Download as pdf or txt
You might also like
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument41 pagesTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineNo ratings yet
- Homeopathy First Aid RemediesDocument91 pagesHomeopathy First Aid Remedieskasradin4791% (22)
- Colour Atlas of Anatomical Pathology 3rd EditionDocument4 pagesColour Atlas of Anatomical Pathology 3rd EditionAura Nirwana0% (1)
- Cancer - 2000 - LossosDocument7 pagesCancer - 2000 - LossoslathifatulNo ratings yet
- Endothelial Dysfunction, Biomarkers of Renal Function SCDDocument7 pagesEndothelial Dysfunction, Biomarkers of Renal Function SCDAnonymous 9QxPDpNo ratings yet
- colette2016Document9 pagescolette2016marisapramsNo ratings yet
- 83 Siadh2 PDFDocument8 pages83 Siadh2 PDFAnonymous QNYOxtHNo ratings yet
- Frequency and Predictors of Pulmonary Hypertension in Patients With Systemic Lupus ErythematosusDocument4 pagesFrequency and Predictors of Pulmonary Hypertension in Patients With Systemic Lupus ErythematosusAndi WahyudiNo ratings yet
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 pagesAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaNo ratings yet
- Diagnostic Evaluation of A Pleural Effusion in Adults: Initial TestingDocument27 pagesDiagnostic Evaluation of A Pleural Effusion in Adults: Initial TestingaraNo ratings yet
- ArtLinfoma InfolenteDocument5 pagesArtLinfoma InfolenteSamy De La Cruz SánchezNo ratings yet
- Villena 2004Document4 pagesVillena 2004azkaparobiNo ratings yet
- Study of Anemia Among Hemophilia Patients: Original ArticleDocument3 pagesStudy of Anemia Among Hemophilia Patients: Original ArticleyouyouNo ratings yet
- The Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsDocument5 pagesThe Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsSaskiaaNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Diagnostic Accuracy of Lymphoscintigraphy ForDocument4 pagesDiagnostic Accuracy of Lymphoscintigraphy ForMARIA FLAVIA MACEDO PÉREZNo ratings yet
- Hom 3Document7 pagesHom 3Mira SrikandiNo ratings yet
- To Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurDocument9 pagesTo Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurIJAR JOURNALNo ratings yet
- Pulmonary Tuberculosis and Its Haematological Correlates-1Document8 pagesPulmonary Tuberculosis and Its Haematological Correlates-1mentari_64No ratings yet
- Evans Syndrome - A Study of Six Cases With Review of LiteratureDocument6 pagesEvans Syndrome - A Study of Six Cases With Review of Literaturedrrome01No ratings yet
- Primary Hyperaldosteronism (Conn'S Syndrome) Our Results of Laparoscopic Surgical TreatmentDocument4 pagesPrimary Hyperaldosteronism (Conn'S Syndrome) Our Results of Laparoscopic Surgical TreatmentamnaNo ratings yet
- Lieshmeniasis IJPSIDocument3 pagesLieshmeniasis IJPSIdvenumohanNo ratings yet
- Use of Blood Product in SepsisDocument6 pagesUse of Blood Product in SepsisAditya IrawanNo ratings yet
- Activacion Inmune SepsisDocument7 pagesActivacion Inmune SepsisDiana AngelesNo ratings yet
- Pulmonary Hemorrhage in Henoch-Schönlein Purpura: Case Report and Systematic Review of The English LiteratureDocument10 pagesPulmonary Hemorrhage in Henoch-Schönlein Purpura: Case Report and Systematic Review of The English LiteratureIwan MiswarNo ratings yet
- Acute Myeloid Leukemia With Mutated NPM1 Mimics Acute Promyelocytic Leukemia PresentationDocument9 pagesAcute Myeloid Leukemia With Mutated NPM1 Mimics Acute Promyelocytic Leukemia PresentationMunawwar SaukaniNo ratings yet
- Trisomy 12 in CLLDocument6 pagesTrisomy 12 in CLLYanet FrancoNo ratings yet
- Diagnostics 10 01046 v2Document20 pagesDiagnostics 10 01046 v2M Halis HermawanNo ratings yet
- Diagnostic Evaluation of A Pleural Effusion in Adults - Initial Testing - UpToDateDocument27 pagesDiagnostic Evaluation of A Pleural Effusion in Adults - Initial Testing - UpToDateDevi EfrinaNo ratings yet
- Juinjo Abdul MananDocument6 pagesJuinjo Abdul MananMuhammad Hadi ArwaniNo ratings yet
- Hairy Cell Leukemia: A N Unusual Lymphoproliferative DiseaseDocument11 pagesHairy Cell Leukemia: A N Unusual Lymphoproliferative DiseaseMotasem Sirag Mohmmed othmanNo ratings yet
- Hypercalcemia Leukocytosis SyndromeDocument7 pagesHypercalcemia Leukocytosis SyndromeTun MahadankNo ratings yet
