: CausesKiara GovenderNo ratings yet
- Thyroid Examination and ThyroidectomyDocument9 pagesThyroid Examination and ThyroidectomyAhmadNo ratings yet
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Medicine Viva Notes by Dr. VaidyaDocument57 pagesMedicine Viva Notes by Dr. VaidyaFariha AnsariNo ratings yet
- STROKEDocument61 pagesSTROKEK.MERCYNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- Eop AnaesDocument26 pagesEop AnaesSheera EiyraaNo ratings yet
- Wa0040.Document1 pageWa0040.Sheera EiyraaNo ratings yet
- GPE in ChildrenDocument4 pagesGPE in ChildrenSheera EiyraaNo ratings yet
- Viva 2 Family MedicineDocument8 pagesViva 2 Family MedicineSheera EiyraaNo ratings yet
- Fammed Viva Posting 5 ZackDocument11 pagesFammed Viva Posting 5 ZackSheera EiyraaNo ratings yet
- Viva 1 Group C FammedDocument6 pagesViva 1 Group C FammedSheera EiyraaNo ratings yet
- DR Geeta Pangi HypertensionDocument6 pagesDR Geeta Pangi HypertensionSheera EiyraaNo ratings yet
- Group 5Document7 pagesGroup 5Sheera EiyraaNo ratings yet
- OPHTHALMOLOGY 2018/2019 Short Case / Long Case Examination (Questions)Document7 pagesOPHTHALMOLOGY 2018/2019 Short Case / Long Case Examination (Questions)Sheera EiyraaNo ratings yet
- Management of Sore ThroatDocument11 pagesManagement of Sore ThroatSheera EiyraaNo ratings yet
- Fever and Rash: - Approach To Patient - HT & Pe - Type of Lesion - Type of Rash - Examples of DiseasesDocument12 pagesFever and Rash: - Approach To Patient - HT & Pe - Type of Lesion - Type of Rash - Examples of DiseasesSheera EiyraaNo ratings yet
- International Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobDocument5 pagesInternational Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobR JNo ratings yet
- Nursing NCP Acute GastroenteritisDocument8 pagesNursing NCP Acute GastroenteritisWinnie AriolaNo ratings yet
- OSMITROL Injection (Mannitol Injection, USP) : in VIAFLEX Plastic ContainerDocument2 pagesOSMITROL Injection (Mannitol Injection, USP) : in VIAFLEX Plastic Containerßhagyesh PatelNo ratings yet
- Current Nutritional Therapies in Inflammatory Bowel Disease - Improving Clinical Remission Rates and Sustainability of Long-Term Dietary TherapiesDocument11 pagesCurrent Nutritional Therapies in Inflammatory Bowel Disease - Improving Clinical Remission Rates and Sustainability of Long-Term Dietary TherapiesAdriana SáNo ratings yet
- ATTUNE S+ Master Content Deck DSUS - JRC - 0517 - 2142Document82 pagesATTUNE S+ Master Content Deck DSUS - JRC - 0517 - 2142medtechy100% (1)
- A 58 Year Old Client Is Admitted With A Diagnosis of Lung CancerDocument9 pagesA 58 Year Old Client Is Admitted With A Diagnosis of Lung CancerNur SanaaniNo ratings yet
- Contraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsDocument3 pagesContraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsSagar HanamasagarNo ratings yet
- Hospital Inspection Format Proforma CompleteDocument9 pagesHospital Inspection Format Proforma CompleteDr Sachin Chitnis M O UPHC AiroliNo ratings yet
- BLS-1Document24 pagesBLS-1Fajar ShahidNo ratings yet
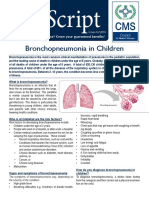
- Bronchopneumonia in ChildrenDocument3 pagesBronchopneumonia in ChildrenputraNo ratings yet
- AccuDEXA Model 7100 User GuideDocument82 pagesAccuDEXA Model 7100 User GuideManuel Vivero DiéguezNo ratings yet
- Medical Surgical Nursing ReviewDocument16 pagesMedical Surgical Nursing ReviewArda LynNo ratings yet
- Black Seed Nigella Sativa A Cure To Every DiseaseDocument6 pagesBlack Seed Nigella Sativa A Cure To Every DiseaseShahmeer KhanNo ratings yet
- CLOZAPINEDocument14 pagesCLOZAPINEsumaryatiNo ratings yet
- Intro PurcomDocument1 pageIntro PurcomAni TubeNo ratings yet
- 04 Worksheet Clariz-A.-DemateraDocument2 pages04 Worksheet Clariz-A.-DemateraashlijquintanaNo ratings yet
- The Society For Vascular Surgery Clinical Practice Guidelines On Popliteal Artery AneurysmsDocument12 pagesThe Society For Vascular Surgery Clinical Practice Guidelines On Popliteal Artery AneurysmsGhaithNo ratings yet
- Tinjauan Alur Prosedur Pelayanan Pasien Rawat Jalan Peserta BPJS Di RSU Imelda Pekerja Indonesia MedanDocument7 pagesTinjauan Alur Prosedur Pelayanan Pasien Rawat Jalan Peserta BPJS Di RSU Imelda Pekerja Indonesia Medannurintan kurniaNo ratings yet
- WHO CINDI Programme-Implemented Projects and Activities in Macedonia, 2001-2005Document5 pagesWHO CINDI Programme-Implemented Projects and Activities in Macedonia, 2001-2005Ass. Prof. Vera Simovska, MD., PhD.100% (1)
- OxyContin (Oxycodone) MundipharmaDocument15 pagesOxyContin (Oxycodone) MundipharmaRayzal AdamNo ratings yet
- Dr. Vibha Hegde - 18Document5 pagesDr. Vibha Hegde - 18Biswaroop ChandraNo ratings yet
- Urologist, Dr. Natan Davoudzadeh Joins NY HealthDocument3 pagesUrologist, Dr. Natan Davoudzadeh Joins NY HealthPR.comNo ratings yet
- Who 2016Document35 pagesWho 2016Herlina InaNo ratings yet
- CASP Checklist: Systematic ReviewDocument5 pagesCASP Checklist: Systematic ReviewWie SeptiaNiNo ratings yet
- Gongsun Sp-4: Grandfather GrandsonDocument2 pagesGongsun Sp-4: Grandfather Grandsonray72roNo ratings yet
- Summary Overview of AB890: Practice Area Topic Area Effective Date Bus. & Prof. Code (BPC) Section ExplanationDocument9 pagesSummary Overview of AB890: Practice Area Topic Area Effective Date Bus. & Prof. Code (BPC) Section Explanationolla0% (1)
- CPOT OriginalDocument9 pagesCPOT OriginalGaby ChocobarNo ratings yet
- AMR Kebijakan WHO - Regulator - BPOMDocument18 pagesAMR Kebijakan WHO - Regulator - BPOMPutri Febrina Rizki AmaliahNo ratings yet
- Acetaminophen - ParacetamolDocument3 pagesAcetaminophen - Paracetamolammar amerNo ratings yet