Download as pdf or txt
You might also like
- Practical Text Analytics: Maximizing the Value of Text DataFrom EverandPractical Text Analytics: Maximizing the Value of Text DataNo ratings yet
- Theory Development in NursingDocument15 pagesTheory Development in NursingJules Antonette RNNo ratings yet
- Deep Learning For Database Mapping and Asking Clarification Questions in Dialogue SystemsDocument14 pagesDeep Learning For Database Mapping and Asking Clarification Questions in Dialogue Systemsramesh kumarNo ratings yet
- Summary of ChatGPT Related Research and Perspective Towards TH - 2023 - Meta RadDocument14 pagesSummary of ChatGPT Related Research and Perspective Towards TH - 2023 - Meta RadRiddhesh PatelNo ratings yet
- 2023 Acl-Long 896Document15 pages2023 Acl-Long 896hakim223mohamedabdNo ratings yet
- Cognitive - Analytics - Going Beyond - Big - Data - Analytics - and - Machine - LearningDocument37 pagesCognitive - Analytics - Going Beyond - Big - Data - Analytics - and - Machine - Learningritu kumbhaniNo ratings yet
- 2023 Eacl-Main 107Document14 pages2023 Eacl-Main 107bosheng dingNo ratings yet
- CNN LSTM Hybrid Approach For Sentiment AnalysisDocument14 pagesCNN LSTM Hybrid Approach For Sentiment AnalysisIJRASETPublicationsNo ratings yet
- JCM 12 05410Document12 pagesJCM 12 05410koNo ratings yet
- Exploring The Limits of Chatgpt For Query or Aspect-Based Text SummarizationDocument9 pagesExploring The Limits of Chatgpt For Query or Aspect-Based Text SummarizationIsmail NajimNo ratings yet
- Internet-Based Brain Training Games, Citizen Scientists, and Big Data Ethical Issues in Unprecedented Virtual TerritoriesDocument4 pagesInternet-Based Brain Training Games, Citizen Scientists, and Big Data Ethical Issues in Unprecedented Virtual TerritoriesManal ChennoufNo ratings yet
- Expert Systems With ApplicationsDocument13 pagesExpert Systems With ApplicationsMuhammad Junaid AliNo ratings yet
- Tugas Resume Pustiknas ICT4MDocument4 pagesTugas Resume Pustiknas ICT4MdianNo ratings yet
- A Quantitative Study of Data in The NLP CommunityDocument7 pagesA Quantitative Study of Data in The NLP CommunityKekukoNo ratings yet
- Ijerph 20 03378Document10 pagesIjerph 20 03378koNo ratings yet
- Chatdoctor: A Medical Chat Model Fine-Tuned On A Large Language Model Meta-Ai (Llama) Using Medical Domain KnowledgeDocument12 pagesChatdoctor: A Medical Chat Model Fine-Tuned On A Large Language Model Meta-Ai (Llama) Using Medical Domain KnowledgelaocheyujieNo ratings yet
- Detecting Protected Health Information With An Incremental Learning Ensemble A Case Study On New Zealand Clinical TextDocument10 pagesDetecting Protected Health Information With An Incremental Learning Ensemble A Case Study On New Zealand Clinical TextDewan Tarikul MannanNo ratings yet
- Bridging Artificial Intelligence in Medicine With Generative Pre-Trained Transformer (GPT) TechnologyDocument6 pagesBridging Artificial Intelligence in Medicine With Generative Pre-Trained Transformer (GPT) Technologycerberus thanatosNo ratings yet
- Mathematics: Survey On Synthetic Data Generation, Evaluation Methods and GansDocument41 pagesMathematics: Survey On Synthetic Data Generation, Evaluation Methods and GansJakub Wojciech WisniewskiNo ratings yet
