
Compass Hinge Knee ST
Compass Hinge Knee ST
You might also like
- 300 NPTE Questions and Answers PTMASUD PDFDocument921 pages300 NPTE Questions and Answers PTMASUD PDFManik Mishra75% (8)
- TKR Smith&nephew Technique Orthomatch GENESIS II Surgical Technique.10.17Document32 pagesTKR Smith&nephew Technique Orthomatch GENESIS II Surgical Technique.10.17Ahmed JamalNo ratings yet
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryDocument1 pageDr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryrobertNo ratings yet
- Mountain Dog Enormous and Strong LegsDocument27 pagesMountain Dog Enormous and Strong LegsÂdâm Jônês83% (6)
- Brachial Plexus InjuriesDocument346 pagesBrachial Plexus InjuriesvinaymanNo ratings yet
- MRH Revision Knee Instruments and Technique (Stryker) 5Document29 pagesMRH Revision Knee Instruments and Technique (Stryker) 5saraki234No ratings yet
- JourneyDocument60 pagesJourneyJayjeet BhoiteNo ratings yet
- Freedom Knee Surgical Technique PrintDocument16 pagesFreedom Knee Surgical Technique PrintSagaram ShashidarNo ratings yet
- Legion Porous CR 40830105 UsDocument16 pagesLegion Porous CR 40830105 UsSufyanNo ratings yet
- Legion KneeDocument48 pagesLegion Kneekrueg3rNo ratings yet
- GENESIS II Surgical Technique DCFDocument46 pagesGENESIS II Surgical Technique DCFMazilo VictorNo ratings yet
- Persona Knee Surgical TechniqueDocument72 pagesPersona Knee Surgical TechniquedrorthokingNo ratings yet
- GLBLen Nex Gen Complete Knee Solution Intramedullary Instrumentation FINAL72 Dpi 1Document36 pagesGLBLen Nex Gen Complete Knee Solution Intramedullary Instrumentation FINAL72 Dpi 1Rat MarianNo ratings yet
- Journeyii CR 00344v1 UsDocument40 pagesJourneyii CR 00344v1 UsSufyanNo ratings yet
- Columbus IQ InstrumentsDocument84 pagesColumbus IQ Instrumentst5cfdcw977No ratings yet
- GTS Surgical TechniqueDocument22 pagesGTS Surgical TechniqueMaurinho MnhNo ratings yet
- The Casparevolution System Anterior Cervical PlatingDocument15 pagesThe Casparevolution System Anterior Cervical PlatingJose Esteban Gomez LiscanoNo ratings yet
- Open Reduction and Internal Fixation of Distal Femoral Fractures in Adults Technique Approach Considerations, Angled Blade PlatDocument1 pageOpen Reduction and Internal Fixation of Distal Femoral Fractures in Adults Technique Approach Considerations, Angled Blade PlatRamiel ChristopherNo ratings yet
- Clavo Expert LFN Diafisis FemurDocument84 pagesClavo Expert LFN Diafisis FemurC Martin TraumatoNo ratings yet
- Nexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueDocument32 pagesNexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueTudor MadalinaNo ratings yet
- 1609.1-GLBL-En NexGen Prime Knee Surgical Technique-FINAL 72dpi1Document60 pages1609.1-GLBL-En NexGen Prime Knee Surgical Technique-FINAL 72dpi1Rat MarianNo ratings yet
- Secur-Fit Advanced: Surgical TechniqueDocument28 pagesSecur-Fit Advanced: Surgical TechniqueX ComNo ratings yet
- Diaphyseal Fixation Using Long Tapered StemDocument19 pagesDiaphyseal Fixation Using Long Tapered StemPurushotham NalamatiNo ratings yet
- Genesis II Revision Surgical TechniqueDocument36 pagesGenesis II Revision Surgical TechniquequetecojaunburroNo ratings yet
- Tec Cirurgica Minimax99 13mm 12 Eng-1Document16 pagesTec Cirurgica Minimax99 13mm 12 Eng-1SufyanNo ratings yet
- HOMBRO DE REVERSA BiometDocument60 pagesHOMBRO DE REVERSA BiometCristian Aline Osorio HernandezNo ratings yet
- U2 Knee Ps TecnicaDocument52 pagesU2 Knee Ps TecnicaIsabella MarulandaNo ratings yet
- MDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical Technique 97-2252-005-01 Rev3!09!2011Document28 pagesMDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical Technique 97-2252-005-01 Rev3!09!2011cukiNo ratings yet
- M.U.S.T MINI - Posterior Cervical Screw SytemDocument20 pagesM.U.S.T MINI - Posterior Cervical Screw Sytemmaelained4No ratings yet
- Nexgen Complete Knee Solution: ZimmerDocument37 pagesNexgen Complete Knee Solution: Zimmerflo1987No ratings yet
- MK006 105Document20 pagesMK006 105C Martin TraumatoNo ratings yet
- Placa Cervical Anterior AtlantisDocument39 pagesPlaca Cervical Anterior AtlantisJavier Peña ChavezNo ratings yet
- Comp RVS ST 2019 PDFDocument60 pagesComp RVS ST 2019 PDFYair Alvarez OjedaNo ratings yet
- USER MANUAL TERBARU - Id.enDocument3 pagesUSER MANUAL TERBARU - Id.enAndri aryanataNo ratings yet
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Document48 pagesNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987No ratings yet
- v1 Acufex Pinpoint TG Digital 0321Document12 pagesv1 Acufex Pinpoint TG Digital 0321Alejandro SalinasNo ratings yet
- Large - Distractor - Femur UputstvoDocument15 pagesLarge - Distractor - Femur Uputstvoana starcevicNo ratings yet
- DPEM ORT 0812 0182a 1 - LRDocument32 pagesDPEM ORT 0812 0182a 1 - LRVladimir NikopolNo ratings yet
- ZNN Retrograde NailDocument24 pagesZNN Retrograde Nailmisterx73No ratings yet
- 8238 036.000.033 PDFDocument24 pages8238 036.000.033 PDFRaymond ParungNo ratings yet
- Magna FX Cannulated Screw Fixation Sytem Abbreviated Surgical TechniqueDocument4 pagesMagna FX Cannulated Screw Fixation Sytem Abbreviated Surgical TechniqueAnonymous a3JsNXNNo ratings yet
- Avenir Hip System Surgical TechniqueDocument16 pagesAvenir Hip System Surgical Techniquesuraj mahadikNo ratings yet
- Osmedic Orthofix Albue Fixator Operative TechniqueDocument27 pagesOsmedic Orthofix Albue Fixator Operative TechniqueAshok RathinaveluNo ratings yet
- R3 Surgical Technique - IntlDocument27 pagesR3 Surgical Technique - Intlquetecojaunburro100% (1)
- Arthroscopic Shoulder Repair Using The Smith & Nephew Footprint PK Suture AnchorDocument12 pagesArthroscopic Shoulder Repair Using The Smith & Nephew Footprint PK Suture Anchorapi-19808945No ratings yet
- 9485 R0 NuNec Surgical Technique 8-30-16Document24 pages9485 R0 NuNec Surgical Technique 8-30-16BobNo ratings yet
- Articulators in Complete Dentures - WORD - 1Document13 pagesArticulators in Complete Dentures - WORD - 1radhikamiNo ratings yet
- Mosaicplasty 1030208g UsDocument12 pagesMosaicplasty 1030208g UsAnil SoodNo ratings yet
- BHR SurgicalTechniqueDocument50 pagesBHR SurgicalTechniqueingridbach100% (1)
- Articulators: DR - Muhammad Aamir Rafiq Assistant ProfDocument52 pagesArticulators: DR - Muhammad Aamir Rafiq Assistant Profnauman tariqNo ratings yet
- All On Four - The Basics - Jimson 2016Document5 pagesAll On Four - The Basics - Jimson 2016Natalia AcevedoNo ratings yet
- Zimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevDocument38 pagesZimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevNIku ChanNo ratings yet
- PFC RP Surgical Technique (DePuy)Document43 pagesPFC RP Surgical Technique (DePuy)Sagaram Shashidar100% (1)
- Bankart Repair Using The Smith & Nephew BIORAPTOR™ 2.9 Suture AnchorDocument7 pagesBankart Repair Using The Smith & Nephew BIORAPTOR™ 2.9 Suture Anchorapi-19808945No ratings yet
- Short Reconstruction NailDocument14 pagesShort Reconstruction NailSimona DraganNo ratings yet
- Splints and Casts: Indications and MethodsDocument9 pagesSplints and Casts: Indications and Methodsjeremy1roseNo ratings yet
- Acumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CDocument20 pagesAcumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CMark SharonNo ratings yet
- Meniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewDocument16 pagesMeniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewAlejandro RodriguezNo ratings yet
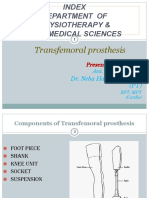
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanNo ratings yet
- CHS Catalog TehnicaDocument32 pagesCHS Catalog TehnicaIon GhercaviNo ratings yet
- Wise-Lock Modular Hand - Foot SystemDocument47 pagesWise-Lock Modular Hand - Foot SystemDJGGNo ratings yet
- Broken Screw Removal SystemDocument16 pagesBroken Screw Removal SystemDJGGNo ratings yet
- DYNEXQuick ReferenceDocument15 pagesDYNEXQuick ReferenceDJGGNo ratings yet
- HPS STGDocument33 pagesHPS STGDJGGNo ratings yet
- Awb 787399845149Document2 pagesAwb 787399845149DJGGNo ratings yet
- Distal Femoral Osteotomy System: Surgical TechniqueDocument26 pagesDistal Femoral Osteotomy System: Surgical TechniqueDJGGNo ratings yet
- H 3 LRFDocument44 pagesH 3 LRFDJGGNo ratings yet
- Titanium Locking Screw and Bolts For Im Nails.J3686CDocument2 pagesTitanium Locking Screw and Bolts For Im Nails.J3686CDJGGNo ratings yet
- Primary Tray: Nique Evice DentificationDocument8 pagesPrimary Tray: Nique Evice DentificationDJGGNo ratings yet
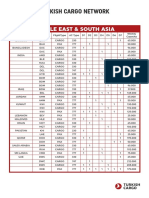
- Turkish Cargo Network: Middle East & South AsiaDocument6 pagesTurkish Cargo Network: Middle East & South AsiaDJGGNo ratings yet
- DECOR-100 Series: Bathroom Extract FansDocument7 pagesDECOR-100 Series: Bathroom Extract FansDJGGNo ratings yet
- C L A S S 1 0 0 0 0 S E R I E S 1 2 H D Series 12 Standard Hub HD Fan Right Hand RotationDocument1 pageC L A S S 1 0 0 0 0 S E R I E S 1 2 H D Series 12 Standard Hub HD Fan Right Hand RotationDJGGNo ratings yet
- Respirator Models No Longer Authorized COVID19 - 0Document7 pagesRespirator Models No Longer Authorized COVID19 - 0DJGGNo ratings yet
- Low Iodine Diet: What Is The Thyroid Gland?Document1 pageLow Iodine Diet: What Is The Thyroid Gland?DJGGNo ratings yet
- Orthotics and Prosthetics LectureDocument40 pagesOrthotics and Prosthetics LectureRock Obaidat100% (1)
- Shoulder ReductionDocument4 pagesShoulder ReductionWaqas HaleemNo ratings yet
- Suture Anchor Fixation For Scaphoid Nonunions With Small Proximal Fragments - Report of 11 CasesDocument6 pagesSuture Anchor Fixation For Scaphoid Nonunions With Small Proximal Fragments - Report of 11 CasesLUIS SALVADOR FLORESNo ratings yet
- Kano State College of Nursing and Midwifery: Club FootDocument20 pagesKano State College of Nursing and Midwifery: Club FootMuhammad Daha SanusiNo ratings yet
- Barbell Exercises For Legs: Site NavigationDocument4 pagesBarbell Exercises For Legs: Site NavigationAbdullah Ibn MubarakNo ratings yet
- Surgey MCQSDocument95 pagesSurgey MCQSZain HadiNo ratings yet
- Low Profile MTP Plate Surgical Technique: © 2012, Arthrex Inc. All Rights Reserved. LT1-0457-EN - GDocument4 pagesLow Profile MTP Plate Surgical Technique: © 2012, Arthrex Inc. All Rights Reserved. LT1-0457-EN - GSomon IsupovNo ratings yet
- ACPOMIT Workshop-Hand and WristDocument20 pagesACPOMIT Workshop-Hand and WristRezaul RajibNo ratings yet
- PAETDocument34 pagesPAETEsterGrefielNo ratings yet
- Motor Relearning ProgrammeDocument36 pagesMotor Relearning Programmerabia khalidNo ratings yet
- Kitai 1989 Et - Al, - Specificity of Joint Angle in Isometric TrainingDocument5 pagesKitai 1989 Et - Al, - Specificity of Joint Angle in Isometric Trainingok okNo ratings yet
