
ICF Core Sets
ICF Core Sets
You might also like
- Instant Download Ebook PDF Essentials of Health Culture and Diversity Understanding People Reducing Disparities PDF ScribdDocument47 pagesInstant Download Ebook PDF Essentials of Health Culture and Diversity Understanding People Reducing Disparities PDF Scribdjames.nohel84498% (49)
- Opd Task Force Operationalized Psychodynamic Diagnosis OPD 2 - Manual of Diagnosis and Treatment Planning Hogrefe Huber Pub 2007 PDFDocument438 pagesOpd Task Force Operationalized Psychodynamic Diagnosis OPD 2 - Manual of Diagnosis and Treatment Planning Hogrefe Huber Pub 2007 PDFნინა ზედგინიძეNo ratings yet
- Manual MusclelabDocument20 pagesManual MusclelaboscampoNo ratings yet
- Cardio Kick Boxing-1 PDFDocument78 pagesCardio Kick Boxing-1 PDFmarsnetworkNo ratings yet
- Research and Development in Adult Education: Fields and TrendsFrom EverandResearch and Development in Adult Education: Fields and TrendsNo ratings yet
- Introduction For Nurse Leader InterviewDocument4 pagesIntroduction For Nurse Leader Interviewapi-312833369No ratings yet
- Textbook Exploring Protein Structure Principles and Practice Tim Skern Ebook All Chapter PDFDocument53 pagesTextbook Exploring Protein Structure Principles and Practice Tim Skern Ebook All Chapter PDFjustin.mallard475100% (16)
- SCI L2-S5 Expected Outcome GuideDocument23 pagesSCI L2-S5 Expected Outcome Guidejustgio928No ratings yet
- Full Chapter Muscle Revolution Concepts and Recipes For Building Muscle Mass and Force 1St Edition Marco Toigo PDFDocument53 pagesFull Chapter Muscle Revolution Concepts and Recipes For Building Muscle Mass and Force 1St Edition Marco Toigo PDFmatthew.marshall671100% (6)
- Traumatic Brain Injury 1St Edition Stephen Honeybul Angelos G Kolias Online Ebook Texxtbook Full Chapter PDFDocument69 pagesTraumatic Brain Injury 1St Edition Stephen Honeybul Angelos G Kolias Online Ebook Texxtbook Full Chapter PDFtheressafinch614100% (7)
- 3. ACENS학회 - program PDFDocument100 pages3. ACENS학회 - program PDFHanmin ParkNo ratings yet
- Textbook Cortical Development Neural Diversity and Neocortical Organization 1St Edition Hiromi Shimojo Ebook All Chapter PDFDocument53 pagesTextbook Cortical Development Neural Diversity and Neocortical Organization 1St Edition Hiromi Shimojo Ebook All Chapter PDFhelen.reed309100% (13)
- Textbook Life Care Planning and Case Management Handbook Fourth Edition Berens Ebook All Chapter PDFDocument53 pagesTextbook Life Care Planning and Case Management Handbook Fourth Edition Berens Ebook All Chapter PDFbarbara.ritter532100% (14)
- Textbook Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes Irene Comisso Et Al Ebook All Chapter PDFDocument53 pagesTextbook Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes Irene Comisso Et Al Ebook All Chapter PDFashley.burnham607100% (11)
- PDF Topographic Organization of The Pectine Neuropils in Scorpions An Analysis of Chemosensory Afferents and The Projection Pattern in The Central Nervous System Denise Drozd Ebook Full ChapterDocument54 pagesPDF Topographic Organization of The Pectine Neuropils in Scorpions An Analysis of Chemosensory Afferents and The Projection Pattern in The Central Nervous System Denise Drozd Ebook Full Chapterburl.juel661100% (1)
- Neuropsychiatric Disorders - Miyoshi, Koho (2010)Document339 pagesNeuropsychiatric Disorders - Miyoshi, Koho (2010)Ramon MagsaysayNo ratings yet
- Guidelines For The Organizat PDFDocument15 pagesGuidelines For The Organizat PDFAlagappan ThiyagarajanNo ratings yet
- Franck Billmann, Tobias Keck Essentials of Visceral Surgery ForDocument392 pagesFranck Billmann, Tobias Keck Essentials of Visceral Surgery ForOurtching NestorNo ratings yet
