
Architecture Creative SantiagoQuesada
Architecture Creative SantiagoQuesada
You might also like
- Community ArchitectureDocument15 pagesCommunity Architecturefrancescleo8duran92% (13)
- Mostafa, Magda, 'An Architecture For Autism. Concepts of Design Intervention For The Autistic User,' IJAR International Journal of Architectural Research, Vol. 2, Issue 1 (2008) .Document23 pagesMostafa, Magda, 'An Architecture For Autism. Concepts of Design Intervention For The Autistic User,' IJAR International Journal of Architectural Research, Vol. 2, Issue 1 (2008) .rr-waartNo ratings yet
- Public MarketDocument2 pagesPublic MarketKristine Natividad33% (3)
- Aas WorkbookDocument144 pagesAas WorkbookmaionelNo ratings yet
- Tramadol Vancomycin Drug StudyDocument6 pagesTramadol Vancomycin Drug StudyAllene PaderangaNo ratings yet
- Chapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsDocument13 pagesChapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsNishana ShajahanNo ratings yet
- Principles and Examples of Design of RehabilitatioDocument4 pagesPrinciples and Examples of Design of Rehabilitatiosammyxtian24No ratings yet
- Insights Into Living With Dementia: Five Implications For Architectural DesignDocument16 pagesInsights Into Living With Dementia: Five Implications For Architectural DesignTanish MoorjaniNo ratings yet
- Creative Synergies PosterDocument1 pageCreative Synergies PosterMania1710No ratings yet
- LeNS3-Brazil Paper 42Document6 pagesLeNS3-Brazil Paper 42Gabrielle Lana LinharesNo ratings yet
- Submitted ManuscriptDocument26 pagesSubmitted Manuscriptjay jayNo ratings yet
- Dissertation Detailed SynopsisDocument5 pagesDissertation Detailed SynopsisAarthy ArasuNo ratings yet
- Sociology of DesignDocument10 pagesSociology of DesignDiana AnyangoNo ratings yet
- A "Social Model" of Design: Issues of Practice and Research: Victor Margolin and Sylvia MargolinDocument7 pagesA "Social Model" of Design: Issues of Practice and Research: Victor Margolin and Sylvia MargolinCarol HoffmannNo ratings yet
- Urban Living Labs: A Living Lab Way of Working: June 2017Document96 pagesUrban Living Labs: A Living Lab Way of Working: June 2017Hiếu Bùi TrungNo ratings yet
- Electives ScriptDocument12 pagesElectives ScriptAnghelikaaaNo ratings yet
- Sarmiento - Research JournalDocument9 pagesSarmiento - Research JournalPHOEBE SARMIENTONo ratings yet
- The Death of Modern Hospital Towards A RestorativeDocument16 pagesThe Death of Modern Hospital Towards A Restorativeamir alamNo ratings yet
- Galvin - Maya - Spring 2021 - ThesisDocument82 pagesGalvin - Maya - Spring 2021 - ThesisDonia NaseerNo ratings yet
- Expansion of The University Hospital of The Santa Fe de Bogotá FoundationDocument15 pagesExpansion of The University Hospital of The Santa Fe de Bogotá FoundationdnmNo ratings yet
- Design ApproachDocument5 pagesDesign ApproachAseel QtaishatNo ratings yet
- Art in Health Care Buildings:: Marily Cintra, M.SCDocument8 pagesArt in Health Care Buildings:: Marily Cintra, M.SCkonyicska_kingaNo ratings yet
- SUSTAINABLE ARCHITECTURE IN MEXICO ShareDocument4 pagesSUSTAINABLE ARCHITECTURE IN MEXICO ShareGustavoNo ratings yet
- Therapeutic Landscape Design: Methods, Design Strategies and New Scientific ApproachesDocument131 pagesTherapeutic Landscape Design: Methods, Design Strategies and New Scientific ApproachesRahma Azani100% (1)
- Flexible Solutions For Small Spaces in Spatial Design TeachingDocument13 pagesFlexible Solutions For Small Spaces in Spatial Design TeachingAmeya ThanawalaNo ratings yet
- Flexible Housing The Role of Spatial Organization in Achieving Functional EfficiencyDocument13 pagesFlexible Housing The Role of Spatial Organization in Achieving Functional EfficiencySamar BelalNo ratings yet
- Hospital TrialDocument7 pagesHospital TrialScribdTranslationsNo ratings yet
