Download as docx, pdf, or txt
You might also like
- Through The Eyes of The Masters - David AnriasDocument93 pagesThrough The Eyes of The Masters - David Anriasmalazza95% (21)
- Nursing Care Plan 3 Risk For Altered ParentingDocument7 pagesNursing Care Plan 3 Risk For Altered Parentingdbryant010178% (9)
- Madras Miscellany - The Father of Indian Botany - The HinduDocument4 pagesMadras Miscellany - The Father of Indian Botany - The Hindujoseph xavierNo ratings yet
- Pediatric Radiography - Merrills Atlas of Radiographic Positioning and ProceduresDocument61 pagesPediatric Radiography - Merrills Atlas of Radiographic Positioning and ProceduresJonald Pulgo IcoyNo ratings yet
- Chippewa Park Master Plan ReportDocument28 pagesChippewa Park Master Plan ReportinforumdocsNo ratings yet
- Children For SurgeryDocument7 pagesChildren For SurgeryHany ElbarougyNo ratings yet
- UNIT 6 The Nursing Role in Supporting The Health of Ill Children and Their FamiliesDocument5 pagesUNIT 6 The Nursing Role in Supporting The Health of Ill Children and Their FamiliesStephanie LeeNo ratings yet
- Care of Mother and Child at Risk or With Problems (Acute & Chronic) Learning MaterialsDocument13 pagesCare of Mother and Child at Risk or With Problems (Acute & Chronic) Learning Materials3B NOVIDA, ALEYA G.No ratings yet
- Important Considerations in The Initial Clinical Evaluation of The Dysmorphic NeonateDocument5 pagesImportant Considerations in The Initial Clinical Evaluation of The Dysmorphic NeonateKaroo_123No ratings yet
- Contin Educ Anaesth Crit Care Pain-2010-Tan-48-52Document5 pagesContin Educ Anaesth Crit Care Pain-2010-Tan-48-52deadbysunriseeNo ratings yet
- Editorial: Developmental Assessment Tests: Scope and LimitationsDocument5 pagesEditorial: Developmental Assessment Tests: Scope and LimitationsMOON RNo ratings yet
- Pediatric and Geriatric ProceduresDocument9 pagesPediatric and Geriatric ProceduresTeza RizkyNo ratings yet
- CHApter 27 MCN 2023Document76 pagesCHApter 27 MCN 2023Gwen De CastroNo ratings yet
- Wheeling Hospital Nursing Administrative Policy and Procedure Manual Manual Section: Policy Number: Subject: Revision/Review DatesDocument5 pagesWheeling Hospital Nursing Administrative Policy and Procedure Manual Manual Section: Policy Number: Subject: Revision/Review DatesCart Sunrise AguillonNo ratings yet
- Ped 5Document15 pagesPed 5Tufail AhmadNo ratings yet
- MATERNAL and CHILD SUMMARY Chapters 26 - 29 (Adelle Pillitteri)Document87 pagesMATERNAL and CHILD SUMMARY Chapters 26 - 29 (Adelle Pillitteri)CHRISTIE MONTANO100% (8)
- Working With Children in Humanitarian WASH ProgrammesDocument13 pagesWorking With Children in Humanitarian WASH ProgrammesOxfamNo ratings yet
- Wound Care and The Pediatric PatientDocument14 pagesWound Care and The Pediatric PatientFofiuNo ratings yet
- What Is Tummy Time: Is It Necessary For Newborns?: by Joyce Miller, BSC, DC, PHD, and Sharon Vallone, DC, FiccpDocument3 pagesWhat Is Tummy Time: Is It Necessary For Newborns?: by Joyce Miller, BSC, DC, PHD, and Sharon Vallone, DC, FiccpzikmonNo ratings yet
- Paediatric Physiotherapy Involves The AssessmentDocument2 pagesPaediatric Physiotherapy Involves The AssessmentL RNo ratings yet
- The Pediatric PatientDocument21 pagesThe Pediatric PatientrYanDYNo ratings yet
