Download as pdf or txt
You might also like
- DTDC ReportDocument30 pagesDTDC ReportSujit_tdNo ratings yet
- Psychotropic Drugs: Bryan Mae H. DegorioDocument65 pagesPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Neurotransmitters AnxietyDocument7 pagesNeurotransmitters AnxietyMatthew SyNo ratings yet
- Module 4: Neurologic Medications: TasksDocument5 pagesModule 4: Neurologic Medications: TasksSheril Marek0% (1)
- CNS Depressants - Anxiolytics & Sedative HypnoticsDocument4 pagesCNS Depressants - Anxiolytics & Sedative HypnoticsJustin HulinNo ratings yet
- PsychotropicsDocument4 pagesPsychotropicsGeoffrey KernsNo ratings yet
- PsychiatryDocument5 pagesPsychiatryJohn SmithNo ratings yet
- AnxietyDocument4 pagesAnxietyIT’S ME HAYLANo ratings yet
- Anxiety Disorders 2Document3 pagesAnxiety Disorders 2nursekatieNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
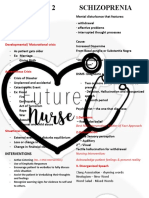
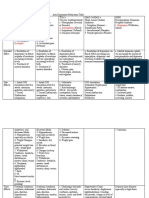
- Day 2 - SchizophreniaDocument4 pagesDay 2 - SchizophreniaVictoria Castillo TamayoNo ratings yet
- Psych NotesDocument3 pagesPsych NotesJuvy Mae NalzaroNo ratings yet
- Drug Study, Olanzapine, Kalium Durule, AripiprazoleDocument7 pagesDrug Study, Olanzapine, Kalium Durule, Aripiprazoleroshannevergara0777No ratings yet
- Phobias-SchizophreniaDocument5 pagesPhobias-SchizophreniaAud SyneNo ratings yet
- Table of Sedative, Hypnotic, AntianxietyDocument4 pagesTable of Sedative, Hypnotic, AntianxietyirfanzukriNo ratings yet
- PsychopharmacologyDocument5 pagesPsychopharmacologyADAL, KATE CARMELANo ratings yet
- 2018-2019 Cns DepressantsDocument5 pages2018-2019 Cns DepressantsMary AgorillaNo ratings yet
- Skeletal Muscle RelaxantsDocument2 pagesSkeletal Muscle RelaxantsRachel Ann FranchescaNo ratings yet
- Psychotherapeutic AgentsDocument2 pagesPsychotherapeutic AgentsjustinahorroNo ratings yet
- Antipsychotic Drugs-1Document5 pagesAntipsychotic Drugs-1Teddy linumbwaNo ratings yet
- Psych 1681444892976Document4 pagesPsych 1681444892976HANNAH BANGKILINGNo ratings yet
- Prozac Venlafaxine Duloxetine Amitriptyline BupropionDocument3 pagesProzac Venlafaxine Duloxetine Amitriptyline BupropionMichael S. PetryNo ratings yet
- PSYCHOPHARMACOLOGY HndoutDocument12 pagesPSYCHOPHARMACOLOGY HndoutMhae TabasaNo ratings yet
- CNS Ta7Document82 pagesCNS Ta7يوسف الشرقاويNo ratings yet
- Depression PDFDocument10 pagesDepression PDFLyadelou FortuNo ratings yet
- PsychePharma 2pagesDocument2 pagesPsychePharma 2pagesBear GrylsNo ratings yet
- Module IV: Central Nervous System MedicationsDocument4 pagesModule IV: Central Nervous System MedicationsVincent Paul SantosNo ratings yet
- Ativan (Lorazepam) Drug StudyDocument3 pagesAtivan (Lorazepam) Drug StudyCHERISE CORDOVA100% (2)
- Of Drug Toxicities Psychiatric Emergencies & Medication Side EffectsDocument8 pagesOf Drug Toxicities Psychiatric Emergencies & Medication Side EffectsBaraa KhalafNo ratings yet
- Psycho MedsDocument3 pagesPsycho Medsdenebrench23No ratings yet
- AnxiolyticsDocument8 pagesAnxiolyticsAlfie16No ratings yet
- Lecture 3Document35 pagesLecture 3Abdelrahman Faiesal MohamedNo ratings yet