- Making Architecture Visible To The Visually Impaired: Bergen University College, NorwayDocument10 pagesMaking Architecture Visible To The Visually Impaired: Bergen University College, NorwayDaniela VazquezNo ratings yet
- PEO JournalDocument1 pagePEO Journalcorememories10No ratings yet
- Toilet LoResDocument41 pagesToilet LoResSarahNo ratings yet
- ECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Document9 pagesECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Richard OrisakweNo ratings yet
- A71 ChristiansenDocument4 pagesA71 ChristiansenShruti MankarNo ratings yet
- Healthy ArchitectureDocument72 pagesHealthy ArchitectureHarshit GuptaNo ratings yet
- Part 2Document10 pagesPart 2KeishaNo ratings yet
- 96 101 ISrael NagoreDocument6 pages96 101 ISrael NagoreDavid Mesa CedilloNo ratings yet
- Chapter 1-3Document15 pagesChapter 1-3Decca Lyn SalvadorNo ratings yet
- Constantino Design 3 Research Not Yet FinalDocument11 pagesConstantino Design 3 Research Not Yet FinalDhei ConstantinoNo ratings yet
- Carrillo-Hermosilla, Del Río, Könnölä - 2010 - Diversity of Eco-Innovations Reflections From Selected Case Studies-AnnotatedDocument25 pagesCarrillo-Hermosilla, Del Río, Könnölä - 2010 - Diversity of Eco-Innovations Reflections From Selected Case Studies-AnnotatedRicardo PucinelliNo ratings yet
- 1.1.3 Statement of The ProblemDocument4 pages1.1.3 Statement of The ProblemObispado Trophy MakerNo ratings yet
- Children's Cancer and Transplant Hospital: A Micro Town Within A BubbleDocument111 pagesChildren's Cancer and Transplant Hospital: A Micro Town Within A BubbleANUPAMA CNo ratings yet
- Design BriefDocument7 pagesDesign BriefOrianaFernandezNo ratings yet
- Design Patterns and Living ArchitectureDocument32 pagesDesign Patterns and Living ArchitectureMiguel Córdova RamirezNo ratings yet
- Alexandria Health CentreDocument5 pagesAlexandria Health CentrednmNo ratings yet
- ARM 402-Module1Document11 pagesARM 402-Module1camillefaith.gonzagaNo ratings yet
- Resumo Alargado RaquelRibeiroDocument10 pagesResumo Alargado RaquelRibeiroHossam Abo SeadaNo ratings yet
- 22 基于患者自传的几个建筑设计独立住宅、附属住宅和公寓Document17 pages22 基于患者自传的几个建筑设计独立住宅、附属住宅和公寓Xiner DongNo ratings yet
- (Youd Want An Energy From A Building) - User Experience of Healing Environment in A Maggies Cancer Caring CentreDocument10 pages(Youd Want An Energy From A Building) - User Experience of Healing Environment in A Maggies Cancer Caring CentremiNo ratings yet
- Principles and Examples of Design of Rehabilitation Centers in Russia and AbroadDocument6 pagesPrinciples and Examples of Design of Rehabilitation Centers in Russia and Abroadkratika gargNo ratings yet
- Modular, Sustainable and Customized: Projects For The Contemporary DwellingDocument11 pagesModular, Sustainable and Customized: Projects For The Contemporary DwellingPATEL MIHIKANo ratings yet
- 1.1.3 Statement of The ProblemDocument4 pages1.1.3 Statement of The ProblemObispado Trophy MakerNo ratings yet
- Literature Review in Home Care: Bushra Bashir, Michelle Chabrol, Christophe CauxDocument11 pagesLiterature Review in Home Care: Bushra Bashir, Michelle Chabrol, Christophe CauxCel CuttyNo ratings yet
- Case Study Carlos HospitalDocument7 pagesCase Study Carlos HospitalAnimesh AgrawalNo ratings yet
- The Elements of A Caring EnvironmentDocument6 pagesThe Elements of A Caring EnvironmentAhmad UmarNo ratings yet
- 6 1 ObaidatDocument10 pages6 1 Obaidatarki tekturaNo ratings yet
- AGED-CARE FACILITY ResearchDocument26 pagesAGED-CARE FACILITY ResearchVictoria VillanuevaNo ratings yet
- Biomimicry in Structural Designs of BuildingsDocument17 pagesBiomimicry in Structural Designs of BuildingsAllen Sapinoso AlejoNo ratings yet
- How Architectural Design Affords Experiences of Freedom in Residential Care for Older People. 建筑设计如何为老年人提供养老院的自由体验Document25 pagesHow Architectural Design Affords Experiences of Freedom in Residential Care for Older People. 建筑设计如何为老年人提供养老院的自由体验siqi zhanNo ratings yet