- Schober TestDocument1 pageSchober TestAtet KurniadiNo ratings yet
- AnatDocument31 pagesAnatBintang ParipurnaNo ratings yet
- Ankle and Lower Leg Rehabilitation: © 2010 Mcgraw-Hill Higher Education. All Rights ReservedDocument63 pagesAnkle and Lower Leg Rehabilitation: © 2010 Mcgraw-Hill Higher Education. All Rights ReservedniekoNo ratings yet
- AnatomyDocument121 pagesAnatomyBlack InsomniaNo ratings yet
- 2017 Book DiagnosisAndManagementOfFemoro PDFDocument279 pages2017 Book DiagnosisAndManagementOfFemoro PDFIvan Guillermo Torres100% (1)
- Solomon Ankle Injury PDFDocument9 pagesSolomon Ankle Injury PDFHikmah Wahid AkbarNo ratings yet
- وضعيات ViewDocument23 pagesوضعيات ViewomarNo ratings yet
- Beginner - Intermediate: 4 Weeks To Total Hip MobilityDocument14 pagesBeginner - Intermediate: 4 Weeks To Total Hip Mobility714 BaliNo ratings yet
- Tegner Lysholm Knee Scoring Scale - Orthopaedic ScoresDocument2 pagesTegner Lysholm Knee Scoring Scale - Orthopaedic Scoresradu_pavalache100% (2)
- Physiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolsDocument76 pagesPhysiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolskoriatsuNo ratings yet
- Assessment MusculoskeletalDocument33 pagesAssessment MusculoskeletalRubinNo ratings yet
- Pilates TrainingDocument4 pagesPilates TrainingJoshua EreterinoNo ratings yet
- Dcia (Deep Circumflex Iliac Artery) FlapDocument43 pagesDcia (Deep Circumflex Iliac Artery) FlapRohit SharmaNo ratings yet
- Casting Techniques For Foot Orthosis - DevadriDocument37 pagesCasting Techniques For Foot Orthosis - DevadriDevadri DeyNo ratings yet
- Crivit Workout Bench - 311166 - ENDocument50 pagesCrivit Workout Bench - 311166 - ENW1ngch0nNo ratings yet





































































































Download as pdf or txt
You might also like
- 300 NPTE Questions and Answers PTMASUD PDFDocument921 pages300 NPTE Questions and Answers PTMASUD PDFManik Mishra75% (8)
- TKR Smith&nephew Technique Orthomatch GENESIS II Surgical Technique.10.17Document32 pagesTKR Smith&nephew Technique Orthomatch GENESIS II Surgical Technique.10.17Ahmed JamalNo ratings yet
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryDocument1 pageDr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryrobertNo ratings yet
- Mountain Dog Enormous and Strong LegsDocument27 pagesMountain Dog Enormous and Strong LegsÂdâm Jônês83% (6)
- Brachial Plexus InjuriesDocument346 pagesBrachial Plexus InjuriesvinaymanNo ratings yet
- MRH Revision Knee Instruments and Technique (Stryker) 5Document29 pagesMRH Revision Knee Instruments and Technique (Stryker) 5saraki234No ratings yet
- JourneyDocument60 pagesJourneyJayjeet BhoiteNo ratings yet
- Freedom Knee Surgical Technique PrintDocument16 pagesFreedom Knee Surgical Technique PrintSagaram ShashidarNo ratings yet
- Legion Porous CR 40830105 UsDocument16 pagesLegion Porous CR 40830105 UsSufyanNo ratings yet
- Legion KneeDocument48 pagesLegion Kneekrueg3rNo ratings yet
- GENESIS II Surgical Technique DCFDocument46 pagesGENESIS II Surgical Technique DCFMazilo VictorNo ratings yet
- Persona Knee Surgical TechniqueDocument72 pagesPersona Knee Surgical TechniquedrorthokingNo ratings yet
- GLBLen Nex Gen Complete Knee Solution Intramedullary Instrumentation FINAL72 Dpi 1Document36 pagesGLBLen Nex Gen Complete Knee Solution Intramedullary Instrumentation FINAL72 Dpi 1Rat MarianNo ratings yet
- Journeyii CR 00344v1 UsDocument40 pagesJourneyii CR 00344v1 UsSufyanNo ratings yet
