Download as pdf or txt
You might also like
- Virtual Cardiologist LabDocument2 pagesVirtual Cardiologist LabVinsmoke SanjiNo ratings yet
- Mitral StenosisDocument29 pagesMitral Stenosisrameshbmc100% (7)
- Acls Algorithms 2021 ChecklistDocument1 pageAcls Algorithms 2021 ChecklistpepNo ratings yet
- Cardiac/Cardiogenic Shock: Clinical Practice GuidelinesDocument3 pagesCardiac/Cardiogenic Shock: Clinical Practice GuidelinesAnonymous Yo0mStNo ratings yet
- CV Karman TandonDocument3 pagesCV Karman TandonkarmantandonNo ratings yet
- Hypertonic Saline Attenuates Cord Swelling and Edema in Experimental Cord Injury - Experimental (2009) PDFDocument7 pagesHypertonic Saline Attenuates Cord Swelling and Edema in Experimental Cord Injury - Experimental (2009) PDFCoal CoalyNo ratings yet
- Echo 2Document16 pagesEcho 2Indera VyasNo ratings yet
- Mesenchymal Stem Cell Implantation in A Swine Myocardial Infarct Model: Engraftment and Functional EffectsDocument8 pagesMesenchymal Stem Cell Implantation in A Swine Myocardial Infarct Model: Engraftment and Functional EffectsAndrés AlvaradoNo ratings yet
- Fitzpatrick 2016Document13 pagesFitzpatrick 2016smansa123No ratings yet
- Jurnal 12Document10 pagesJurnal 12Zella ZakyaNo ratings yet
- Stem Cell Transplantation: The Lung Barrier: Cite This PaperDocument5 pagesStem Cell Transplantation: The Lung Barrier: Cite This Paper190384205058 Cilsa Nabila Hilal MandalikoNo ratings yet
- Physical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelDocument8 pagesPhysical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelNicoleta Popa-FoteaNo ratings yet
- 475 929 2 PBDocument6 pages475 929 2 PBErfaniNo ratings yet
- Evaluation of Morphological Changes in Experimental Models of Myocardial Infarction: Electron and Light Microscopical EvidenceDocument11 pagesEvaluation of Morphological Changes in Experimental Models of Myocardial Infarction: Electron and Light Microscopical EvidenceRania QhalisyaNo ratings yet
- Borenstein 05Document9 pagesBorenstein 05emmanuel le bretNo ratings yet
- JCTVS Myxo Ring Clinical Trial 2008Document9 pagesJCTVS Myxo Ring Clinical Trial 2008Nalini RajamannanNo ratings yet
- Comparizon of K-X and IsofluraneDocument24 pagesComparizon of K-X and IsofluraneIgnacio BarbieriNo ratings yet
- Volatile Anaesthetic Myocardial Protection: A Review of The Current LiteratureDocument5 pagesVolatile Anaesthetic Myocardial Protection: A Review of The Current Literatureserena7205No ratings yet
- Ischemic Preconditioning Does Not Acutely Improve Load-Insensitive Parameters of Contractility in in Vivo Stunned Porcine MyocardiumDocument8 pagesIschemic Preconditioning Does Not Acutely Improve Load-Insensitive Parameters of Contractility in in Vivo Stunned Porcine MyocardiumSol SolNo ratings yet
- Epidermoid Cysts TNEDocument10 pagesEpidermoid Cysts TNEbello_england_209552No ratings yet
- NeuralRegenRes9184-8563115 234711Document8 pagesNeuralRegenRes9184-8563115 234711JouleAlSBNo ratings yet
- Original Article: Transforming Growth Factor Beta-1 (Document8 pagesOriginal Article: Transforming Growth Factor Beta-1 (Lussiana Folleco InsuastyNo ratings yet