- JASN SDHD Paper 2005Document11 pagesJASN SDHD Paper 2005Carlos EghiNo ratings yet
- Low Systemic Vascular ResistanceDocument7 pagesLow Systemic Vascular ResistanceMuhammad BadrushshalihNo ratings yet
- The Clinical Characteristics of Leukopenia in PatiDocument12 pagesThe Clinical Characteristics of Leukopenia in PatipcovarrubiasNo ratings yet
- COVID HematologicparametersDocument8 pagesCOVID HematologicparametersRinny ArdinaNo ratings yet
- Platelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Document6 pagesPlatelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Ahmed MagzoubNo ratings yet
- Seminar: Michael Hallek, Tait D Shanafelt, Barbara EichhorstDocument13 pagesSeminar: Michael Hallek, Tait D Shanafelt, Barbara Eichhorstlengers poworNo ratings yet
- Management of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHDocument10 pagesManagement of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHCarlos Enrique Almonte MarínNo ratings yet
- Diagnostic Evaluation of A Pleural Effusion in Adults: Initial Testing - UpToDateDocument22 pagesDiagnostic Evaluation of A Pleural Effusion in Adults: Initial Testing - UpToDatePaloma GBNo ratings yet
- Lancet-Leucemia Linfocitica CronicaDocument14 pagesLancet-Leucemia Linfocitica CronicaMr. LNo ratings yet
- Hep Chiv Renal DZDocument9 pagesHep Chiv Renal DZSundar RamanathanNo ratings yet
- 260 Ijar-3733Document8 pages260 Ijar-3733kiklikijhyggNo ratings yet
- Clinical Features and Risk Factors of Pancytopenia: A Study in A Tertiary Care HospitalDocument5 pagesClinical Features and Risk Factors of Pancytopenia: A Study in A Tertiary Care HospitalDwitaNo ratings yet
- ANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document7 pagesANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Arv IraNo ratings yet
- Study of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalDocument9 pagesStudy of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Coagulation Dysfunction in Patients With AECOPD and ItsDocument6 pagesCoagulation Dysfunction in Patients With AECOPD and ItsAndreea MoalesNo ratings yet
- A Rare Case of Chronic Lymphocy C Leukaemia With Eosinophilia. Could It Be A Variant of Richter's Transforma On?Document1 pageA Rare Case of Chronic Lymphocy C Leukaemia With Eosinophilia. Could It Be A Variant of Richter's Transforma On?KABILANNo ratings yet
- Cholesterol LDH AdaDocument6 pagesCholesterol LDH AdaIndahNo ratings yet
- Hema 6Document7 pagesHema 6yanuarizkaNo ratings yet
- Jcu 17 127 PDFDocument8 pagesJcu 17 127 PDFRezkyFYNo ratings yet
- Pancytopenia in Children: Etiological ProfileDocument4 pagesPancytopenia in Children: Etiological ProfileHanshel SatriyaNo ratings yet
- 10.1097 01.ccm.0000474847.93776.f4Document2 pages10.1097 01.ccm.0000474847.93776.f4nermeen ahmedNo ratings yet
- Pleural Effusions: The Diagnostic Separation of Transudates and ExudatesDocument8 pagesPleural Effusions: The Diagnostic Separation of Transudates and ExudatesMaría Reynel TarazonaNo ratings yet
- Key Words: Pleural Effusion Peritoneal Effusion Pericardial EffusionDocument11 pagesKey Words: Pleural Effusion Peritoneal Effusion Pericardial EffusionchikaiselaNo ratings yet
- Streptokinase in The Treatment of Pleural Controlled Trial of IntrapleuralDocument7 pagesStreptokinase in The Treatment of Pleural Controlled Trial of IntrapleuraltomgasoneNo ratings yet
- Haemophilia - 2022 - Meijer - Diagnosis of Rare Bleeding DisordersDocument6 pagesHaemophilia - 2022 - Meijer - Diagnosis of Rare Bleeding Disordersyasmineessaheli2001No ratings yet
- Clinical CourseDocument6 pagesClinical CoursePratistha SatyanegaraNo ratings yet
- Up-Regulation of Platelet Activation in Hemophilia ADocument8 pagesUp-Regulation of Platelet Activation in Hemophilia AUtari UbNo ratings yet
- Diagnostic Accuracy of "Pallor" For Detecting Mild and Severe Anaemia in Hospitalized PatientsDocument4 pagesDiagnostic Accuracy of "Pallor" For Detecting Mild and Severe Anaemia in Hospitalized PatientsFrancisco Torres VillagránNo ratings yet
- Arterial Ammonia and Clinical Risk Factors For Encephalopathy and Intracranial Hypertension in Acute Liver FailureDocument9 pagesArterial Ammonia and Clinical Risk Factors For Encephalopathy and Intracranial Hypertension in Acute Liver FailureChannesya TanNo ratings yet
- 1 s2.0 S1578219008703275 MainDocument10 pages1 s2.0 S1578219008703275 Mainavnish sharmaNo ratings yet