- 1 Medicatia SNCDocument29 pages1 Medicatia SNCMiruna-CristianaBirtuNo ratings yet
- Multi-Dimensional Approach To Psychopathology Vlinical Assessment and DiagnosisDocument3 pagesMulti-Dimensional Approach To Psychopathology Vlinical Assessment and Diagnosisrayndennisse759No ratings yet
- Anxiolytic and Hypnotic DrugsDocument3 pagesAnxiolytic and Hypnotic Drugsskoee dbswjNo ratings yet
- TRIAZOLAMDocument4 pagesTRIAZOLAMEzequiel RosalesNo ratings yet
- Psychotropics NotesDocument5 pagesPsychotropics NotesJulianna Rheaven JoreNo ratings yet
- Pharmacology: Reviewer For Final Exam: Nervous SystemDocument18 pagesPharmacology: Reviewer For Final Exam: Nervous Systempatty janeNo ratings yet
- Interventions and Treatments Barlow Durand Ab Psy 7th Ed.Document10 pagesInterventions and Treatments Barlow Durand Ab Psy 7th Ed.Pia ToratoNo ratings yet
- Stereotypical Behavior: Rate Dependence EffectsDocument2 pagesStereotypical Behavior: Rate Dependence EffectsJustin HulinNo ratings yet
- DiazepamDocument1 pageDiazepamGracia Dela CruzNo ratings yet
- Shortnote PsyDocument18 pagesShortnote PsyRasyidah ZakariaNo ratings yet
- PSYCHOPHARMACOLOGYDocument2 pagesPSYCHOPHARMACOLOGYJulia Rae Delos SantosNo ratings yet
- Drug List PsychopharmDocument23 pagesDrug List PsychopharmGeorge HananiaNo ratings yet
- SCHIZOPHRENIA (DX Criteria)Document25 pagesSCHIZOPHRENIA (DX Criteria)Nadhrah ZulkifliNo ratings yet
- Drugs of AbuseDocument3 pagesDrugs of AbuseNovutry SiregarNo ratings yet
- CNS DrugsDocument57 pagesCNS DrugsHussein Al-jmrawiNo ratings yet
- Pharmacology in PsychiatryDocument33 pagesPharmacology in PsychiatryKatrina PonceNo ratings yet
- Drugs Affecting CNSDocument30 pagesDrugs Affecting CNSGwen De CastroNo ratings yet
- Pharmacology IV L5Document4 pagesPharmacology IV L5سلطان القلحNo ratings yet
- Pharmacology of The Central Nervous System-1Document163 pagesPharmacology of The Central Nervous System-1Gølà Sèèñàà–baale irraaNo ratings yet
- Care of Clients With Drugs Affecting The Central and Peripheral Nervous SystemDocument42 pagesCare of Clients With Drugs Affecting The Central and Peripheral Nervous SystemAubrey Justine GaleonNo ratings yet
- Pharmacology Neuromuscular DisordersDocument4 pagesPharmacology Neuromuscular Disorders8dxf5bqv6gNo ratings yet
- MS ReviewerDocument10 pagesMS Reviewermarybeth abelidoNo ratings yet
- Ncmb316 Lec FinalDocument31 pagesNcmb316 Lec FinalDE LEON, CRONICA FAY G.No ratings yet
- ANXIOLYTICS FinalDocument5 pagesANXIOLYTICS FinalErika Blaire N. OlacaoNo ratings yet
- Appendix-B (4) (2068)Document21 pagesAppendix-B (4) (2068)namah odatNo ratings yet
- All Other ClassificationsDocument6 pagesAll Other ClassificationsCorey100% (1)
- Psychotherapy Biomedical Techniques PresentationDocument92 pagesPsychotherapy Biomedical Techniques PresentationRhea Andrea UyNo ratings yet
- Lesson 2.3 Knowledge Check - Pre-CalculusDocument5 pagesLesson 2.3 Knowledge Check - Pre-CalculusNoriko MatsumotoNo ratings yet
- 29 APJABSS Feb BRR797 Social-Sciences-297-306Document10 pages29 APJABSS Feb BRR797 Social-Sciences-297-306Noriko MatsumotoNo ratings yet
