Download as pdf or txt
You might also like
- 6.4 SPIROMETER VIRTUAL LAB - Equipo EGDocument5 pages6.4 SPIROMETER VIRTUAL LAB - Equipo EGAntigua CuentaNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- BRONCHIECTASISDocument40 pagesBRONCHIECTASISImmanuel100% (2)
- Pulmonology MCQsDocument49 pagesPulmonology MCQsaliakbar178100% (1)
- Management of ARDSDocument57 pagesManagement of ARDSRajaNo ratings yet
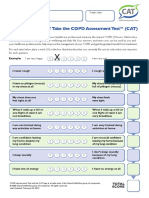
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocument1 pageHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaNo ratings yet
- Acute Respiratory Distress SyndromeDocument43 pagesAcute Respiratory Distress SyndromeAgnes Pritama Fahmi100% (1)
- k12, Pa, Pathology of Copd - rts1-k12Document46 pagesk12, Pa, Pathology of Copd - rts1-k12ashtridNo ratings yet
- BRONCHIECTASISDocument36 pagesBRONCHIECTASISNishanth ReddyNo ratings yet
- COPDDocument70 pagesCOPDDr. Rizwana SamrinNo ratings yet
- Pathology of Airway DiseasesDocument42 pagesPathology of Airway DiseasesZijieNo ratings yet
- Acute & Chronic Bronchitis & COPDDocument49 pagesAcute & Chronic Bronchitis & COPDHendraDarmawanNo ratings yet
- PATHOPHYSIOLOGYDocument46 pagesPATHOPHYSIOLOGYnimrakhalid82000No ratings yet
- Respiratory System DisorderDocument46 pagesRespiratory System DisorderYaniNo ratings yet
- Pulmonary Emphysema: EpidemiologyDocument4 pagesPulmonary Emphysema: EpidemiologyAnonymous 835s2sxNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Clinical and Radiological Evaluation of Emphysematous Chest - A Prospective StudyDocument5 pagesClinical and Radiological Evaluation of Emphysematous Chest - A Prospective StudyTony AndersonNo ratings yet
- Past Year RespiDocument5 pagesPast Year RespiThulasi tootsieNo ratings yet
- Suppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversityDocument65 pagesSuppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversitykingmedicNo ratings yet
- COPDDocument6 pagesCOPDAubrey PerezNo ratings yet
- COPDDocument73 pagesCOPDBroken Oreos100% (1)
- Normal Changes of AgingDocument9 pagesNormal Changes of AgingGiselle EstoquiaNo ratings yet
- PneumothoraxDocument43 pagesPneumothoraxSravani KanchiNo ratings yet
- Case Discussion - CopdDocument63 pagesCase Discussion - CopdrajeshNo ratings yet
- Pulmonary ConditionsDocument42 pagesPulmonary ConditionsMinetteNo ratings yet
- Respiratory Pathology: Dr. Okon MRCSDocument38 pagesRespiratory Pathology: Dr. Okon MRCSEdwin OkonNo ratings yet
- INTERNAL MEDICINEnewDocument22 pagesINTERNAL MEDICINEnewHARPREETNo ratings yet
- RESP MEDICINE For PlabDocument73 pagesRESP MEDICINE For PlabJanie-Vi GorospeNo ratings yet
- BRONCHIECTASISDocument40 pagesBRONCHIECTASISAnujNo ratings yet
- Lung AbscessDocument41 pagesLung AbscessokaciaNo ratings yet
- Pulmonary PathologyDocument46 pagesPulmonary PathologyMuostafa KamelNo ratings yet
- Tina ThankachanDocument50 pagesTina ThankachanBharat JamodNo ratings yet
- Copd Omc Class - BB PDFDocument29 pagesCopd Omc Class - BB PDFafaq alismailiNo ratings yet
- Respiration CH 43.Dr SarahDocument59 pagesRespiration CH 43.Dr Sarahaiman siddiquiNo ratings yet
- BronchiectasisDocument63 pagesBronchiectasisprabad dunusingheNo ratings yet
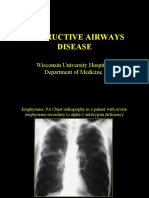
- Obstructive Airways Disease: Wisconsin University Hospital. Department of MedicineDocument27 pagesObstructive Airways Disease: Wisconsin University Hospital. Department of MedicineAlfina Aulia RizkiNo ratings yet
