Download as pdf or txt
You might also like
- Alcimed - BigPharma Case - Printout 1 - 2021Document6 pagesAlcimed - BigPharma Case - Printout 1 - 2021Arthur WNo ratings yet
- Running Head: CASE STUDY PAPER 1Document14 pagesRunning Head: CASE STUDY PAPER 1Issaiah Nicolle CeciliaNo ratings yet
- Doctor-Scientist On Kangen PDFDocument22 pagesDoctor-Scientist On Kangen PDFfredyagussusanto100% (2)
- Efusi Pleural in MassDocument4 pagesEfusi Pleural in MassRofi IrmanNo ratings yet
- Pylephlebitis Incidentally Found On A Patient With Gastric CancerDocument3 pagesPylephlebitis Incidentally Found On A Patient With Gastric CancerTony NouhNo ratings yet
- 54 Shivraj EtalDocument3 pages54 Shivraj EtaleditorijmrhsNo ratings yet
- Alperovich Et Al. - 2015 - Composite Angioimmunoblastic T-Cell and Diffuse Large B-Cell Lymphoma PDFDocument2 pagesAlperovich Et Al. - 2015 - Composite Angioimmunoblastic T-Cell and Diffuse Large B-Cell Lymphoma PDFflashjetNo ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Pandemic H1N1 Influenza A Viral Infection Complicated by Atypical Hemolytic Uremic Syndrome and Diffuse Alveolar HemorrhageDocument5 pagesPandemic H1N1 Influenza A Viral Infection Complicated by Atypical Hemolytic Uremic Syndrome and Diffuse Alveolar HemorrhageDavidNo ratings yet
- A Case of Recurrent Hemoptysis Caused by Pulmonary Actinomycosis Diagnosed Using Transbronchial Lung Biopsy After Bronchial Artery Embolism and A Brief Review of The LiteratureDocument8 pagesA Case of Recurrent Hemoptysis Caused by Pulmonary Actinomycosis Diagnosed Using Transbronchial Lung Biopsy After Bronchial Artery Embolism and A Brief Review of The LiteratureNiatazya Mumtaz SagitaNo ratings yet
- Abdominal Aortic Aneurysm and Gas in The Kidney inDocument2 pagesAbdominal Aortic Aneurysm and Gas in The Kidney inniluh suwasantiNo ratings yet
- Literature Review of Liver AbscessDocument4 pagesLiterature Review of Liver Abscessc5ng67v1100% (1)
- An Adult Female Presenting With On/off Right Flank Pain For 3 Years, Incidentally, Diagnosed With Primary Renal Lymphoma: A Case ReportDocument4 pagesAn Adult Female Presenting With On/off Right Flank Pain For 3 Years, Incidentally, Diagnosed With Primary Renal Lymphoma: A Case ReportIJAR JOURNALNo ratings yet
- Cytophagic Histiocytic Panniculitis, Hemophagocytic Lymphohistiocytosis and Undetermined Autoimmune Disorder: Reconciling The PuzzleDocument5 pagesCytophagic Histiocytic Panniculitis, Hemophagocytic Lymphohistiocytosis and Undetermined Autoimmune Disorder: Reconciling The PuzzleLe DungNo ratings yet
- ArchIntSurg Adult IntuDocument5 pagesArchIntSurg Adult IntusinghalbmNo ratings yet
- 10 11648 J CRJ 20200802 14Document3 pages10 11648 J CRJ 20200802 14Marj MendezNo ratings yet
- Eosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportDocument5 pagesEosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportSabrina JonesNo ratings yet
- Derrame Pleural 3Document46 pagesDerrame Pleural 3Héctor David GalánNo ratings yet
- Increased Hemoglobin A1c Level Associates With LowDocument8 pagesIncreased Hemoglobin A1c Level Associates With LowNguyễn Tấn PhúNo ratings yet
- Schistosomiasis Case StudyDocument5 pagesSchistosomiasis Case Studyapi-318749549No ratings yet
- Case ReportDocument3 pagesCase Reportyena hillNo ratings yet