- Neral ConsiderationsDocument13 pagesNeral ConsiderationsNga NguyễnNo ratings yet
- Problem No. 2: Nursing Care of A Family When A Child Needs Diagnostic or Therapeutic ModalitiesDocument20 pagesProblem No. 2: Nursing Care of A Family When A Child Needs Diagnostic or Therapeutic ModalitiesBrandone Dave ParagosoNo ratings yet
- Keys To Enhancing Brain Development in Young Children: January 2005Document9 pagesKeys To Enhancing Brain Development in Young Children: January 2005Arun KamalNo ratings yet
- Sample ChapterDocument11 pagesSample ChapterTales SoNo ratings yet
- Responding and Identifying To Developmental Delay in ChildrenDocument13 pagesResponding and Identifying To Developmental Delay in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Abstract Leaves PowerPoint TemplateDocument29 pagesAbstract Leaves PowerPoint TemplateshafiraNo ratings yet
- Infancy 878Document119 pagesInfancy 878Jela AgengaNo ratings yet
- Diagnóstico de PC en Niños A TérminoDocument6 pagesDiagnóstico de PC en Niños A TérminoarapontepuNo ratings yet
- Terjemahan Developmental CareDocument7 pagesTerjemahan Developmental Carenisaa 2000No ratings yet
- Pastel Pink Brown Simple Group Project PresentationDocument36 pagesPastel Pink Brown Simple Group Project PresentationuccmaryjoyignacioNo ratings yet
- Group 1 Written Report 2 1 1Document9 pagesGroup 1 Written Report 2 1 1Jessa Mae OhaoNo ratings yet
- Wrapping and Swaddling Infants: Child Health Nurses' Knowledge, Attitudes and PracticeDocument11 pagesWrapping and Swaddling Infants: Child Health Nurses' Knowledge, Attitudes and PracticeGieh SyafitriNo ratings yet
- Fitzpatrick - S Dermatology in General Medicine 8thDocument42 pagesFitzpatrick - S Dermatology in General Medicine 8thorchitarosadila haryonoNo ratings yet
- Rooming in and KMCDocument10 pagesRooming in and KMCmanish dafdaNo ratings yet
- Case Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)Document15 pagesCase Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)narseya100% (1)
- Autism: Pediatric Diagnosis and TreatmentDocument1 pageAutism: Pediatric Diagnosis and TreatmentVivekNo ratings yet
- Essential-Intrapartum-Newborn-Care (MIDTERMS)Document4 pagesEssential-Intrapartum-Newborn-Care (MIDTERMS)Allyssa Mae GalarioNo ratings yet
- Chapter 13 NCLEX RN ReviewDocument12 pagesChapter 13 NCLEX RN ReviewBrethren Dezi HoweNo ratings yet
- Sensory Processing Challenges in ChildrenDocument7 pagesSensory Processing Challenges in ChildrenAldoNo ratings yet
- Chapter 6 Behavior Management and Conscious Sedation of Pediatric Patients in The Oral Surgery OfficeDocument11 pagesChapter 6 Behavior Management and Conscious Sedation of Pediatric Patients in The Oral Surgery OfficeAhmad AbrorNo ratings yet
- CPG For Assessment of Children and AdolescentsDocument18 pagesCPG For Assessment of Children and AdolescentsSarwar BaigNo ratings yet
- BPS Coronavirus and UK Schools Closures Support and AdviceDocument5 pagesBPS Coronavirus and UK Schools Closures Support and Advicerou brouwnieNo ratings yet
- Novak Et Al., 2019Document6 pagesNovak Et Al., 2019Evelyn HerreraNo ratings yet
- Paeds Clinical Examination BookletDocument46 pagesPaeds Clinical Examination BookletQaphela MinenhleNo ratings yet
- FinalautismbookletDocument10 pagesFinalautismbookletapi-228136529No ratings yet