- Transparency and Accountability in AI Decision Support: Explaining and Visualizing Convolutional Neural Networks For Text InformationDocument35 pagesTransparency and Accountability in AI Decision Support: Explaining and Visualizing Convolutional Neural Networks For Text InformationEmmanuel TizNo ratings yet
- Chatdoctor: A Medical Chat Model Fine-Tuned On Llama Model Using Medical Domain KnowledgeDocument7 pagesChatdoctor: A Medical Chat Model Fine-Tuned On Llama Model Using Medical Domain KnowledgeRizki Taufik Ulil AlbabNo ratings yet
- Exploring Large Language Model For Next Generation of Artificial Intelligence in OphthalmologyDocument9 pagesExploring Large Language Model For Next Generation of Artificial Intelligence in OphthalmologyAndrés QueupumilNo ratings yet
- 2020 - Boulesteix - Intro To Simulation Studies - BMJ OpenDocument11 pages2020 - Boulesteix - Intro To Simulation Studies - BMJ OpenReetika ChoudhuryNo ratings yet
- MVillaBioSepln2010 FinalDocument4 pagesMVillaBioSepln2010 FinalManuel De La VillaNo ratings yet
- Project 5467Document13 pagesProject 5467stephennrobertNo ratings yet
- Final Report 169369314Document11 pagesFinal Report 169369314MSR MSRNo ratings yet
- Machine Learning For Health Services ResearchersDocument8 pagesMachine Learning For Health Services ResearchersFaraz KhanNo ratings yet
- PDC Review2Document23 pagesPDC Review2corote1026No ratings yet
- Modelling Temporal Document Sequences For Clinical ICD CodingDocument10 pagesModelling Temporal Document Sequences For Clinical ICD CodingmarekreiNo ratings yet
- ChatGPT For Healthcare Services An Eme - 2023 - BenchCouncil Transactions On BeDocument11 pagesChatGPT For Healthcare Services An Eme - 2023 - BenchCouncil Transactions On BeRiddhesh Patel100% (1)
- Sean Jordan Synthesis PaperDocument18 pagesSean Jordan Synthesis Paperapi-306603109No ratings yet
- A Systematic Review On Data Scarcity Problem in Deep Learning: Solution and ApplicationsDocument29 pagesA Systematic Review On Data Scarcity Problem in Deep Learning: Solution and Applicationsbosheng dingNo ratings yet
- Algorithms For Rapid Digitzation of PrescriptionsDocument16 pagesAlgorithms For Rapid Digitzation of PrescriptionsATHARVA INAMDARNo ratings yet
- LLM MedicineDocument11 pagesLLM MedicineCindy LNo ratings yet
- Foundation Models For Generalist Medical Artificial IntelligenceDocument7 pagesFoundation Models For Generalist Medical Artificial IntelligenceRehan MunirNo ratings yet
- Literature Review On HmisDocument7 pagesLiterature Review On Hmisea219sww100% (1)
- Cloud Based Medical NLPDocument10 pagesCloud Based Medical NLPsavvy_as_98-1No ratings yet
- A Literature Review in Health Informatics Using Data Mining TechniquesDocument5 pagesA Literature Review in Health Informatics Using Data Mining TechniquesafmzzgidncysunNo ratings yet
- Sharpening The Blade Missing Data Imputation Using Supervised Machine LearningDocument24 pagesSharpening The Blade Missing Data Imputation Using Supervised Machine LearningAditya SaxenaNo ratings yet
- Clinical Text ReviewDocument19 pagesClinical Text ReviewRamKrishna108No ratings yet
- Seminar ReportDocument25 pagesSeminar ReportTejaswiniNo ratings yet
- Chat GPTDocument17 pagesChat GPTTim ReeveNo ratings yet
- A Survey On Data Augmentation For Text ClassificationDocument35 pagesA Survey On Data Augmentation For Text ClassificationNonov UrbiznesNo ratings yet