- Foldes, D., Et Al. (2020) - Plasmacytoid Lymphocytes in SARS CoV 2 Infection (Covid 19) - American Journal of Hematology PDFDocument2 pagesFoldes, D., Et Al. (2020) - Plasmacytoid Lymphocytes in SARS CoV 2 Infection (Covid 19) - American Journal of Hematology PDFRalt MedNo ratings yet
- Mediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansDocument5 pagesMediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansWahyu RianiNo ratings yet
- Autoimmune Hepatitis: HistopathologyDocument5 pagesAutoimmune Hepatitis: HistopathologyHernan Del CarpioNo ratings yet
- A 56 Year Old Woman With Multiple Pulmonary CystsDocument8 pagesA 56 Year Old Woman With Multiple Pulmonary CystsAchmad Dodi MeidiantoNo ratings yet
- Modern Management of Pyogenic Hepatic Abscess: A Case Series and Review of The LiteratureDocument8 pagesModern Management of Pyogenic Hepatic Abscess: A Case Series and Review of The LiteratureAstari Pratiwi NuhrintamaNo ratings yet
- The Value of Pleural Fluid Analysis: Steven A. Sahn, MDDocument9 pagesThe Value of Pleural Fluid Analysis: Steven A. Sahn, MDCesart LlerenaNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- The Influence of Spleen On Portal HemodynamicsDocument1 pageThe Influence of Spleen On Portal HemodynamicsdenisegmeloNo ratings yet
- Abdominal Lymphadenopathy - Hypothesize Cat-Scratch Disease and Avoid Abdominal Excisional BiopsyDocument8 pagesAbdominal Lymphadenopathy - Hypothesize Cat-Scratch Disease and Avoid Abdominal Excisional BiopsyСергей СадовниковNo ratings yet
- Coll U 2018 DiagnoseDocument4 pagesColl U 2018 DiagnosevisiniNo ratings yet
- 2015 Article 79Document6 pages2015 Article 79Alfeus GradyNo ratings yet
- Nefrita Lupica Care Mimeaza Nefropatie Asociata Virus CDocument5 pagesNefrita Lupica Care Mimeaza Nefropatie Asociata Virus CdeliaNo ratings yet
- Pancytopenia Secondary To Bacterial SepsisDocument16 pagesPancytopenia Secondary To Bacterial Sepsisiamralph89No ratings yet
- Respiratory Medicine Case Reports: Lauryn A. Benninger, Julia A. Ross, Marino E. Leon, Raju Reddy TDocument5 pagesRespiratory Medicine Case Reports: Lauryn A. Benninger, Julia A. Ross, Marino E. Leon, Raju Reddy TAuliaNo ratings yet
- 61a Woman LES N Chest PainDocument6 pages61a Woman LES N Chest PainGabriel MouraNo ratings yet
- Case Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDocument4 pagesCase Report: A Case Report of Peritoneal Tuberculosis: A Challenging DiagnosisDumitru RadulescuNo ratings yet
- Fulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportDocument4 pagesFulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportrahNo ratings yet
- Attending Pleural Effusion ModuleDocument6 pagesAttending Pleural Effusion ModuleMayank MauryaNo ratings yet
- Alveolar Hemorrhage in Systemic Lupus Erythematosus: An OverviewDocument11 pagesAlveolar Hemorrhage in Systemic Lupus Erythematosus: An OverviewHaider AlshomraniNo ratings yet
- Case 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsDocument7 pagesCase 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsJoshua MendozaNo ratings yet
- Hepatic HydrothoraxDocument14 pagesHepatic HydrothoraxIt's MeNo ratings yet
- Hyponatremia and Anti-Diuretic Hormone in Legionnaires ' DiseaseDocument9 pagesHyponatremia and Anti-Diuretic Hormone in Legionnaires ' DiseasejuanpbagurNo ratings yet
- JTD 06 06 E77Document4 pagesJTD 06 06 E77jamieNo ratings yet
- Crim Em2013-948071Document2 pagesCrim Em2013-948071m.fahimsharifiNo ratings yet