- Full Chapter in Vivo Neuropharmacology and Neurophysiology 1St Edition Athineos Philippu Eds PDFDocument34 pagesFull Chapter in Vivo Neuropharmacology and Neurophysiology 1St Edition Athineos Philippu Eds PDFkim.gomez589100% (8)
- Clinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtDocument29 pagesClinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtGlauber Teixeira Ervilha100% (1)
- SOP ExerciseTherapy - e - Eng PDFDocument372 pagesSOP ExerciseTherapy - e - Eng PDFEli WatiNo ratings yet
- 指南手册Document119 pages指南手册HugoNo ratings yet
- A Visual Guide To Clinical Anatomy Oct 19 2020 - 1119708109 - Wiley Blackwell 1St Edition Whitaker Full Chapter PDFDocument70 pagesA Visual Guide To Clinical Anatomy Oct 19 2020 - 1119708109 - Wiley Blackwell 1St Edition Whitaker Full Chapter PDFjayetcoxca100% (9)
- PDF Data and Text Processing For Health and Life Sciences Francisco M Couto Ebook Full ChapterDocument53 pagesPDF Data and Text Processing For Health and Life Sciences Francisco M Couto Ebook Full Chapterjanice.quillen556100% (3)
- Leadership and OSHDocument61 pagesLeadership and OSHShabin ShabiNo ratings yet
- QPBR HandbookDocument120 pagesQPBR HandbookGeetha RajashekharNo ratings yet
- ebook download Neurological Examination. Made Easy 6th Edition Fuller Geraint - eBook PDF all chapterDocument54 pagesebook download Neurological Examination. Made Easy 6th Edition Fuller Geraint - eBook PDF all chapteraidokabajaro100% (3)
- Full Download PDF of Neurological Examination. Made Easy 6th Edition Fuller Geraint - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Neurological Examination. Made Easy 6th Edition Fuller Geraint - Ebook PDF All Chapterokornkisida100% (6)
- Taquicardia SupraventricularDocument69 pagesTaquicardia Supraventricularwindar baqueroNo ratings yet
- ACE PT4th Manual Ch1Document69 pagesACE PT4th Manual Ch1chandramouuli78% (9)
- Full Chapter Musculoskeletal Imaging A Survival Manual 1St Edition Plotkin PDFDocument53 pagesFull Chapter Musculoskeletal Imaging A Survival Manual 1St Edition Plotkin PDFjohn.miller951100% (9)
- Leadership and Occupational Safety and Health (OSH) : An Expert AnalysisDocument62 pagesLeadership and Occupational Safety and Health (OSH) : An Expert Analysishuu nguyen nguyenNo ratings yet
- Musculoskeletal Injections Manual - Basics, Techniques and Injectable Agents (Apr 25, 2024) - (3031526023) - (Springer) 1st Edition Baris KocaogluDocument54 pagesMusculoskeletal Injections Manual - Basics, Techniques and Injectable Agents (Apr 25, 2024) - (3031526023) - (Springer) 1st Edition Baris Kocaoglujohn.miller951100% (7)
- Authors:: Sports Physiotherapy Competencies and StandardsDocument78 pagesAuthors:: Sports Physiotherapy Competencies and Standards杨钦杰No ratings yet
- Culture Assessment Soar enDocument79 pagesCulture Assessment Soar enHrishikesh PNo ratings yet
- 2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaDocument3 pages2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaBuya TaftaNo ratings yet
- Job Seeker's Workbook - JISTDocument81 pagesJob Seeker's Workbook - JISTteewako100% (1)
- Add Neu To You Pra Cli Gui To The Cli Neu and BraDocument197 pagesAdd Neu To You Pra Cli Gui To The Cli Neu and BraDomingo Torres S100% (1)
- Oxy ReportDocument83 pagesOxy ReportPride Sikipa0% (1)
- Regional Nerve Blocks in Anesthesia and Pain Therapy Imaging Guided and Traditional Techniques Danilo Jankovic Editor Philip Peng EditorDocument70 pagesRegional Nerve Blocks in Anesthesia and Pain Therapy Imaging Guided and Traditional Techniques Danilo Jankovic Editor Philip Peng Editorjaimemoeller819896100% (6)