- Analysis and Results of Prolonged Resuscitation in Cardiac Arrest Patients Rescued by Extracorporeal Membrane OxygenationDocument7 pagesAnalysis and Results of Prolonged Resuscitation in Cardiac Arrest Patients Rescued by Extracorporeal Membrane OxygenationMuhammad RizqiNo ratings yet
- Determinants of Delayed Preconditioning Against Myocardial PDFDocument19 pagesDeterminants of Delayed Preconditioning Against Myocardial PDFSol SolNo ratings yet
- The Early Response To Major Trauma and Intramedullary Nailing PDFDocument5 pagesThe Early Response To Major Trauma and Intramedullary Nailing PDFantonio dengNo ratings yet
- Clinical Research: Heart Failure/cardiomyopathyDocument8 pagesClinical Research: Heart Failure/cardiomyopathyNoel Saúl Argüello SánchezNo ratings yet
- Sel Mesenkim 4Document10 pagesSel Mesenkim 4Ida Ifan YulianaNo ratings yet
- Acute Coronary Syndrome in Two Patients With Mechanical Valve ProsthesesDocument5 pagesAcute Coronary Syndrome in Two Patients With Mechanical Valve ProsthesesgalalNo ratings yet
- Cardio ResusiDocument9 pagesCardio ResusiDanarFauzanAdiPrayitnoNo ratings yet
- AJP Heart and Circulatory Physiology Volume 287 Issue 2 2004 (Doi 10.1152 - Ajpheart.01247.2003) Hodgson, D. M. - Stable Benefit of EmbryonDocument10 pagesAJP Heart and Circulatory Physiology Volume 287 Issue 2 2004 (Doi 10.1152 - Ajpheart.01247.2003) Hodgson, D. M. - Stable Benefit of EmbryonArini Dwi NastitiNo ratings yet
- Endovascular Treatment of Intracranial Aneurysms: Initial Experience in A Low-Volume CenterDocument5 pagesEndovascular Treatment of Intracranial Aneurysms: Initial Experience in A Low-Volume CenterAswin ChristantoNo ratings yet
- Circulation Research-2015 - E81-94Document40 pagesCirculation Research-2015 - E81-94acNo ratings yet
- Final Histological Assessment of Spinal Cord Injury - RevisedDocument18 pagesFinal Histological Assessment of Spinal Cord Injury - Revisedapi-308976551No ratings yet
- Rodriguez2005-Cognitive Dysfunction After Total Knee Arthroplasty - Effects of Intraoperative Cerebral Embolization and Postoperative ComplicationsDocument9 pagesRodriguez2005-Cognitive Dysfunction After Total Knee Arthroplasty - Effects of Intraoperative Cerebral Embolization and Postoperative ComplicationsSyahpikal SahanaNo ratings yet
- Disseccao Tipo b2Document6 pagesDisseccao Tipo b2coopervascba.diradmNo ratings yet
- EJVES VF Watanabe April 2020Document4 pagesEJVES VF Watanabe April 2020Francisco Álvarez MarcosNo ratings yet
- Barsheshet 2007Document7 pagesBarsheshet 2007Bambang DwiputraNo ratings yet
- Craneoplastia y Regulacion FSC Germany 00Document9 pagesCraneoplastia y Regulacion FSC Germany 00djcafNo ratings yet
- Intracardiac Echocardiography2Document12 pagesIntracardiac Echocardiography2Salah AttaNo ratings yet
- Etm 14 4 3563 PDFDocument6 pagesEtm 14 4 3563 PDFUlfahNo ratings yet
- Xin 2013Document5 pagesXin 2013Maximiliano PfannlNo ratings yet
- Tissue EngineeringDocument12 pagesTissue EngineeringcerebruzNo ratings yet
- Article - Sequential Bypass Grafting On The Beating Heart - Blood Flow CharacteristicsDocument4 pagesArticle - Sequential Bypass Grafting On The Beating Heart - Blood Flow Characteristicsfluid_man_brazilNo ratings yet