- BasCal PETA 1 Ramp Design Guide Question and Peer Evaluation FormatDocument3 pagesBasCal PETA 1 Ramp Design Guide Question and Peer Evaluation FormatNoriko MatsumotoNo ratings yet
- Unit 1, Lesson 4 Study GuideDocument5 pagesUnit 1, Lesson 4 Study GuideNoriko MatsumotoNo ratings yet
- Unit 1, Lesson 2 Study GuideDocument7 pagesUnit 1, Lesson 2 Study GuideNoriko MatsumotoNo ratings yet
- Hipolito WW2.3Document12 pagesHipolito WW2.3Noriko MatsumotoNo ratings yet
- Lesson 1.3 Lets PracticeDocument4 pagesLesson 1.3 Lets PracticeNoriko MatsumotoNo ratings yet
- Study Guide 2.4.1.2 - Angle of Elevation and DepressionDocument5 pagesStudy Guide 2.4.1.2 - Angle of Elevation and DepressionNoriko MatsumotoNo ratings yet
- Lesson 1.4 Lets PracticeDocument2 pagesLesson 1.4 Lets PracticeNoriko MatsumotoNo ratings yet
- Study Guide 2.3 - Graphs of Circular FunctionsDocument17 pagesStudy Guide 2.3 - Graphs of Circular FunctionsNoriko MatsumotoNo ratings yet
- Study Guide 2.4.1.1 - Fundamental Trigonometric IdentitiesDocument5 pagesStudy Guide 2.4.1.1 - Fundamental Trigonometric IdentitiesNoriko MatsumotoNo ratings yet
- Module 2 - Discrete Probability DistributionDocument7 pagesModule 2 - Discrete Probability DistributionNoriko MatsumotoNo ratings yet
- Ans HandoutsDocument6 pagesAns HandoutsNoriko MatsumotoNo ratings yet
- L2 - Prokaryotic Eukaryotic CellhgfhfgDocument65 pagesL2 - Prokaryotic Eukaryotic CellhgfhfgNoriko MatsumotoNo ratings yet
- Module 3 - Standard Normal DistributionDocument13 pagesModule 3 - Standard Normal DistributionNoriko MatsumotoNo ratings yet
- CNSDocument102 pagesCNSNoriko MatsumotoNo ratings yet
- Halo On Bright Objects) ArrhythmiaDocument9 pagesHalo On Bright Objects) ArrhythmiaNoriko MatsumotoNo ratings yet
- L1 - Basic Cell Principles and Cell TheoryDocument37 pagesL1 - Basic Cell Principles and Cell TheoryNoriko MatsumotoNo ratings yet
- L1 - Introduction To Biology Part 1Document38 pagesL1 - Introduction To Biology Part 1Noriko MatsumotoNo ratings yet
- Module 1 - Random VariablesDocument4 pagesModule 1 - Random VariablesNoriko MatsumotoNo ratings yet
- BasCal PETA 1 Ramp Design SAMPLE OUTPUTDocument5 pagesBasCal PETA 1 Ramp Design SAMPLE OUTPUTNoriko MatsumotoNo ratings yet
- Student Registration and Assessment Form (S.Y. 2022-2023)Document1 pageStudent Registration and Assessment Form (S.Y. 2022-2023)Noriko MatsumotoNo ratings yet
- Authorization LetterDocument1 pageAuthorization LetterNoriko MatsumotoNo ratings yet
- 25 Nonfiction Passages With Vocab Build'g CrosswordsDocument65 pages25 Nonfiction Passages With Vocab Build'g Crosswordsvsroilgas78% (9)
- The Victim's Autopsy ReportDocument2 pagesThe Victim's Autopsy ReportShan KNo ratings yet
- Managing Clean Core For SAP S4HANA Cloud NotesDocument59 pagesManaging Clean Core For SAP S4HANA Cloud NotesGLEN KGATLANo ratings yet
- Iii FinalDocument22 pagesIii FinalYu RiNo ratings yet
- Repair Appx V3Document18 pagesRepair Appx V3soniaNo ratings yet
- CHN Transes Week 1Document5 pagesCHN Transes Week 1cheskalyka.asiloNo ratings yet