- PDF Arthroscopy Basic To Advanced 1St Edition Pietro Randelli Ebook Full ChapterDocument53 pagesPDF Arthroscopy Basic To Advanced 1St Edition Pietro Randelli Ebook Full Chapterjohn.campos373100% (4)
- Psilocybin Tyls 2014Document16 pagesPsilocybin Tyls 2014Sergio Elias Mateus ReyesNo ratings yet
- INSHPO Capability FrameworkDocument51 pagesINSHPO Capability FrameworkAndy MayNo ratings yet
- Master Thesis LuoDocument89 pagesMaster Thesis LuoLuisNo ratings yet
- Full Report - English FINALDocument126 pagesFull Report - English FINALMarcia KoikeNo ratings yet
- Textbook Putting Systems and Complexity Sciences Into Practice Joachim P Sturmberg Ebook All Chapter PDFDocument53 pagesTextbook Putting Systems and Complexity Sciences Into Practice Joachim P Sturmberg Ebook All Chapter PDFmichael.servin593100% (7)
- (Neuromethods 138) Felipe Fregni - Clinical Trials in Neurology-Springer New York - Humana Press (2018)Document614 pages(Neuromethods 138) Felipe Fregni - Clinical Trials in Neurology-Springer New York - Humana Press (2018)Eric Grossi MoratoNo ratings yet
- Long Term Care in Europe A Juridical Approach PDFDocument604 pagesLong Term Care in Europe A Juridical Approach PDFKarina SmithNo ratings yet
- Full Chapter Brain Computer Interface Research A State of The Art Summary 8 Christoph Guger PDFDocument53 pagesFull Chapter Brain Computer Interface Research A State of The Art Summary 8 Christoph Guger PDFkelly.phillips528100% (6)
- Persistent Work Related Technology Use Recovery and Well Being Processes Focus On Supplemental Work After Hours 1st Edition Lenka UranováDocument54 pagesPersistent Work Related Technology Use Recovery and Well Being Processes Focus On Supplemental Work After Hours 1st Edition Lenka Uranovácharles.sanders769100% (3)
- The Effect of Osteopathic Manipulative Techniques On Diaphragm Movement and Respiratory Function in Asymptomatic SubjectsDocument76 pagesThe Effect of Osteopathic Manipulative Techniques On Diaphragm Movement and Respiratory Function in Asymptomatic SubjectsVladislav Kotov100% (1)
- Cowley Etal 2016 The Psychophysiology Primer-Vol11-HCI-065-1100000065Document162 pagesCowley Etal 2016 The Psychophysiology Primer-Vol11-HCI-065-1100000065joelmuk2001No ratings yet
- BIOL200 Prereading GuideDocument24 pagesBIOL200 Prereading GuideParveen BrarNo ratings yet
- Human Anatomy RespiratoryDocument36 pagesHuman Anatomy RespiratoryHafid JuniorNo ratings yet
- Peace Corps Life Skills Manual 2001 M0063Document254 pagesPeace Corps Life Skills Manual 2001 M0063Accessible Journal Media: Peace Corps Documents100% (2)
- Neurological Examination Made Easy 6Th Edition Fuller Geraint Full ChapterDocument67 pagesNeurological Examination Made Easy 6Th Edition Fuller Geraint Full Chapterlinda.elgin584100% (10)
- Tutorial Book On Asset Management - Maintenance and Replacement Strategies at The IEEE PES ... PDFDocument108 pagesTutorial Book On Asset Management - Maintenance and Replacement Strategies at The IEEE PES ... PDFnasrulsalman9883No ratings yet
- CBC 1 de 1Document97 pagesCBC 1 de 1José Luis PsicoterapeutaNo ratings yet
- Case Studies in Applied Psychophysiology: Neurofeedback and Biofeedback Treatments for Advances in Human PerformanceFrom EverandCase Studies in Applied Psychophysiology: Neurofeedback and Biofeedback Treatments for Advances in Human PerformanceNo ratings yet
- Working Misunderstandings: An Ethnography of Project Collaboration in a Multinational Corporation in IndiaFrom EverandWorking Misunderstandings: An Ethnography of Project Collaboration in a Multinational Corporation in IndiaNo ratings yet