- Emphysema Notes DownloadDocument6 pagesEmphysema Notes DownloadJubitta JobyNo ratings yet
- Patologi KardiopulmonalDocument43 pagesPatologi Kardiopulmonal9661jackNo ratings yet
- Respiratory SystemDocument43 pagesRespiratory SystemMaxxdlc 16No ratings yet
- Case Study PneumoniaDocument13 pagesCase Study Pneumonialavparedes93% (44)
- OSPE UNMANNED STATION - Chest X RayDocument7 pagesOSPE UNMANNED STATION - Chest X Rayshadhana sivakumarNo ratings yet
- PathologyDocument159 pagesPathologyIkram ShinwariNo ratings yet
- 2 - CopdDocument40 pages2 - CopdFathima MulthazimaNo ratings yet
- Cor Pulmonale An Overview 2003Document12 pagesCor Pulmonale An Overview 2003Ade Cahyo IslamiNo ratings yet
- Bronchitis Obliterans Due To Mycoplasma PneumoniaDocument7 pagesBronchitis Obliterans Due To Mycoplasma Pneumoniawawa chenNo ratings yet
- Articulo Parcial 1 Urgencias Respiratorias Perros y GatosDocument23 pagesArticulo Parcial 1 Urgencias Respiratorias Perros y GatosYara Valentina Toledo ManriqueNo ratings yet
- Reespiratory Tract InfectionDocument53 pagesReespiratory Tract InfectionDr. Pawan KumarNo ratings yet
- High Resolution Chest CT (HRCT) : Protocol, Indications, and PathologiesDocument36 pagesHigh Resolution Chest CT (HRCT) : Protocol, Indications, and PathologiesAashishNo ratings yet
- Respiratory Case StudiesDocument6 pagesRespiratory Case Studiesadom09No ratings yet
- Interventions For Critically Ill Patients With Respiratory Problems LectureDocument118 pagesInterventions For Critically Ill Patients With Respiratory Problems LecturedeebertoNo ratings yet
- Fundamental Concepts of Anesthesiology: Dr. Weiwei LiuDocument31 pagesFundamental Concepts of Anesthesiology: Dr. Weiwei Liusimple livingNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Chronic Obstructive Pulmonary Disease: Christine Loren T. Laya BSN 3-1Document41 pagesChronic Obstructive Pulmonary Disease: Christine Loren T. Laya BSN 3-1Kristine CastilloNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Cough & Dyspnea (Initial)Document23 pagesCough & Dyspnea (Initial)Eman BuNo ratings yet
- Resp 180214084710Document72 pagesResp 180214084710Karla Geraldine Carhuas VeliNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric WongDocument7 pagesChronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric Wongjamil aldasriNo ratings yet
- DR Sumardi PPOK - Emfisema-UIIDocument22 pagesDR Sumardi PPOK - Emfisema-UIItrianaamaliaNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Pulmonary Functional Imaging: Basics and Clinical ApplicationsFrom EverandPulmonary Functional Imaging: Basics and Clinical ApplicationsYoshiharu OhnoNo ratings yet
- Health Service Management at Lamjung District HospitalDocument102 pagesHealth Service Management at Lamjung District HospitalShashanka PoudelNo ratings yet
- Do HSDocument97 pagesDo HSShashanka PoudelNo ratings yet
- Anil Municipality Interview GuidelinesDocument9 pagesAnil Municipality Interview GuidelinesShashanka PoudelNo ratings yet
- PHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THDocument6 pagesPHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THShashanka PoudelNo ratings yet
- BiochemistryDocument36 pagesBiochemistryShashanka PoudelNo ratings yet
- AnatomyDocument18 pagesAnatomyShashanka PoudelNo ratings yet
- PathologyDocument32 pagesPathologyShashanka PoudelNo ratings yet
- PhysiologyDocument40 pagesPhysiologyShashanka PoudelNo ratings yet
- AnatomyDocument32 pagesAnatomyShashanka PoudelNo ratings yet