- Sulh On Maintenance of WifeDocument20 pagesSulh On Maintenance of WifeNurulatika Lasiman100% (1)
- Roger Bacon Resume Nov2020Document1 pageRoger Bacon Resume Nov2020api-232293986No ratings yet
- 1.5 Introducing Petty Cash Books: Suggested ActivitiesDocument2 pages1.5 Introducing Petty Cash Books: Suggested ActivitiesDonatien Oulaii100% (2)
- Labor UnionDocument16 pagesLabor UnionRZ RosalNo ratings yet
- Engineering Economy ProblemsDocument19 pagesEngineering Economy ProblemsEmperor VallenNo ratings yet
- AMS4029MDocument5 pagesAMS4029M黄当甲No ratings yet
- S Bing 0605175 Chapter4Document29 pagesS Bing 0605175 Chapter4Rose GreenNo ratings yet
- Underwood C. P., "HVAC Control Systems, Modelling Analysis and Design" RoutledgeDocument2 pagesUnderwood C. P., "HVAC Control Systems, Modelling Analysis and Design" Routledgeatif shaikhNo ratings yet
- B Com English 2016Document12 pagesB Com English 2016PRIYANK PATEL67% (3)
- Extrusion Compounding Process For The Development of Eco-Friendly SCG/PP Composite PelletsDocument12 pagesExtrusion Compounding Process For The Development of Eco-Friendly SCG/PP Composite PelletsVirendra RathvaNo ratings yet
- Genrich Altshuller-Innovation Algorithm - TRIZ, Systematic Innovation and Technical Creativity-Technical Innovation Center, Inc. (1999)Document290 pagesGenrich Altshuller-Innovation Algorithm - TRIZ, Systematic Innovation and Technical Creativity-Technical Innovation Center, Inc. (1999)Dendra FebriawanNo ratings yet
- Dan Webb Concealment GradeDocument2 pagesDan Webb Concealment Gradeapi-565691734No ratings yet
- Covid ReportDocument1 pageCovid ReportTV UNITNo ratings yet
- Lesson Exemplar School Grade Level Teacher Learning Area Practical Research 2 Teaching Date Quarter Teaching Time No. of DaysDocument9 pagesLesson Exemplar School Grade Level Teacher Learning Area Practical Research 2 Teaching Date Quarter Teaching Time No. of DaysJovie Bitas DaeloNo ratings yet
- Manual MINITAB ReferenciasDocument168 pagesManual MINITAB ReferenciasAnonymous WRK1qDcNo ratings yet
- Intrinsic Element of Short Story - Litte Joe in Trouble AgainDocument13 pagesIntrinsic Element of Short Story - Litte Joe in Trouble AgainEnrico GiøvanoNo ratings yet
- Information Booklet Awards Day 2012Document16 pagesInformation Booklet Awards Day 2012kartytyNo ratings yet
- Annotated BibliographyDocument4 pagesAnnotated Bibliographyapi-302549909No ratings yet
- Usability Testing Report (ENGLISH Only)Document7 pagesUsability Testing Report (ENGLISH Only)memorphNo ratings yet
- Sean Combs v. All Surface Entertainment, Inc., Cancellation No. 92051490 (T.T.A.B. 2012) (DIRTY MONEY)Document21 pagesSean Combs v. All Surface Entertainment, Inc., Cancellation No. 92051490 (T.T.A.B. 2012) (DIRTY MONEY)Charles E. ColmanNo ratings yet
- Navansha Dasha JaiminiDocument6 pagesNavansha Dasha JaiminiSandhya KadamNo ratings yet
- Part of SpeechDocument163 pagesPart of SpeechHHHHNo ratings yet
- Stolen by The Sinner Russian Torpedo Book 1 Hayley Faiman All ChapterDocument67 pagesStolen by The Sinner Russian Torpedo Book 1 Hayley Faiman All Chapterjoshua.sweat158100% (4)