- Columbus IQ InstrumentsDocument84 pagesColumbus IQ Instrumentst5cfdcw977No ratings yet
- GTS Surgical TechniqueDocument22 pagesGTS Surgical TechniqueMaurinho MnhNo ratings yet
- The Casparevolution System Anterior Cervical PlatingDocument15 pagesThe Casparevolution System Anterior Cervical PlatingJose Esteban Gomez LiscanoNo ratings yet
- Open Reduction and Internal Fixation of Distal Femoral Fractures in Adults Technique Approach Considerations, Angled Blade PlatDocument1 pageOpen Reduction and Internal Fixation of Distal Femoral Fractures in Adults Technique Approach Considerations, Angled Blade PlatRamiel ChristopherNo ratings yet
- Clavo Expert LFN Diafisis FemurDocument84 pagesClavo Expert LFN Diafisis FemurC Martin TraumatoNo ratings yet
- Nexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueDocument32 pagesNexgen Complete Knee Solution Epicondylar Instrumentation Surgical Technique For Legacy Posterior Stabalized Knees Surgical TechniqueTudor MadalinaNo ratings yet
- 1609.1-GLBL-En NexGen Prime Knee Surgical Technique-FINAL 72dpi1Document60 pages1609.1-GLBL-En NexGen Prime Knee Surgical Technique-FINAL 72dpi1Rat MarianNo ratings yet
- Secur-Fit Advanced: Surgical TechniqueDocument28 pagesSecur-Fit Advanced: Surgical TechniqueX ComNo ratings yet
- Diaphyseal Fixation Using Long Tapered StemDocument19 pagesDiaphyseal Fixation Using Long Tapered StemPurushotham NalamatiNo ratings yet
- Genesis II Revision Surgical TechniqueDocument36 pagesGenesis II Revision Surgical TechniquequetecojaunburroNo ratings yet
- Tec Cirurgica Minimax99 13mm 12 Eng-1Document16 pagesTec Cirurgica Minimax99 13mm 12 Eng-1SufyanNo ratings yet
- HOMBRO DE REVERSA BiometDocument60 pagesHOMBRO DE REVERSA BiometCristian Aline Osorio HernandezNo ratings yet
- U2 Knee Ps TecnicaDocument52 pagesU2 Knee Ps TecnicaIsabella MarulandaNo ratings yet
- MDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical Technique 97-2252-005-01 Rev3!09!2011Document28 pagesMDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical Technique 97-2252-005-01 Rev3!09!2011cukiNo ratings yet
- M.U.S.T MINI - Posterior Cervical Screw SytemDocument20 pagesM.U.S.T MINI - Posterior Cervical Screw Sytemmaelained4No ratings yet
- Nexgen Complete Knee Solution: ZimmerDocument37 pagesNexgen Complete Knee Solution: Zimmerflo1987No ratings yet
- MK006 105Document20 pagesMK006 105C Martin TraumatoNo ratings yet
- Placa Cervical Anterior AtlantisDocument39 pagesPlaca Cervical Anterior AtlantisJavier Peña ChavezNo ratings yet
- Comp RVS ST 2019 PDFDocument60 pagesComp RVS ST 2019 PDFYair Alvarez OjedaNo ratings yet
- USER MANUAL TERBARU - Id.enDocument3 pagesUSER MANUAL TERBARU - Id.enAndri aryanataNo ratings yet
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Document48 pagesNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987No ratings yet
- v1 Acufex Pinpoint TG Digital 0321Document12 pagesv1 Acufex Pinpoint TG Digital 0321Alejandro SalinasNo ratings yet
- Large - Distractor - Femur UputstvoDocument15 pagesLarge - Distractor - Femur Uputstvoana starcevicNo ratings yet
- DPEM ORT 0812 0182a 1 - LRDocument32 pagesDPEM ORT 0812 0182a 1 - LRVladimir NikopolNo ratings yet
- ZNN Retrograde NailDocument24 pagesZNN Retrograde Nailmisterx73No ratings yet
- 8238 036.000.033 PDFDocument24 pages8238 036.000.033 PDFRaymond ParungNo ratings yet
- Magna FX Cannulated Screw Fixation Sytem Abbreviated Surgical TechniqueDocument4 pagesMagna FX Cannulated Screw Fixation Sytem Abbreviated Surgical TechniqueAnonymous a3JsNXNNo ratings yet