- MicrobiologyDocument50 pagesMicrobiologyShashanka PoudelNo ratings yet
- BiochemistryDocument18 pagesBiochemistryShashanka PoudelNo ratings yet
- Paper I-IV (Past Question)Document22 pagesPaper I-IV (Past Question)Shashanka PoudelNo ratings yet
- PharmacologyDocument26 pagesPharmacologyShashanka PoudelNo ratings yet
- Interstitial Lung DiseaseDocument4 pagesInterstitial Lung DiseasedewimarisNo ratings yet
- AsthmaDocument2 pagesAsthmaZyra AmbaganNo ratings yet
- Bronchial AsthmaDocument40 pagesBronchial Asthmasamson bd mokuntil100% (1)
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDocument8 pagesOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoNo ratings yet
- Ism Interview Assessment 1Document3 pagesIsm Interview Assessment 1api-482594367No ratings yet
- Zab Mohsenifar, Guy W. Soo Hoo Lung Biology in Health & Disease Volume 213 Practical Pulmonary and Critical Care Medicine Respiratory Failure PDFDocument444 pagesZab Mohsenifar, Guy W. Soo Hoo Lung Biology in Health & Disease Volume 213 Practical Pulmonary and Critical Care Medicine Respiratory Failure PDFAnca Dumitru50% (2)
- Mendelson's SyndromeDocument17 pagesMendelson's SyndromeMeena ViswaNo ratings yet
- Ventilation-Perfusion RatioDocument34 pagesVentilation-Perfusion Rationeeba habeebNo ratings yet
- Joshi Abhishek Ashvinbhai S.Y.P.B.B.Sc - Nursing Gov - College of Nursing JamnagarDocument123 pagesJoshi Abhishek Ashvinbhai S.Y.P.B.B.Sc - Nursing Gov - College of Nursing JamnagarKristine C.No ratings yet
- Pews Observation and Escalation Chart 0 11 Months UpdatedDocument1 pagePews Observation and Escalation Chart 0 11 Months Updatedanitn2020No ratings yet
- Lower Respiratory Tract InfectionsDocument14 pagesLower Respiratory Tract InfectionsEric EpahNo ratings yet
- Jadual Respiro 2021Document16 pagesJadual Respiro 2021yayayayayayayaNo ratings yet
- Ketamine Use Allows Non Invasive VentilationDocument2 pagesKetamine Use Allows Non Invasive Ventilationankur vermaNo ratings yet
- Sleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongDocument6 pagesSleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongVijay KumarNo ratings yet
- NCM 112 CopdDocument6 pagesNCM 112 CopdFifaNo ratings yet
- Clinical Approach of Noisy Breathing in Infant and ChildrenDocument40 pagesClinical Approach of Noisy Breathing in Infant and ChildrenAndriana SusantiNo ratings yet
- Basic Clinical Lab Competencies For Respiratory Care 5Th Edition White Test Bank Full Chapter PDFDocument29 pagesBasic Clinical Lab Competencies For Respiratory Care 5Th Edition White Test Bank Full Chapter PDFflorenceronaldoxo0100% (15)
- CPAP ManualDocument43 pagesCPAP ManualTachira Julher RiveraNo ratings yet
- GgoDocument6 pagesGgoAnupam ShrivastavaNo ratings yet
- CuesDocument8 pagesCuesFloyd SevillaNo ratings yet
- Changing Trends in The Decompression of Tension PneumothoraxDocument6 pagesChanging Trends in The Decompression of Tension Pneumothoraxnanang hidayatullohNo ratings yet
- Hospitals and Diagnostic CentreDocument32 pagesHospitals and Diagnostic CentreMurmu BricksNo ratings yet
- Ambu BagDocument12 pagesAmbu BagAejaz Ahmad100% (1)
- Airway Management VentilationDocument13 pagesAirway Management Ventilationmariafer99No ratings yet
- SimvDocument5 pagesSimvUCIADULTO UPEDNo ratings yet
- Focus On VentilationDocument4 pagesFocus On VentilationPablo IgnacioNo ratings yet
- Cardio NoteDocument17 pagesCardio NoteMustak AhmedNo ratings yet