- Negative Data AugmentationDocument17 pagesNegative Data AugmentationKaykayNo ratings yet
- Exploring The Benefits of Chatgpt in Medical Equipment Maintenance: An Evaluation of PerformanceDocument7 pagesExploring The Benefits of Chatgpt in Medical Equipment Maintenance: An Evaluation of Performancejosiah masukaNo ratings yet
- Predicting Sample Size Required For Classification PerformanceDocument10 pagesPredicting Sample Size Required For Classification PerformanceNelsonNwaucheNo ratings yet
- Combining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachDocument11 pagesCombining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachAbdelkader MEJDOUBNo ratings yet
- Automatic Reports From Spreadsheets: Data Analysis For The Rest of UsDocument2 pagesAutomatic Reports From Spreadsheets: Data Analysis For The Rest of Usprojects eastlinkNo ratings yet
- Artificialintelligence Applicationsfor Workflow, Process Optimizationandpredictive AnalyticsDocument15 pagesArtificialintelligence Applicationsfor Workflow, Process Optimizationandpredictive AnalyticsSantosh Kumar TataNo ratings yet
- 2018 HISISE BigDatavfDocument10 pages2018 HISISE BigDatavfblank anonimNo ratings yet
- Human Activity Recognition Using Inertial Physiological and Environmental Sensors A Comprehensive SurveyDocument21 pagesHuman Activity Recognition Using Inertial Physiological and Environmental Sensors A Comprehensive SurveyducksgomooNo ratings yet
- Types of AnalyticsDocument4 pagesTypes of AnalyticsSaif UllahNo ratings yet
- Stemming Information Retrieval Research PaperDocument8 pagesStemming Information Retrieval Research Papercakvaw0q100% (1)
- Enhancing The Fuzzy Inference System Using Genetic Algorithm For Predicting The Optimum Production of A Scientific Publishing HouseDocument10 pagesEnhancing The Fuzzy Inference System Using Genetic Algorithm For Predicting The Optimum Production of A Scientific Publishing HouseCSIT iaesprimeNo ratings yet
- SSRN Id3981160Document44 pagesSSRN Id3981160hetalpatel259No ratings yet
- (IJCST-V8I6P9) :Y MadhankumarDocument6 pages(IJCST-V8I6P9) :Y MadhankumarEighthSenseGroupNo ratings yet
- The Role of Big Data Analytics in Hospital Management SystemDocument6 pagesThe Role of Big Data Analytics in Hospital Management SystemAsora Yasmin snehaNo ratings yet
- Machine Learning and Big DataDocument17 pagesMachine Learning and Big DataArkabho BiswasNo ratings yet
- International Journal of Advanced Trends in Computer Science and EngineeringDocument8 pagesInternational Journal of Advanced Trends in Computer Science and EngineeringLokesh AnandanNo ratings yet
- Applications of Artificial Intelligence in Supply Chain Management and Logistics: Focusing Onto Recognition For Supply Chain ExecutionDocument14 pagesApplications of Artificial Intelligence in Supply Chain Management and Logistics: Focusing Onto Recognition For Supply Chain ExecutionVijay Singh ThakurNo ratings yet
- Information SciencesDocument21 pagesInformation SciencesAnthony Job Rosales LuisNo ratings yet
- MCQs SociologyDocument4 pagesMCQs SociologyMustafa AsifNo ratings yet
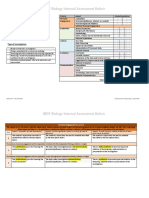
- IBDP Biology Internal Assessment Rubric: Investigation TitleDocument6 pagesIBDP Biology Internal Assessment Rubric: Investigation TitleEman BadryNo ratings yet