- Trousseau's Syndrome in CholangiocarcinomaDocument7 pagesTrousseau's Syndrome in CholangiocarcinomaAnna MariaNo ratings yet
- Pulmonary Hemorrhage in Henoch-Schönlein Purpura: Case Report and Systematic Review of The English LiteratureDocument10 pagesPulmonary Hemorrhage in Henoch-Schönlein Purpura: Case Report and Systematic Review of The English LiteratureIwan MiswarNo ratings yet
- BlablaDocument3 pagesBlablaRosdiana Elizabeth SiburianNo ratings yet
- An Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystDocument3 pagesAn Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystAgus PrimaNo ratings yet
- Multiple Cavitary Lung Lesions in An Adolescent - Case Report of A Rare Presentation of Nodular Lymphocyte Predominant Hodgkin LymphomaDocument4 pagesMultiple Cavitary Lung Lesions in An Adolescent - Case Report of A Rare Presentation of Nodular Lymphocyte Predominant Hodgkin LymphomaManisha UppalNo ratings yet
- Diffuse Large B-Cell Lymphoma Arising From The Lesion ofDocument7 pagesDiffuse Large B-Cell Lymphoma Arising From The Lesion ofFadel AhmadNo ratings yet
- Hepatocellular Carcinoma Causing Severe.1057Document1 pageHepatocellular Carcinoma Causing Severe.1057Vardan KocharNo ratings yet
- Al-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Document6 pagesAl-Azhar Assiut Medical Journal Aamj, Vol 13, No 4, October 2015 Suppl-2Vincentius Michael WilliantoNo ratings yet
- Case PresentationDocument42 pagesCase Presentationjose henaoNo ratings yet
- David S. Raiford Amebic Vs Pyogenic AbscessDocument4 pagesDavid S. Raiford Amebic Vs Pyogenic AbscessyanteeeNo ratings yet
- Pi Is 0168827803002356Document2 pagesPi Is 0168827803002356JeanetteNo ratings yet
- Absceso HepaticoDocument10 pagesAbsceso HepaticoDiego Rodríguez VerdugoNo ratings yet
- Blood Conservation in Pediatric Cardiac SurgeryDocument5 pagesBlood Conservation in Pediatric Cardiac Surgerymohanakrishna007No ratings yet
- Spontaneous Mediastinal Hemorrhage in A Patient With End Stage Renal Disease: An Unusual Case of Uremic BleedingDocument5 pagesSpontaneous Mediastinal Hemorrhage in A Patient With End Stage Renal Disease: An Unusual Case of Uremic BleedingFoscamNo ratings yet
- Hepatic AbscessDocument3 pagesHepatic AbscessbsonNo ratings yet
- Hepatic AbscessDocument3 pagesHepatic AbscessbsonNo ratings yet
- 1 s2.0 S1578219008703275 MainDocument10 pages1 s2.0 S1578219008703275 Mainavnish sharmaNo ratings yet
- Own Damage-06-Feb-2021 To 05-Feb-2022: Schedule of Premium (Amount in RS.)Document4 pagesOwn Damage-06-Feb-2021 To 05-Feb-2022: Schedule of Premium (Amount in RS.)avnish sharmaNo ratings yet
- Acad Course Btech Phe 2014 15Document6 pagesAcad Course Btech Phe 2014 15avnish sharmaNo ratings yet
- Uin10vj7axowtkkqunsq WDocument1 pageUin10vj7axowtkkqunsq Wavnish sharmaNo ratings yet
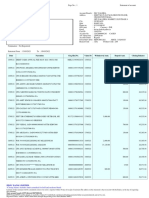
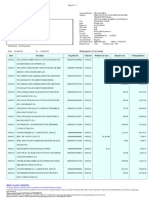
- Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument50 pagesDate Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing Balanceavnish sharmaNo ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument11 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing Balanceavnish sharmaNo ratings yet
- InvoiceDocument1 pageInvoiceavnish sharmaNo ratings yet
- Pi Is 0954611199903153Document4 pagesPi Is 0954611199903153avnish sharmaNo ratings yet
- C H A L L A N Challan 031-2Document1 pageC H A L L A N Challan 031-2avnish sharmaNo ratings yet
- ReovirusesDocument1 pageReoviruseshasna muhadzibNo ratings yet