- Avenir Hip System Surgical TechniqueDocument16 pagesAvenir Hip System Surgical Techniquesuraj mahadikNo ratings yet
- Osmedic Orthofix Albue Fixator Operative TechniqueDocument27 pagesOsmedic Orthofix Albue Fixator Operative TechniqueAshok RathinaveluNo ratings yet
- R3 Surgical Technique - IntlDocument27 pagesR3 Surgical Technique - Intlquetecojaunburro100% (1)
- Arthroscopic Shoulder Repair Using The Smith & Nephew Footprint PK Suture AnchorDocument12 pagesArthroscopic Shoulder Repair Using The Smith & Nephew Footprint PK Suture Anchorapi-19808945No ratings yet
- 9485 R0 NuNec Surgical Technique 8-30-16Document24 pages9485 R0 NuNec Surgical Technique 8-30-16BobNo ratings yet
- Articulators in Complete Dentures - WORD - 1Document13 pagesArticulators in Complete Dentures - WORD - 1radhikamiNo ratings yet
- Mosaicplasty 1030208g UsDocument12 pagesMosaicplasty 1030208g UsAnil SoodNo ratings yet
- BHR SurgicalTechniqueDocument50 pagesBHR SurgicalTechniqueingridbach100% (1)
- Articulators: DR - Muhammad Aamir Rafiq Assistant ProfDocument52 pagesArticulators: DR - Muhammad Aamir Rafiq Assistant Profnauman tariqNo ratings yet
- All On Four - The Basics - Jimson 2016Document5 pagesAll On Four - The Basics - Jimson 2016Natalia AcevedoNo ratings yet
- Zimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevDocument38 pagesZimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevNIku ChanNo ratings yet
- PFC RP Surgical Technique (DePuy)Document43 pagesPFC RP Surgical Technique (DePuy)Sagaram Shashidar100% (1)
- Bankart Repair Using The Smith & Nephew BIORAPTOR™ 2.9 Suture AnchorDocument7 pagesBankart Repair Using The Smith & Nephew BIORAPTOR™ 2.9 Suture Anchorapi-19808945No ratings yet
- Short Reconstruction NailDocument14 pagesShort Reconstruction NailSimona DraganNo ratings yet
- Splints and Casts: Indications and MethodsDocument9 pagesSplints and Casts: Indications and Methodsjeremy1roseNo ratings yet
- Acumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CDocument20 pagesAcumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CMark SharonNo ratings yet
- Meniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewDocument16 pagesMeniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewAlejandro RodriguezNo ratings yet
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanNo ratings yet
- CHS Catalog TehnicaDocument32 pagesCHS Catalog TehnicaIon GhercaviNo ratings yet
- Wise-Lock Modular Hand - Foot SystemDocument47 pagesWise-Lock Modular Hand - Foot SystemDJGGNo ratings yet
- Broken Screw Removal SystemDocument16 pagesBroken Screw Removal SystemDJGGNo ratings yet
- DYNEXQuick ReferenceDocument15 pagesDYNEXQuick ReferenceDJGGNo ratings yet
- HPS STGDocument33 pagesHPS STGDJGGNo ratings yet
- Awb 787399845149Document2 pagesAwb 787399845149DJGGNo ratings yet
- Distal Femoral Osteotomy System: Surgical TechniqueDocument26 pagesDistal Femoral Osteotomy System: Surgical TechniqueDJGGNo ratings yet
- H 3 LRFDocument44 pagesH 3 LRFDJGGNo ratings yet
- Titanium Locking Screw and Bolts For Im Nails.J3686CDocument2 pagesTitanium Locking Screw and Bolts For Im Nails.J3686CDJGGNo ratings yet
- Primary Tray: Nique Evice DentificationDocument8 pagesPrimary Tray: Nique Evice DentificationDJGGNo ratings yet
- Turkish Cargo Network: Middle East & South AsiaDocument6 pagesTurkish Cargo Network: Middle East & South AsiaDJGGNo ratings yet
- DECOR-100 Series: Bathroom Extract FansDocument7 pagesDECOR-100 Series: Bathroom Extract FansDJGGNo ratings yet