- Certificate of Registration - Ms Jisna Panackaparambil Xavier 1Document2 pagesCertificate of Registration - Ms Jisna Panackaparambil Xavier 1api-541029403No ratings yet
- Lepy 103Document19 pagesLepy 103Syed FerozNo ratings yet
- Procedures On OutsourcingDocument2 pagesProcedures On OutsourcingQUINCY75% (4)
- Cover Letter For Thesis Questionnaire SampleDocument6 pagesCover Letter For Thesis Questionnaire SampleHelpWithPaperEverett100% (1)
- Narrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022Document2 pagesNarrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022JAYSON BALINBINNo ratings yet
- DRR11/12-Ic-8. Explain The Meaning of VulnerabilityDocument6 pagesDRR11/12-Ic-8. Explain The Meaning of VulnerabilityallanrnmanalotoNo ratings yet
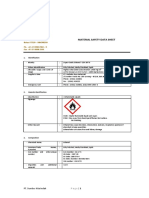
- Material Safety Data Sheet: Pt. Sumber Kita IndahDocument6 pagesMaterial Safety Data Sheet: Pt. Sumber Kita Indahcakradaya indonesiaNo ratings yet
- TM-9-2350-261-10 Μ113Α2Document765 pagesTM-9-2350-261-10 Μ113Α2Thoukididis ThoukididouNo ratings yet
- IFU Dia TT EN 20170915Document2 pagesIFU Dia TT EN 20170915P managerNo ratings yet
- Connection of Health and Daily Routines - Scoala Profesionala CorlatelDocument163 pagesConnection of Health and Daily Routines - Scoala Profesionala CorlatelOTILIA INA CRĂCEANo ratings yet
- Read This Passage and Then Answer The Questions That FollowDocument3 pagesRead This Passage and Then Answer The Questions That FollowWong MkNo ratings yet
- Junior 100m BDocument5 pagesJunior 100m BsjktkbbmNo ratings yet
- Social Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictDocument3 pagesSocial Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictRashmi MishraNo ratings yet
- HYEN-RFQ-ME-004 - RFQ For FET - Rev.C - 210218Document22 pagesHYEN-RFQ-ME-004 - RFQ For FET - Rev.C - 210218MouiciNo ratings yet
- 4 Weeks To Total Posture & Spinal Mobility: Beginner - IntermediateDocument14 pages4 Weeks To Total Posture & Spinal Mobility: Beginner - Intermediate714 BaliNo ratings yet
- 2020-07-16 Calvert County TimesDocument24 pages2020-07-16 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- Ozone Disco FireDocument2 pagesOzone Disco FireNoeme BaylonNo ratings yet
- Berduka Dalam PenjaraDocument9 pagesBerduka Dalam PenjaraTimothy Stevano AlangNo ratings yet
- Mouth Preparation For RPDDocument45 pagesMouth Preparation For RPDArbaz SajjadNo ratings yet
- Human Capital:: Education and Health in Economic DevelopmentDocument17 pagesHuman Capital:: Education and Health in Economic DevelopmentMike AntolinoNo ratings yet
- Chapter 3Document59 pagesChapter 3MATHIS DO CAONo ratings yet
- Transitional Housing ListDocument27 pagesTransitional Housing ListA IDOHERBALIFE IDOHERBABBASLIFENo ratings yet
- Rock Blasting ProceduresDocument21 pagesRock Blasting ProceduresRajanbabu100% (1)
- Qualities of Full-Cream Powdered Milk of Different Brands Available in Retail Markets of BangladeshDocument7 pagesQualities of Full-Cream Powdered Milk of Different Brands Available in Retail Markets of BangladeshSaajed Morshed JaigirdarNo ratings yet
- Axial Ow Artificial Heart Blood Pumps: A Brief Review: Trends in Biomaterials and Artificial Organs January 2013Document8 pagesAxial Ow Artificial Heart Blood Pumps: A Brief Review: Trends in Biomaterials and Artificial Organs January 2013Saad BarnousNo ratings yet
- Kuliah Radiologi Emergensi - Maret 2020 - PlainDocument67 pagesKuliah Radiologi Emergensi - Maret 2020 - PlainArief VerditoNo ratings yet
- 10 Questions For Electrical SafetyDocument1 page10 Questions For Electrical Safetyrizvidawar221No ratings yet
- Introduction To Nursing TheoryDocument33 pagesIntroduction To Nursing TheoryLea Mae FernandezNo ratings yet






















































