- Own Damage-06-Feb-2021 To 05-Feb-2022: Schedule of Premium (Amount in RS.)Document4 pagesOwn Damage-06-Feb-2021 To 05-Feb-2022: Schedule of Premium (Amount in RS.)avnish sharmaNo ratings yet
- Acad Course Btech Phe 2014 15Document6 pagesAcad Course Btech Phe 2014 15avnish sharmaNo ratings yet
- Uin10vj7axowtkkqunsq WDocument1 pageUin10vj7axowtkkqunsq Wavnish sharmaNo ratings yet
- Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument50 pagesDate Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing Balanceavnish sharmaNo ratings yet
- Pi Is 0012369215372330Document7 pagesPi Is 0012369215372330avnish sharmaNo ratings yet
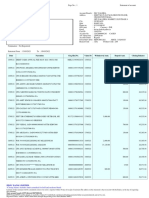
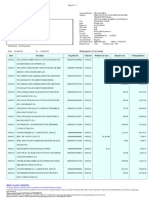
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument11 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing Balanceavnish sharmaNo ratings yet
- C H A L L A N Challan 031-2Document1 pageC H A L L A N Challan 031-2avnish sharmaNo ratings yet
- InvoiceDocument1 pageInvoiceavnish sharmaNo ratings yet
- AB HWC Brochure June 2021 EnglishDocument28 pagesAB HWC Brochure June 2021 EnglishDr. Abhishek OnkarNo ratings yet
- Neurology 40 KochiDocument9 pagesNeurology 40 KochiSrirupa BiswasNo ratings yet
- Gndesitac 4 SMDocument160 pagesGndesitac 4 SMirayoNo ratings yet
- Final Research Bulletin 2014 HEMOGLOBIN WHODocument483 pagesFinal Research Bulletin 2014 HEMOGLOBIN WHOnurul_sharaswatiNo ratings yet
- Bahasa Inggris 3Document9 pagesBahasa Inggris 3vinavzenirNo ratings yet
- Gastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Document11 pagesGastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Giselle Pezoa WattsonNo ratings yet
- FAA Safety NewsletterDocument32 pagesFAA Safety NewsletterHarris DianNo ratings yet
- Medical Books Reference ListDocument6 pagesMedical Books Reference ListKarl CNo ratings yet
- Jurnal 1 PapilitisDocument10 pagesJurnal 1 PapilitisCut Keumala PutriNo ratings yet
- 01 Initial Pages I XxivDocument24 pages01 Initial Pages I XxivJagannathNo ratings yet
- Quantifiable Effects of Osteopathic Manipulative Techniques PDFDocument5 pagesQuantifiable Effects of Osteopathic Manipulative Techniques PDFRodrigo MedinaNo ratings yet
- Bishop Score of PregnancyDocument13 pagesBishop Score of PregnancydrvijeypsgNo ratings yet
- Lactational MastitisDocument2 pagesLactational MastitisMarijosse NavarroNo ratings yet
- RETINOBLASTOMA, DR Claudio Owino, SurgeryDocument30 pagesRETINOBLASTOMA, DR Claudio Owino, SurgeryKaruga NyagahNo ratings yet
- Splenectomy For Hematologic DisordersDocument8 pagesSplenectomy For Hematologic DisordersShofa NisaNo ratings yet
- 2 Normal Oral Cavity Findings and Variants of NormalDocument6 pages2 Normal Oral Cavity Findings and Variants of NormalalbaablyNo ratings yet
- A Silent Revolution in Cancer and AIDSDocument16 pagesA Silent Revolution in Cancer and AIDSUsman MalikNo ratings yet
- Pharmacology BRS - Flash CardsDocument101 pagesPharmacology BRS - Flash Cardsmilap88100% (1)
- Analysis and Quantification of in Wines From Alentejo Region (Portugal)Document6 pagesAnalysis and Quantification of in Wines From Alentejo Region (Portugal)Ivan NikolicNo ratings yet
- Designer Babies PDFDocument12 pagesDesigner Babies PDFAbbie MahinayNo ratings yet
- Crystalloid Fluid Choice and Clinical Outcomes in Pediatric Sepsis J Peds 2017 PDFDocument17 pagesCrystalloid Fluid Choice and Clinical Outcomes in Pediatric Sepsis J Peds 2017 PDFYan Hein TanawaniNo ratings yet
- Sleisenger IndiceDocument4 pagesSleisenger IndiceMario SchettinoNo ratings yet
- Analogue CheeseDocument11 pagesAnalogue CheeseDul Pedroza100% (1)
- Scientific Reasons Behind Indian Traditions - SpeakingtreeDocument14 pagesScientific Reasons Behind Indian Traditions - SpeakingtreeKristina Berg0% (1)
- Profound Ai: For Digital Breast TomosynthesisDocument2 pagesProfound Ai: For Digital Breast TomosynthesisJuanGabrielVillamizarNo ratings yet
- KJ - Ppt..chromosome DefectsDocument84 pagesKJ - Ppt..chromosome DefectsGerald CatiponNo ratings yet
- High Risk Pregnancy - Identification and ManagementDocument24 pagesHigh Risk Pregnancy - Identification and Managementapi-3823785100% (2)
- Flaxseed: A Review of Health BenefitsDocument4 pagesFlaxseed: A Review of Health BenefitsOsman AitaNo ratings yet