- C L A S S 1 0 0 0 0 S E R I E S 1 2 H D Series 12 Standard Hub HD Fan Right Hand RotationDocument1 pageC L A S S 1 0 0 0 0 S E R I E S 1 2 H D Series 12 Standard Hub HD Fan Right Hand RotationDJGGNo ratings yet
- Respirator Models No Longer Authorized COVID19 - 0Document7 pagesRespirator Models No Longer Authorized COVID19 - 0DJGGNo ratings yet
- Low Iodine Diet: What Is The Thyroid Gland?Document1 pageLow Iodine Diet: What Is The Thyroid Gland?DJGGNo ratings yet
- Orthotics and Prosthetics LectureDocument40 pagesOrthotics and Prosthetics LectureRock Obaidat100% (1)
- Shoulder ReductionDocument4 pagesShoulder ReductionWaqas HaleemNo ratings yet
- Suture Anchor Fixation For Scaphoid Nonunions With Small Proximal Fragments - Report of 11 CasesDocument6 pagesSuture Anchor Fixation For Scaphoid Nonunions With Small Proximal Fragments - Report of 11 CasesLUIS SALVADOR FLORESNo ratings yet
- Kano State College of Nursing and Midwifery: Club FootDocument20 pagesKano State College of Nursing and Midwifery: Club FootMuhammad Daha SanusiNo ratings yet
- Barbell Exercises For Legs: Site NavigationDocument4 pagesBarbell Exercises For Legs: Site NavigationAbdullah Ibn MubarakNo ratings yet
- Surgey MCQSDocument95 pagesSurgey MCQSZain HadiNo ratings yet
- Low Profile MTP Plate Surgical Technique: © 2012, Arthrex Inc. All Rights Reserved. LT1-0457-EN - GDocument4 pagesLow Profile MTP Plate Surgical Technique: © 2012, Arthrex Inc. All Rights Reserved. LT1-0457-EN - GSomon IsupovNo ratings yet
- ACPOMIT Workshop-Hand and WristDocument20 pagesACPOMIT Workshop-Hand and WristRezaul RajibNo ratings yet
- PAETDocument34 pagesPAETEsterGrefielNo ratings yet
- Motor Relearning ProgrammeDocument36 pagesMotor Relearning Programmerabia khalidNo ratings yet
- Kitai 1989 Et - Al, - Specificity of Joint Angle in Isometric TrainingDocument5 pagesKitai 1989 Et - Al, - Specificity of Joint Angle in Isometric Trainingok okNo ratings yet
- Schober TestDocument1 pageSchober TestAtet KurniadiNo ratings yet
- AnatDocument31 pagesAnatBintang ParipurnaNo ratings yet
- Ankle and Lower Leg Rehabilitation: © 2010 Mcgraw-Hill Higher Education. All Rights ReservedDocument63 pagesAnkle and Lower Leg Rehabilitation: © 2010 Mcgraw-Hill Higher Education. All Rights ReservedniekoNo ratings yet
- AnatomyDocument121 pagesAnatomyBlack InsomniaNo ratings yet
- 2017 Book DiagnosisAndManagementOfFemoro PDFDocument279 pages2017 Book DiagnosisAndManagementOfFemoro PDFIvan Guillermo Torres100% (1)
- Solomon Ankle Injury PDFDocument9 pagesSolomon Ankle Injury PDFHikmah Wahid AkbarNo ratings yet
- وضعيات ViewDocument23 pagesوضعيات ViewomarNo ratings yet
- Beginner - Intermediate: 4 Weeks To Total Hip MobilityDocument14 pagesBeginner - Intermediate: 4 Weeks To Total Hip Mobility714 BaliNo ratings yet
- Tegner Lysholm Knee Scoring Scale - Orthopaedic ScoresDocument2 pagesTegner Lysholm Knee Scoring Scale - Orthopaedic Scoresradu_pavalache100% (2)
- Physiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolsDocument76 pagesPhysiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolskoriatsuNo ratings yet
- Assessment MusculoskeletalDocument33 pagesAssessment MusculoskeletalRubinNo ratings yet
- Pilates TrainingDocument4 pagesPilates TrainingJoshua EreterinoNo ratings yet
- Dcia (Deep Circumflex Iliac Artery) FlapDocument43 pagesDcia (Deep Circumflex Iliac Artery) FlapRohit SharmaNo ratings yet
- Casting Techniques For Foot Orthosis - DevadriDocument37 pagesCasting Techniques For Foot Orthosis - DevadriDevadri DeyNo ratings yet
- Crivit Workout Bench - 311166 - ENDocument50 pagesCrivit Workout Bench - 311166 - ENW1ngch0nNo ratings yet