- Types of Curriculum Design-3Document7 pagesTypes of Curriculum Design-3Marivic Aguilar Bituin0% (1)
- SpenceDocument224 pagesSpenceGabriela Romanet100% (1)
- Big Data Analytics-SyllabusDocument3 pagesBig Data Analytics-SyllabusDual DaveNo ratings yet
- Divine Light (Akhand Jyoti)Document48 pagesDivine Light (Akhand Jyoti)sksuman100% (13)
- ICMASTS-2024Document2 pagesICMASTS-2024Syed AfwAnNo ratings yet
- 2022 AI Index Report Master (001 060)Document60 pages2022 AI Index Report Master (001 060)Alex ChuquisanaNo ratings yet
- Introduction To PhysicsDocument30 pagesIntroduction To PhysicsRusnizaARNo ratings yet
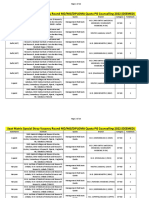
- (DEEMED) Seat Matrix Stray Vacancy Round MD MS DIPDocument26 pages(DEEMED) Seat Matrix Stray Vacancy Round MD MS DIPMinerva Medical Treatment Pvt LtdNo ratings yet
- Module 1 HistoryDocument9 pagesModule 1 HistoryBrendan Lewis DelgadoNo ratings yet
- Hypoth. TestingDocument35 pagesHypoth. TestingRobert Manea100% (1)
- Research Paper K-12Document8 pagesResearch Paper K-12ifqaerbnd100% (1)
- Curriculum S1 S2 PDFDocument7 pagesCurriculum S1 S2 PDFJayan McNo ratings yet
- Concreting of Residential Road Along Sitio SubanaDocument2 pagesConcreting of Residential Road Along Sitio SubanaJoan ZullaNo ratings yet
- घटना चक्र प्राचीन भारत का इतिहास (WWW.UPSCPDF.IN)Document37 pagesघटना चक्र प्राचीन भारत का इतिहास (WWW.UPSCPDF.IN)khanNo ratings yet
- Edplus Online Platform Expectations For 14-15Document2 pagesEdplus Online Platform Expectations For 14-15api-261849620No ratings yet
- Simulación de Movimiento PlanetarioDocument7 pagesSimulación de Movimiento PlanetarioJorgeVNo ratings yet
- Best Practice in Elementary ScienceDocument5 pagesBest Practice in Elementary ScienceJhelai OconNo ratings yet
- Research in Daily Life 2 (HRE 121) - LAP 4 - Week 6-7Document15 pagesResearch in Daily Life 2 (HRE 121) - LAP 4 - Week 6-7Elle KeiNo ratings yet
- Article Xii National Economy and Patrimony SECTION 1. The Goals of The NationalDocument10 pagesArticle Xii National Economy and Patrimony SECTION 1. The Goals of The NationalHazel Martinii PanganibanNo ratings yet
- Assignment / Tugasan HBEC2903 Behaviour Management For Young Children / January 2021 SemesterDocument9 pagesAssignment / Tugasan HBEC2903 Behaviour Management For Young Children / January 2021 SemesterHazlanNo ratings yet
- Literature Review On Rainfall AnalysisDocument7 pagesLiterature Review On Rainfall Analysisafdtuslbb100% (1)
- Dav Public School, Sec-Vi, Cda, Cuttack Book List For The Session: 2023-24 LKGDocument10 pagesDav Public School, Sec-Vi, Cda, Cuttack Book List For The Session: 2023-24 LKGKailash MohantyNo ratings yet
- This Study Resource Was Shared Via: La Consolacion College - IsabelaDocument4 pagesThis Study Resource Was Shared Via: La Consolacion College - IsabelaEddie Agbayani Jr.No ratings yet
- 5 BR Wise TopperDocument32 pages5 BR Wise TopperDollaRaiNo ratings yet
- Investigating Reaction RatesDocument5 pagesInvestigating Reaction RatesAgus SalimNo ratings yet
- Using The HydroFORM For External Corrosion Mapping Using The HydroFORM For External Corrosion MappingDocument1 pageUsing The HydroFORM For External Corrosion Mapping Using The HydroFORM For External Corrosion Mappingpon sharonNo ratings yet
- ScaffDocument26 pagesScaffAnonymous HF5fT2Tw6YNo ratings yet