- Early Intervention: Environmental or Experimental Factors The First 5 Years of LifeDocument55 pagesEarly Intervention: Environmental or Experimental Factors The First 5 Years of Lifeshruti kumar100% (1)
- 448 FullDocument21 pages448 FullSonnymon A. SobrevillaNo ratings yet
- Self Learning Module For Unit 2 Individual As A Client-1Document61 pagesSelf Learning Module For Unit 2 Individual As A Client-1Tamara Kate HalicanNo ratings yet
- File JURNAL-5 3d26b5a6Document4 pagesFile JURNAL-5 3d26b5a6Surya DimastiarNo ratings yet
- Integrate Strategies That Support Diversity and Anti-Bias PerspectivesDocument4 pagesIntegrate Strategies That Support Diversity and Anti-Bias Perspectivesapi-267528958No ratings yet
- EN - TB - Mod6 - Rehabilitation Techniques, Training and Health Care SystemsDocument30 pagesEN - TB - Mod6 - Rehabilitation Techniques, Training and Health Care SystemsΒασίλης ΒασιλείουNo ratings yet
- The Newborn Individualized Developmental Care Als 2011 PDFDocument29 pagesThe Newborn Individualized Developmental Care Als 2011 PDFMediCNNo ratings yet
- 1.8837 Hypoxic Ischaemic Encaphalopathy (HIE)Document2 pages1.8837 Hypoxic Ischaemic Encaphalopathy (HIE)Bia BarridoNo ratings yet
- Basic Life SupportDocument128 pagesBasic Life SupportRadhiatun NisaNo ratings yet
- A New Method in Reminder Therapy Technique For Ceasing Digit Sucking Habit in ChildrenDocument3 pagesA New Method in Reminder Therapy Technique For Ceasing Digit Sucking Habit in ChildrensrinandanNo ratings yet
- Zitelli Development Cap 3Document30 pagesZitelli Development Cap 3Marcela HincapiéNo ratings yet
- Textbook Mcqs in Pediatrics Review of Nelson Textbook of Pediatrics 20Th Edition Zuhair M Almusawi Ebook All Chapter PDFDocument53 pagesTextbook Mcqs in Pediatrics Review of Nelson Textbook of Pediatrics 20Th Edition Zuhair M Almusawi Ebook All Chapter PDFsandra.millican277100% (11)
- PedsinReview EarlyidentificationDocument14 pagesPedsinReview EarlyidentificationPranay PandeyNo ratings yet
- Ni Hms 596642Document29 pagesNi Hms 596642putrideasNo ratings yet
- How Can I Help?: A Teacher's Guide to Early Childhood Behavioral HealthFrom EverandHow Can I Help?: A Teacher's Guide to Early Childhood Behavioral HealthNo ratings yet
- EV EXAM 1 Answer KeyDocument9 pagesEV EXAM 1 Answer KeyRachelle Danya Dela RosaNo ratings yet
- Midfi Patho 2Document8 pagesMidfi Patho 2Rachelle Danya Dela RosaNo ratings yet
- Ev Exam 4Document9 pagesEv Exam 4Rachelle Danya Dela RosaNo ratings yet
- Ultra FinalDocument4 pagesUltra FinalRachelle Danya Dela RosaNo ratings yet
- Script in ContrastDocument7 pagesScript in ContrastRachelle Danya Dela RosaNo ratings yet
- Image Production and Evaluation Property of Diagnostic Imagers NationwideDocument36 pagesImage Production and Evaluation Property of Diagnostic Imagers NationwideRachelle Danya Dela RosaNo ratings yet
- Bedside RadiographyDocument10 pagesBedside RadiographyRachelle Danya Dela RosaNo ratings yet
- CT AssignmentDocument7 pagesCT AssignmentRachelle Danya Dela RosaNo ratings yet
- Mri BoxDocument3 pagesMri BoxRachelle Danya Dela RosaNo ratings yet
- Bedside RadiographyDocument11 pagesBedside RadiographyRachelle Danya Dela RosaNo ratings yet
- GuideDocument3 pagesGuideRachelle Danya Dela RosaNo ratings yet