- Cerebral Monitoring During Carotid Endarterectomy by Transcranial Doppler UltrasonographyDocument5 pagesCerebral Monitoring During Carotid Endarterectomy by Transcranial Doppler UltrasonographyAmira DayoubNo ratings yet
- Ross OtoHNS2005 ArterialCouplingDocument5 pagesRoss OtoHNS2005 ArterialCouplingSungjin SongNo ratings yet
- Recombinant Human Vascular Endothelial Growth Factor Enhances Bone Healing in An Experimental Nonunion ModelDocument9 pagesRecombinant Human Vascular Endothelial Growth Factor Enhances Bone Healing in An Experimental Nonunion ModelAnton NopiarNo ratings yet
- Transplantation of Human Placenta-Derived Mesenchymal StemDocument17 pagesTransplantation of Human Placenta-Derived Mesenchymal Stemvirginia.mirandaNo ratings yet
- JHLT Abstract 2019-2Document1 pageJHLT Abstract 2019-2G WNo ratings yet
- Advances in Acute Stroke Treatment 2020Document6 pagesAdvances in Acute Stroke Treatment 2020ayman shomanNo ratings yet
- Apoptosis Post Microwave Ablation of The Liver: Does It Change With Power?Document6 pagesApoptosis Post Microwave Ablation of The Liver: Does It Change With Power?asclepiuspdfsNo ratings yet
- Intervesnsi Stroke 1Document9 pagesIntervesnsi Stroke 1Zilbran BerontaxNo ratings yet
- A Simple and Fast Experimental Model: Laboratory InvestigationDocument4 pagesA Simple and Fast Experimental Model: Laboratory InvestigationAjay PeddiNo ratings yet
- Crocin Attenuates Oxidative Stress and Myocardial Infarction Injury in RatsDocument7 pagesCrocin Attenuates Oxidative Stress and Myocardial Infarction Injury in RatsAdrian BratuNo ratings yet
- JurnalDocument9 pagesJurnalSiscaNo ratings yet
- Midterm Results of Mitral Valve Repair With Homemade Annuloplasty RingsDocument4 pagesMidterm Results of Mitral Valve Repair With Homemade Annuloplasty Ringsadel husseinNo ratings yet
- Chiu 2006Document8 pagesChiu 2006r esspNo ratings yet
- Arrhythmogenic Right Ventricular Cardiomyopathy in A WeimaranerDocument5 pagesArrhythmogenic Right Ventricular Cardiomyopathy in A WeimaranerEmilia AmmariNo ratings yet
- Ehx493 P5438Document1 pageEhx493 P5438Anonymous NeRC5JYiSNo ratings yet
- Veterinary Medicine Today ECG of The MonthDocument4 pagesVeterinary Medicine Today ECG of The Monthabc defNo ratings yet
- Tenecteplase in StrokeDocument10 pagesTenecteplase in StrokeJorge BarriosNo ratings yet
- Tendinitis Crónica Articulo en InglesDocument6 pagesTendinitis Crónica Articulo en IngleskarolndNo ratings yet
- Effect of Pneumatic Tubing System Transport On Platelet Apheresis UnitsDocument13 pagesEffect of Pneumatic Tubing System Transport On Platelet Apheresis Unitsrizka widyanaNo ratings yet
- Conclusion: Long-Term Follow-Up ForDocument31 pagesConclusion: Long-Term Follow-Up ForHima HuNo ratings yet
- Araszkiewicz Et Al. - 2014 - Postconditioning Reduces Enzymatic Infarct Size and Improves Microvascular Reperfusion in Patients With STDocument8 pagesAraszkiewicz Et Al. - 2014 - Postconditioning Reduces Enzymatic Infarct Size and Improves Microvascular Reperfusion in Patients With STscribd mendeleyNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- Fast Two-Photon in Vivo Imaging With Three-Dimensional Random-Access Scanning in Large Tissue VolumesDocument11 pagesFast Two-Photon in Vivo Imaging With Three-Dimensional Random-Access Scanning in Large Tissue Volumesiulia andreeaNo ratings yet