- Available Online Through: International Journal of Pharmaceutical Archive-2 (3), 2013Document10 pagesAvailable Online Through: International Journal of Pharmaceutical Archive-2 (3), 2013Beladiena Citra Siregar100% (1)
- Scheme of Work Grade 9 2023Document2 pagesScheme of Work Grade 9 2023ramloghun veerNo ratings yet
- Pulmonary Tuberculosis - Curitana BSN 2bDocument10 pagesPulmonary Tuberculosis - Curitana BSN 2bDrex CuritanaNo ratings yet
- Clinical Protocol in Pediatrics, 2012Document96 pagesClinical Protocol in Pediatrics, 2012floare de colt100% (1)
- Inserto Anti RNP SM OrgentecDocument4 pagesInserto Anti RNP SM OrgentecSantiagoAFNo ratings yet
- Rheumatoid Factor Latex Test PartolanDocument15 pagesRheumatoid Factor Latex Test Partolanchocoholic potchiNo ratings yet
- Product Report GarlicDocument81 pagesProduct Report GarlicJilani HussainNo ratings yet
- Teaching Orgasm For Females With Chronic Anorgasmia Using The Betty Dodson MethodDocument14 pagesTeaching Orgasm For Females With Chronic Anorgasmia Using The Betty Dodson MethodAntares1973100% (1)
- Cardiovascular ImagingDocument401 pagesCardiovascular ImagingRani Mulia100% (5)
- Pharmacology Answer Key PINK PACOP 2005Document48 pagesPharmacology Answer Key PINK PACOP 2005Shane KimNo ratings yet
- Final PDFDocument16 pagesFinal PDFVijay Kumar MahanthNo ratings yet
- Knowledge On Infertility Among People at Gairigaun, Tokha - 9Document45 pagesKnowledge On Infertility Among People at Gairigaun, Tokha - 9shiva sharmaNo ratings yet
- China GB 4789.1 2010 National Food Safety Standard Food Microbiological Examination General GuidelDocument7 pagesChina GB 4789.1 2010 National Food Safety Standard Food Microbiological Examination General Guidelmmoradi55No ratings yet
- Pathophysiology of Body Fluids and Fluid TherapyDocument3 pagesPathophysiology of Body Fluids and Fluid TherapybookwormMDNo ratings yet
- Cracking NewSAT 2016 PT6Document62 pagesCracking NewSAT 2016 PT6Anonymous 4cJj6pNo ratings yet
- Normal Laboratory ValuesDocument8 pagesNormal Laboratory ValuesStephanieNo ratings yet
- Autism Spectrum Disorder (ASD) in Girls. Co-Occurring Psychopathology. Sex Differences in Clinical ManifestationDocument11 pagesAutism Spectrum Disorder (ASD) in Girls. Co-Occurring Psychopathology. Sex Differences in Clinical ManifestationRania shafiraNo ratings yet
- Impact of Mindfulness Katherine WeareDocument12 pagesImpact of Mindfulness Katherine WeareMeek El100% (1)
- Wesleyan University-Philippines College of Nursing A.Y. 2022-2023Document30 pagesWesleyan University-Philippines College of Nursing A.Y. 2022-2023Jasmin DaclagNo ratings yet
- Immunological Lab Diagnosis of TuberculosisDocument38 pagesImmunological Lab Diagnosis of TuberculosisRasha EmadNo ratings yet
- TZ-ModularOT - Operating RoomDocument61 pagesTZ-ModularOT - Operating RoomSeni BinaNo ratings yet
- B.SC - Nursing 1st Year PDFDocument9 pagesB.SC - Nursing 1st Year PDFSunita RaniNo ratings yet
- Hifu and Liposunix Combine MachineDocument29 pagesHifu and Liposunix Combine MachineAnisia StefanNo ratings yet
- JHHHJDocument23 pagesJHHHJMoath Zorqan100% (3)
- "Pounds and Inches" For More DetailsDocument89 pages"Pounds and Inches" For More DetailsManu0301No ratings yet
- Discover Your DietDocument51 pagesDiscover Your DietAkanksha SinghNo ratings yet
- Schizophrenia NotesDocument10 pagesSchizophrenia NotesJamesNo ratings yet