- Sona ReactionDocument2 pagesSona ReactionRachelle Danya Dela RosaNo ratings yet
- Bloody War With Japanese InvadersDocument3 pagesBloody War With Japanese InvadersRachelle Danya Dela RosaNo ratings yet
- Sensorimotor Training A Global Approach For BalancDocument9 pagesSensorimotor Training A Global Approach For BalancVizaNo ratings yet
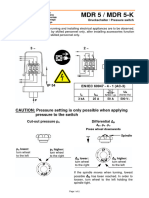
- Pressure Switch MDR5Document4 pagesPressure Switch MDR5Fidelis NdanoNo ratings yet
- Deluge Valve Installation ManualDocument7 pagesDeluge Valve Installation Manualrahull.miishraNo ratings yet
- '21.8월 논문게재 윤인복Document10 pages'21.8월 논문게재 윤인복윤인복No ratings yet
- Creator Excerpt PsycanicsDocument40 pagesCreator Excerpt Psycanicscheshirecatz348No ratings yet
- The Wall Street Journal - Vol. 277 No. 075 (01 Apr 2021)Document32 pagesThe Wall Street Journal - Vol. 277 No. 075 (01 Apr 2021)Andrei StrăchinescuNo ratings yet
- SM - 9 Automatic TransmissionDocument61 pagesSM - 9 Automatic TransmissionJoeNo ratings yet
- Perculse Rubber Manufacturing Industry - Salem Indroduction About Internship TrainingDocument47 pagesPerculse Rubber Manufacturing Industry - Salem Indroduction About Internship Trainingk eswariNo ratings yet
- Al Handal Contracting Company ProfileDocument20 pagesAl Handal Contracting Company Profilerecca23267% (3)
- Helicopter SafetyDocument11 pagesHelicopter SafetyWilliam Greco100% (2)
- Systems Thinking: Gerald MidgleyDocument11 pagesSystems Thinking: Gerald MidgleyKaligula PiranhaNo ratings yet
- Firearms in America 1600 - 1899Document310 pagesFirearms in America 1600 - 1899Mike100% (3)
- Equivalent Length Calculator - RevADocument10 pagesEquivalent Length Calculator - RevArkrajan1502No ratings yet
- Share SyllabusCHY61Document7 pagesShare SyllabusCHY61Roxanne Mae VillacoraNo ratings yet
- Chapter 15 Hormones & Endocrine Glands - Lecture NotesDocument5 pagesChapter 15 Hormones & Endocrine Glands - Lecture Notesapi-3728508100% (3)
- Brkipm-3017 2Document112 pagesBrkipm-3017 2Adilson PedroNo ratings yet
- Electrical Transmission and DistributionDocument31 pagesElectrical Transmission and DistributionPutri Hanifah SNo ratings yet
- Ray OpticsDocument6 pagesRay OpticsshardaviharphysicsNo ratings yet
- Dơnload A Simple Secret 2nd Edition M Brereton Full ChapterDocument24 pagesDơnload A Simple Secret 2nd Edition M Brereton Full Chapterjsfjarbin100% (4)
- Irjet V3i4441 PDFDocument5 pagesIrjet V3i4441 PDFnisaNo ratings yet
- WCP Nietzsche OnNatureGodEthicsDocument4 pagesWCP Nietzsche OnNatureGodEthicsmasohaNo ratings yet
- 9865 0040 01 Cop 1838+ He+ Mux+ Hux+ BrochureDocument4 pages9865 0040 01 Cop 1838+ He+ Mux+ Hux+ BrochuresofrankxNo ratings yet
- Biological Bases of BehaviorDocument7 pagesBiological Bases of BehaviorSANTHOSH KUMAR T MNo ratings yet
- Huawei FusionSolar Smart PV SolutionDocument32 pagesHuawei FusionSolar Smart PV SolutionJOGmzNo ratings yet
- Variables On Both Sides of EquationsDocument17 pagesVariables On Both Sides of EquationsShatakshi DixitNo ratings yet
- Question Paper - BiologyDocument5 pagesQuestion Paper - BiologyAratrika ChakravartyNo ratings yet
- Acceleration Theory & Business Cycles: Sem Ii - MebeDocument14 pagesAcceleration Theory & Business Cycles: Sem Ii - MebePrabhmeet SethiNo ratings yet