- Eliasmith2012-Large-Scale Model of The Brain-SupplDocument38 pagesEliasmith2012-Large-Scale Model of The Brain-Suppliulia andreeaNo ratings yet
- Sylwestrak2012 Elfn1Document6 pagesSylwestrak2012 Elfn1iulia andreeaNo ratings yet
- Science 2012 Machens Building The Human BrainDocument3 pagesScience 2012 Machens Building The Human Brainiulia andreeaNo ratings yet
- Miller2012 Braqin TeasersDocument1 pageMiller2012 Braqin Teasersiulia andreeaNo ratings yet
- Transcriptome and Epigenome Landscape of Human Cortical Development Modeled in OrganoidsDocument11 pagesTranscriptome and Epigenome Landscape of Human Cortical Development Modeled in Organoidsiulia andreeaNo ratings yet
- Miller2012-Why Is Mental Ilness So Hard To TreatDocument2 pagesMiller2012-Why Is Mental Ilness So Hard To Treatiulia andreeaNo ratings yet
- McBain2012-Decoding The Neuronal Tower of BabelDocument3 pagesMcBain2012-Decoding The Neuronal Tower of Babeliulia andreeaNo ratings yet
- Vogel2012-Can We Make Our Brains More PlasticDocument3 pagesVogel2012-Can We Make Our Brains More Plasticiulia andreeaNo ratings yet
- Balter2012-Why Are Our Brains So BigDocument2 pagesBalter2012-Why Are Our Brains So Bigiulia andreeaNo ratings yet
- Leathers&Olson2012-LIP Neurons Encode Cue SalienceDocument5 pagesLeathers&Olson2012-LIP Neurons Encode Cue Salienceiulia andreeaNo ratings yet
- Eisch&Petrik2012-Depression and Hippocampal NeurogenesisDocument5 pagesEisch&Petrik2012-Depression and Hippocampal Neurogenesisiulia andreeaNo ratings yet
- Stern2012-Defeating The DementorsDocument1 pageStern2012-Defeating The Dementorsiulia andreeaNo ratings yet
- Scheer2006 Caspase InhibitorsDocument6 pagesScheer2006 Caspase Inhibitorsiulia andreeaNo ratings yet
- Wedeen2012-Grid Structure of Brain Pathways-SOMDocument25 pagesWedeen2012-Grid Structure of Brain Pathways-SOMiulia andreeaNo ratings yet
- Karlsson2012-Network Resets in Prefrontal CortexDocument6 pagesKarlsson2012-Network Resets in Prefrontal Cortexiulia andreeaNo ratings yet
- Gerstner2012-Theory and Simulation in NeuroscienceDocument7 pagesGerstner2012-Theory and Simulation in Neuroscienceiulia andreeaNo ratings yet
- Koo2012-BDNF Negative Regulator of Morphin ActionDocument6 pagesKoo2012-BDNF Negative Regulator of Morphin Actioniulia andreeaNo ratings yet
- Tiwari-Woodruff2007-estrogen Recs&ms ModelDocument6 pagesTiwari-Woodruff2007-estrogen Recs&ms Modeliulia andreeaNo ratings yet
- Wang2008-Diploid Genome Sequence of An Asian IndividualDocument7 pagesWang2008-Diploid Genome Sequence of An Asian Individualiulia andreeaNo ratings yet
- Pastalkova2008 SupplDocument28 pagesPastalkova2008 Suppliulia andreeaNo ratings yet
- Baratta2002-Somatostatin LTP Dentate GyrusDocument9 pagesBaratta2002-Somatostatin LTP Dentate Gyrusiulia andreeaNo ratings yet
- Altshuler2008-Genetic Mapping in Human DiseaseDocument9 pagesAltshuler2008-Genetic Mapping in Human Diseaseiulia andreeaNo ratings yet
- BlissDocument7 pagesBlissiulia andreeaNo ratings yet
- Liu2007 Sox17Document7 pagesLiu2007 Sox17iulia andreeaNo ratings yet