Download as pdf or txt
You might also like
- Instant Download Ebook PDF Essentials of Health Culture and Diversity Understanding People Reducing Disparities PDF ScribdDocument47 pagesInstant Download Ebook PDF Essentials of Health Culture and Diversity Understanding People Reducing Disparities PDF Scribdjames.nohel84498% (49)
- Opd Task Force Operationalized Psychodynamic Diagnosis OPD 2 - Manual of Diagnosis and Treatment Planning Hogrefe Huber Pub 2007 PDFDocument438 pagesOpd Task Force Operationalized Psychodynamic Diagnosis OPD 2 - Manual of Diagnosis and Treatment Planning Hogrefe Huber Pub 2007 PDFნინა ზედგინიძეNo ratings yet
- Manual MusclelabDocument20 pagesManual MusclelaboscampoNo ratings yet
- Cardio Kick Boxing-1 PDFDocument78 pagesCardio Kick Boxing-1 PDFmarsnetworkNo ratings yet
- Research and Development in Adult Education: Fields and TrendsFrom EverandResearch and Development in Adult Education: Fields and TrendsNo ratings yet
- Introduction For Nurse Leader InterviewDocument4 pagesIntroduction For Nurse Leader Interviewapi-312833369No ratings yet
- Textbook Exploring Protein Structure Principles and Practice Tim Skern Ebook All Chapter PDFDocument53 pagesTextbook Exploring Protein Structure Principles and Practice Tim Skern Ebook All Chapter PDFjustin.mallard475100% (16)
- SCI L2-S5 Expected Outcome GuideDocument23 pagesSCI L2-S5 Expected Outcome Guidejustgio928No ratings yet
- Full Chapter Muscle Revolution Concepts and Recipes For Building Muscle Mass and Force 1St Edition Marco Toigo PDFDocument53 pagesFull Chapter Muscle Revolution Concepts and Recipes For Building Muscle Mass and Force 1St Edition Marco Toigo PDFmatthew.marshall671100% (6)
- Traumatic Brain Injury 1St Edition Stephen Honeybul Angelos G Kolias Online Ebook Texxtbook Full Chapter PDFDocument69 pagesTraumatic Brain Injury 1St Edition Stephen Honeybul Angelos G Kolias Online Ebook Texxtbook Full Chapter PDFtheressafinch614100% (7)
- 3. ACENS학회 - program PDFDocument100 pages3. ACENS학회 - program PDFHanmin ParkNo ratings yet
- Textbook Cortical Development Neural Diversity and Neocortical Organization 1St Edition Hiromi Shimojo Ebook All Chapter PDFDocument53 pagesTextbook Cortical Development Neural Diversity and Neocortical Organization 1St Edition Hiromi Shimojo Ebook All Chapter PDFhelen.reed309100% (13)
- Textbook Life Care Planning and Case Management Handbook Fourth Edition Berens Ebook All Chapter PDFDocument53 pagesTextbook Life Care Planning and Case Management Handbook Fourth Edition Berens Ebook All Chapter PDFbarbara.ritter532100% (14)
- Textbook Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes Irene Comisso Et Al Ebook All Chapter PDFDocument53 pagesTextbook Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes Irene Comisso Et Al Ebook All Chapter PDFashley.burnham607100% (11)
- PDF Topographic Organization of The Pectine Neuropils in Scorpions An Analysis of Chemosensory Afferents and The Projection Pattern in The Central Nervous System Denise Drozd Ebook Full ChapterDocument54 pagesPDF Topographic Organization of The Pectine Neuropils in Scorpions An Analysis of Chemosensory Afferents and The Projection Pattern in The Central Nervous System Denise Drozd Ebook Full Chapterburl.juel661100% (1)
- Neuropsychiatric Disorders - Miyoshi, Koho (2010)Document339 pagesNeuropsychiatric Disorders - Miyoshi, Koho (2010)Ramon MagsaysayNo ratings yet
- Guidelines For The Organizat PDFDocument15 pagesGuidelines For The Organizat PDFAlagappan ThiyagarajanNo ratings yet