- Wang2007 Icaritin NeuroprotectionDocument12 pagesWang2007 Icaritin Neuroprotectioniulia andreeaNo ratings yet
- Knowles2007-Kinetics and Thermodynamics of Amyloid AggregationDocument7 pagesKnowles2007-Kinetics and Thermodynamics of Amyloid Aggregationiulia andreeaNo ratings yet
- Oakes-Mitochondria Ca Immune SynapseDocument2 pagesOakes-Mitochondria Ca Immune Synapseiulia andreeaNo ratings yet
- Schridde2006 IhDocument13 pagesSchridde2006 Ihiulia andreeaNo ratings yet
- Jan1998-Ion Channels & Neurologic DiseaseDocument8 pagesJan1998-Ion Channels & Neurologic Diseaseiulia andreeaNo ratings yet
- 0298-W1403570 NT Dg3002ih Ang 03 03Document299 pages0298-W1403570 NT Dg3002ih Ang 03 03JORGE NAVARRONo ratings yet
- Brugada Syndrome ECGDocument34 pagesBrugada Syndrome ECGMohammad Irfan100% (1)
- ACS LectureDocument55 pagesACS LectureAyunda AlmiradaniNo ratings yet
- Physical Examination of Cardiovascular SystDocument13 pagesPhysical Examination of Cardiovascular Systgamal attamNo ratings yet
- Cardiac Surgery - Postoperative ArrhythmiasDocument9 pagesCardiac Surgery - Postoperative ArrhythmiaswanariaNo ratings yet
- Đề số 29Document5 pagesĐề số 29Mëssënġër Việt NamNo ratings yet
- NN Drip ObatDocument7 pagesNN Drip ObatDioniivanNo ratings yet
- DapusDocument4 pagesDapusAtika DalilaaNo ratings yet
- 2 Anaesthesia TriadDocument2 pages2 Anaesthesia TriadFarrukh Ali KhanNo ratings yet
- Heart AnatomyDocument178 pagesHeart AnatomysubbuNo ratings yet
- Risk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWDocument429 pagesRisk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWRohan Upadhyay UpadhyayNo ratings yet
- Beating Heart Tech Brochure 200701512c - ENDocument6 pagesBeating Heart Tech Brochure 200701512c - ENWinta Sari AprilianaNo ratings yet
- Mending Broken Hearts: by Jennifer Kahn Photograph by Robert ClarkDocument3 pagesMending Broken Hearts: by Jennifer Kahn Photograph by Robert Clarkmonalall0% (1)
- CardiomyopathyDocument9 pagesCardiomyopathyMinh Nguyễn Phương HồngNo ratings yet
- Soca CHF LuhurDocument5 pagesSoca CHF LuhurPradana Nur OviyantiNo ratings yet
- Autopulse Ems Brochure UkDocument5 pagesAutopulse Ems Brochure UkForum PompieriiNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisJohiarra Madanglog TabigneNo ratings yet
- Stoelting Anasthesia and Co Existing Disease PDFDocument28 pagesStoelting Anasthesia and Co Existing Disease PDFEgidia SetyaNo ratings yet
- Nikaidoh Procedure: A Perspective: EditorialDocument5 pagesNikaidoh Procedure: A Perspective: Editorialmihalcea alinNo ratings yet
- Pathologt of The HeartDocument40 pagesPathologt of The HeartJudithNo ratings yet
- Ic Guía Esc 2021-99-128Document30 pagesIc Guía Esc 2021-99-128aassNo ratings yet
- Step by Step Echocardiography in Congenital Heart DiseasesDocument224 pagesStep by Step Echocardiography in Congenital Heart DiseasesEbookStore.DocNo ratings yet
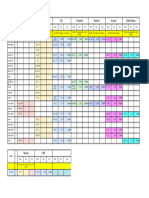
- Time Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICDocument5 pagesTime Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICSheryl ElitaNo ratings yet
- Or-DR Tally FinalDocument1 pageOr-DR Tally FinalMarvinNo ratings yet
- Left Ventricular FailureDocument17 pagesLeft Ventricular Failurenisha24100% (1)