- Franck Billmann, Tobias Keck Essentials of Visceral Surgery ForDocument392 pagesFranck Billmann, Tobias Keck Essentials of Visceral Surgery ForOurtching NestorNo ratings yet
- Full Chapter in Vivo Neuropharmacology and Neurophysiology 1St Edition Athineos Philippu Eds PDFDocument34 pagesFull Chapter in Vivo Neuropharmacology and Neurophysiology 1St Edition Athineos Philippu Eds PDFkim.gomez589100% (8)
- Clinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtDocument29 pagesClinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtGlauber Teixeira Ervilha100% (1)
- SOP ExerciseTherapy - e - Eng PDFDocument372 pagesSOP ExerciseTherapy - e - Eng PDFEli WatiNo ratings yet
- 指南手册Document119 pages指南手册HugoNo ratings yet
- A Visual Guide To Clinical Anatomy Oct 19 2020 - 1119708109 - Wiley Blackwell 1St Edition Whitaker Full Chapter PDFDocument70 pagesA Visual Guide To Clinical Anatomy Oct 19 2020 - 1119708109 - Wiley Blackwell 1St Edition Whitaker Full Chapter PDFjayetcoxca100% (9)
- PDF Data and Text Processing For Health and Life Sciences Francisco M Couto Ebook Full ChapterDocument53 pagesPDF Data and Text Processing For Health and Life Sciences Francisco M Couto Ebook Full Chapterjanice.quillen556100% (3)
- Leadership and OSHDocument61 pagesLeadership and OSHShabin ShabiNo ratings yet
- QPBR HandbookDocument120 pagesQPBR HandbookGeetha RajashekharNo ratings yet
- ebook download Neurological Examination. Made Easy 6th Edition Fuller Geraint - eBook PDF all chapterDocument54 pagesebook download Neurological Examination. Made Easy 6th Edition Fuller Geraint - eBook PDF all chapteraidokabajaro100% (3)
- Full Download PDF of Neurological Examination. Made Easy 6th Edition Fuller Geraint - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Neurological Examination. Made Easy 6th Edition Fuller Geraint - Ebook PDF All Chapterokornkisida100% (6)
- Taquicardia SupraventricularDocument69 pagesTaquicardia Supraventricularwindar baqueroNo ratings yet
- ACE PT4th Manual Ch1Document69 pagesACE PT4th Manual Ch1chandramouuli78% (9)
- Full Chapter Musculoskeletal Imaging A Survival Manual 1St Edition Plotkin PDFDocument53 pagesFull Chapter Musculoskeletal Imaging A Survival Manual 1St Edition Plotkin PDFjohn.miller951100% (9)
- Leadership and Occupational Safety and Health (OSH) : An Expert AnalysisDocument62 pagesLeadership and Occupational Safety and Health (OSH) : An Expert Analysishuu nguyen nguyenNo ratings yet
- Musculoskeletal Injections Manual - Basics, Techniques and Injectable Agents (Apr 25, 2024) - (3031526023) - (Springer) 1st Edition Baris KocaogluDocument54 pagesMusculoskeletal Injections Manual - Basics, Techniques and Injectable Agents (Apr 25, 2024) - (3031526023) - (Springer) 1st Edition Baris Kocaoglujohn.miller951100% (7)
- Authors:: Sports Physiotherapy Competencies and StandardsDocument78 pagesAuthors:: Sports Physiotherapy Competencies and Standards杨钦杰No ratings yet
- Culture Assessment Soar enDocument79 pagesCulture Assessment Soar enHrishikesh PNo ratings yet
- 2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaDocument3 pages2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaBuya TaftaNo ratings yet
- Job Seeker's Workbook - JISTDocument81 pagesJob Seeker's Workbook - JISTteewako100% (1)
- Add Neu To You Pra Cli Gui To The Cli Neu and BraDocument197 pagesAdd Neu To You Pra Cli Gui To The Cli Neu and BraDomingo Torres S100% (1)
- Oxy ReportDocument83 pagesOxy ReportPride Sikipa0% (1)
- Regional Nerve Blocks in Anesthesia and Pain Therapy Imaging Guided and Traditional Techniques Danilo Jankovic Editor Philip Peng EditorDocument70 pagesRegional Nerve Blocks in Anesthesia and Pain Therapy Imaging Guided and Traditional Techniques Danilo Jankovic Editor Philip Peng Editorjaimemoeller819896100% (6)
- PDF Arthroscopy Basic To Advanced 1St Edition Pietro Randelli Ebook Full ChapterDocument53 pagesPDF Arthroscopy Basic To Advanced 1St Edition Pietro Randelli Ebook Full Chapterjohn.campos373100% (4)
- Psilocybin Tyls 2014Document16 pagesPsilocybin Tyls 2014Sergio Elias Mateus ReyesNo ratings yet
- INSHPO Capability FrameworkDocument51 pagesINSHPO Capability FrameworkAndy MayNo ratings yet
- Master Thesis LuoDocument89 pagesMaster Thesis LuoLuisNo ratings yet
- Full Report - English FINALDocument126 pagesFull Report - English FINALMarcia KoikeNo ratings yet
- Textbook Putting Systems and Complexity Sciences Into Practice Joachim P Sturmberg Ebook All Chapter PDFDocument53 pagesTextbook Putting Systems and Complexity Sciences Into Practice Joachim P Sturmberg Ebook All Chapter PDFmichael.servin593100% (7)
- (Neuromethods 138) Felipe Fregni - Clinical Trials in Neurology-Springer New York - Humana Press (2018)Document614 pages(Neuromethods 138) Felipe Fregni - Clinical Trials in Neurology-Springer New York - Humana Press (2018)Eric Grossi MoratoNo ratings yet
- Long Term Care in Europe A Juridical Approach PDFDocument604 pagesLong Term Care in Europe A Juridical Approach PDFKarina SmithNo ratings yet
- Full Chapter Brain Computer Interface Research A State of The Art Summary 8 Christoph Guger PDFDocument53 pagesFull Chapter Brain Computer Interface Research A State of The Art Summary 8 Christoph Guger PDFkelly.phillips528100% (6)
- Persistent Work Related Technology Use Recovery and Well Being Processes Focus On Supplemental Work After Hours 1st Edition Lenka UranováDocument54 pagesPersistent Work Related Technology Use Recovery and Well Being Processes Focus On Supplemental Work After Hours 1st Edition Lenka Uranovácharles.sanders769100% (3)
- The Effect of Osteopathic Manipulative Techniques On Diaphragm Movement and Respiratory Function in Asymptomatic SubjectsDocument76 pagesThe Effect of Osteopathic Manipulative Techniques On Diaphragm Movement and Respiratory Function in Asymptomatic SubjectsVladislav Kotov100% (1)
- Cowley Etal 2016 The Psychophysiology Primer-Vol11-HCI-065-1100000065Document162 pagesCowley Etal 2016 The Psychophysiology Primer-Vol11-HCI-065-1100000065joelmuk2001No ratings yet
- BIOL200 Prereading GuideDocument24 pagesBIOL200 Prereading GuideParveen BrarNo ratings yet
- Human Anatomy RespiratoryDocument36 pagesHuman Anatomy RespiratoryHafid JuniorNo ratings yet
- Peace Corps Life Skills Manual 2001 M0063Document254 pagesPeace Corps Life Skills Manual 2001 M0063Accessible Journal Media: Peace Corps Documents100% (2)
- Neurological Examination Made Easy 6Th Edition Fuller Geraint Full ChapterDocument67 pagesNeurological Examination Made Easy 6Th Edition Fuller Geraint Full Chapterlinda.elgin584100% (10)
- Tutorial Book On Asset Management - Maintenance and Replacement Strategies at The IEEE PES ... PDFDocument108 pagesTutorial Book On Asset Management - Maintenance and Replacement Strategies at The IEEE PES ... PDFnasrulsalman9883No ratings yet
- CBC 1 de 1Document97 pagesCBC 1 de 1José Luis PsicoterapeutaNo ratings yet
- Case Studies in Applied Psychophysiology: Neurofeedback and Biofeedback Treatments for Advances in Human PerformanceFrom EverandCase Studies in Applied Psychophysiology: Neurofeedback and Biofeedback Treatments for Advances in Human PerformanceNo ratings yet
- Working Misunderstandings: An Ethnography of Project Collaboration in a Multinational Corporation in IndiaFrom EverandWorking Misunderstandings: An Ethnography of Project Collaboration in a Multinational Corporation in IndiaNo ratings yet
- Certificate of Registration - Ms Jisna Panackaparambil Xavier 1Document2 pagesCertificate of Registration - Ms Jisna Panackaparambil Xavier 1api-541029403No ratings yet
- Lepy 103Document19 pagesLepy 103Syed FerozNo ratings yet
- Procedures On OutsourcingDocument2 pagesProcedures On OutsourcingQUINCY75% (4)
- Cover Letter For Thesis Questionnaire SampleDocument6 pagesCover Letter For Thesis Questionnaire SampleHelpWithPaperEverett100% (1)
- Narrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022Document2 pagesNarrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022JAYSON BALINBINNo ratings yet
- DRR11/12-Ic-8. Explain The Meaning of VulnerabilityDocument6 pagesDRR11/12-Ic-8. Explain The Meaning of VulnerabilityallanrnmanalotoNo ratings yet
- Material Safety Data Sheet: Pt. Sumber Kita IndahDocument6 pagesMaterial Safety Data Sheet: Pt. Sumber Kita Indahcakradaya indonesiaNo ratings yet
- TM-9-2350-261-10 Μ113Α2Document765 pagesTM-9-2350-261-10 Μ113Α2Thoukididis ThoukididouNo ratings yet
- IFU Dia TT EN 20170915Document2 pagesIFU Dia TT EN 20170915P managerNo ratings yet
- Connection of Health and Daily Routines - Scoala Profesionala CorlatelDocument163 pagesConnection of Health and Daily Routines - Scoala Profesionala CorlatelOTILIA INA CRĂCEANo ratings yet
- Read This Passage and Then Answer The Questions That FollowDocument3 pagesRead This Passage and Then Answer The Questions That FollowWong MkNo ratings yet
- Junior 100m BDocument5 pagesJunior 100m BsjktkbbmNo ratings yet
- Social Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictDocument3 pagesSocial Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictRashmi MishraNo ratings yet
- HYEN-RFQ-ME-004 - RFQ For FET - Rev.C - 210218Document22 pagesHYEN-RFQ-ME-004 - RFQ For FET - Rev.C - 210218MouiciNo ratings yet
- 4 Weeks To Total Posture & Spinal Mobility: Beginner - IntermediateDocument14 pages4 Weeks To Total Posture & Spinal Mobility: Beginner - Intermediate714 BaliNo ratings yet
- 2020-07-16 Calvert County TimesDocument24 pages2020-07-16 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- Ozone Disco FireDocument2 pagesOzone Disco FireNoeme BaylonNo ratings yet
- Berduka Dalam PenjaraDocument9 pagesBerduka Dalam PenjaraTimothy Stevano AlangNo ratings yet
- Mouth Preparation For RPDDocument45 pagesMouth Preparation For RPDArbaz SajjadNo ratings yet
- Human Capital:: Education and Health in Economic DevelopmentDocument17 pagesHuman Capital:: Education and Health in Economic DevelopmentMike AntolinoNo ratings yet
- Chapter 3Document59 pagesChapter 3MATHIS DO CAONo ratings yet
- Transitional Housing ListDocument27 pagesTransitional Housing ListA IDOHERBALIFE IDOHERBABBASLIFENo ratings yet
- Rock Blasting ProceduresDocument21 pagesRock Blasting ProceduresRajanbabu100% (1)
- Qualities of Full-Cream Powdered Milk of Different Brands Available in Retail Markets of BangladeshDocument7 pagesQualities of Full-Cream Powdered Milk of Different Brands Available in Retail Markets of BangladeshSaajed Morshed JaigirdarNo ratings yet
- Axial Ow Artificial Heart Blood Pumps: A Brief Review: Trends in Biomaterials and Artificial Organs January 2013Document8 pagesAxial Ow Artificial Heart Blood Pumps: A Brief Review: Trends in Biomaterials and Artificial Organs January 2013Saad BarnousNo ratings yet
- Kuliah Radiologi Emergensi - Maret 2020 - PlainDocument67 pagesKuliah Radiologi Emergensi - Maret 2020 - PlainArief VerditoNo ratings yet
- 10 Questions For Electrical SafetyDocument1 page10 Questions For Electrical Safetyrizvidawar221No ratings yet
- Introduction To Nursing TheoryDocument33 pagesIntroduction To Nursing TheoryLea Mae FernandezNo ratings yet