- Industrial Symbiosis for the Circular Economy: Operational Experiences, Best Practices and Obstacles to a Collaborative Business ApproachFrom EverandIndustrial Symbiosis for the Circular Economy: Operational Experiences, Best Practices and Obstacles to a Collaborative Business ApproachRoberta SalomoneNo ratings yet
- The Covert Life of Hospital ArchitectureFrom EverandThe Covert Life of Hospital ArchitectureJulie ZookNo ratings yet
- CV - Asjad AbdulWahabDocument1 pageCV - Asjad AbdulWahabjay jayNo ratings yet
- Business Plan Assignment (BP) - Group4Document21 pagesBusiness Plan Assignment (BP) - Group4jay jayNo ratings yet
- Haobin Fu College of Art and Design, Nanyang Institute of Technology, Nanyang, 473000, ChinaDocument7 pagesHaobin Fu College of Art and Design, Nanyang Institute of Technology, Nanyang, 473000, Chinajay jayNo ratings yet
- Application of AI Technology in Interior DesignDocument6 pagesApplication of AI Technology in Interior Designjay jayNo ratings yet
- Black and White Minimalist Commercial Real Estate Architecture PresentationDocument13 pagesBlack and White Minimalist Commercial Real Estate Architecture Presentationjay jayNo ratings yet
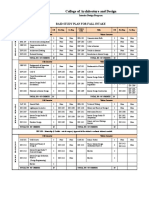
- Study Plan Bachelor of Interior DesignDocument3 pagesStudy Plan Bachelor of Interior Designjay jayNo ratings yet
- Matrikx Cto Data SheetDocument2 pagesMatrikx Cto Data Sheetjay jayNo ratings yet
- Family Care ClinicDocument23 pagesFamily Care Clinicjay jayNo ratings yet
- Sarasatr,+17 +Sajid+I+Awal+210-223Document14 pagesSarasatr,+17 +Sajid+I+Awal+210-223jay jayNo ratings yet
- NatlsocDocument9 pagesNatlsocjay jayNo ratings yet
- 2006 Publicand Private Spacein Urban AreasDocument12 pages2006 Publicand Private Spacein Urban Areasjay jayNo ratings yet
- 0733464815574094.full 2 2Document24 pages0733464815574094.full 2 2jay jayNo ratings yet
- Submitted ManuscriptDocument26 pagesSubmitted Manuscriptjay jayNo ratings yet
- Document 1Document3 pagesDocument 1jay jayNo ratings yet
- Advocate LutheranDocument4 pagesAdvocate Lutheranjay jayNo ratings yet
- Aktiviti Latihan Terapi AirDocument2 pagesAktiviti Latihan Terapi Airas-suhairiNo ratings yet
- Biology Contents - RPSC FSO by Food TecKnowDocument35 pagesBiology Contents - RPSC FSO by Food TecKnowRahul JainNo ratings yet
- Managment of Trauma Patient in ERDocument46 pagesManagment of Trauma Patient in ERtofanNo ratings yet
- Advocacy Letter-Amy JohnsDocument2 pagesAdvocacy Letter-Amy Johnsapi-239145075No ratings yet
- EPI Lecture Note April 2005, YemaneDocument132 pagesEPI Lecture Note April 2005, YemaneGetahun TekleNo ratings yet
- Pre-NEET Pediatrics Taruna MehraDocument181 pagesPre-NEET Pediatrics Taruna MehraNick Amonsull Phanuwat0% (1)
- My LogDocument229 pagesMy Logsowpij290laslNo ratings yet
- Hollow Organ InjuryDocument47 pagesHollow Organ InjuryreginaNo ratings yet
- Significance of Gulika: by Dr. Suresh Chandra Mishra, IndiaDocument10 pagesSignificance of Gulika: by Dr. Suresh Chandra Mishra, IndiaAnonymous jGdHMEODVmNo ratings yet
- 2022 - Acute Kidney Injury and Critical Care NephrologyDocument123 pages2022 - Acute Kidney Injury and Critical Care NephrologyEdson MarquesNo ratings yet
- Lab Report Exp 2 - Kidney Function & Physiology (Group 4)Document10 pagesLab Report Exp 2 - Kidney Function & Physiology (Group 4)FARHAH BATRISYIA ABDUL RAHIMNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryInternos YopalNo ratings yet
- Group 2 Case Study MergedDocument12 pagesGroup 2 Case Study MergedKobe Bryan GermoNo ratings yet
- Assignment of Pathology 401: Submitted byDocument5 pagesAssignment of Pathology 401: Submitted byaymen gulzarNo ratings yet
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- Natural Aromatase InhibitorsDocument69 pagesNatural Aromatase InhibitorsIme Muško OsječkoNo ratings yet
- Sociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilDocument8 pagesSociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilInternational Medical PublisherNo ratings yet
- Operating RoomDocument9 pagesOperating RoomMarie Ashley CasiaNo ratings yet
- An Update On Oral Human Papillomavirus Infection: Review ArticleDocument7 pagesAn Update On Oral Human Papillomavirus Infection: Review ArticlebungagladysNo ratings yet
- Cole Crops and Other Brassicas: Organic Production: AttraDocument20 pagesCole Crops and Other Brassicas: Organic Production: AttraRebecca SheaNo ratings yet
- Origin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesDocument11 pagesOrigin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesmmbasquesNo ratings yet
- Renal PediatricDocument48 pagesRenal PediatricEslam R. Almassri100% (1)
- Health Talk ExcerciseDocument5 pagesHealth Talk ExcerciseNyalen Hakom100% (1)
- Case Report 3 MukokelDocument3 pagesCase Report 3 MukokelWidychii GadiestchhetyaNo ratings yet
- Anthonela - Terán SebastiánDocument5 pagesAnthonela - Terán SebastiánJuleyssiNo ratings yet
- DissociativeidentitydisorderDocument8 pagesDissociativeidentitydisorderapi-355984916No ratings yet
- Chordal Preservation TechniquesDocument8 pagesChordal Preservation TechniquesKunwar Sidharth SaurabhNo ratings yet
- Chronic Myeloid LeukemiaDocument26 pagesChronic Myeloid LeukemiaasaleemnaNo ratings yet
- Septic Arthritis AssignmentDocument14 pagesSeptic Arthritis AssignmentDEO NDAYISABANo ratings yet





































































































Download as pdf or txt
You might also like
- Community ArchitectureDocument15 pagesCommunity Architecturefrancescleo8duran92% (13)
- Mostafa, Magda, 'An Architecture For Autism. Concepts of Design Intervention For The Autistic User,' IJAR International Journal of Architectural Research, Vol. 2, Issue 1 (2008) .Document23 pagesMostafa, Magda, 'An Architecture For Autism. Concepts of Design Intervention For The Autistic User,' IJAR International Journal of Architectural Research, Vol. 2, Issue 1 (2008) .rr-waartNo ratings yet
- Public MarketDocument2 pagesPublic MarketKristine Natividad33% (3)
- Aas WorkbookDocument144 pagesAas WorkbookmaionelNo ratings yet
- Tramadol Vancomycin Drug StudyDocument6 pagesTramadol Vancomycin Drug StudyAllene PaderangaNo ratings yet
- Chapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsDocument13 pagesChapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsNishana ShajahanNo ratings yet
- Principles and Examples of Design of RehabilitatioDocument4 pagesPrinciples and Examples of Design of Rehabilitatiosammyxtian24No ratings yet
- Insights Into Living With Dementia: Five Implications For Architectural DesignDocument16 pagesInsights Into Living With Dementia: Five Implications For Architectural DesignTanish MoorjaniNo ratings yet
- Creative Synergies PosterDocument1 pageCreative Synergies PosterMania1710No ratings yet
- LeNS3-Brazil Paper 42Document6 pagesLeNS3-Brazil Paper 42Gabrielle Lana LinharesNo ratings yet
- Submitted ManuscriptDocument26 pagesSubmitted Manuscriptjay jayNo ratings yet
- Dissertation Detailed SynopsisDocument5 pagesDissertation Detailed SynopsisAarthy ArasuNo ratings yet
- Sociology of DesignDocument10 pagesSociology of DesignDiana AnyangoNo ratings yet
- A "Social Model" of Design: Issues of Practice and Research: Victor Margolin and Sylvia MargolinDocument7 pagesA "Social Model" of Design: Issues of Practice and Research: Victor Margolin and Sylvia MargolinCarol HoffmannNo ratings yet
- Urban Living Labs: A Living Lab Way of Working: June 2017Document96 pagesUrban Living Labs: A Living Lab Way of Working: June 2017Hiếu Bùi TrungNo ratings yet
- Electives ScriptDocument12 pagesElectives ScriptAnghelikaaaNo ratings yet
- Sarmiento - Research JournalDocument9 pagesSarmiento - Research JournalPHOEBE SARMIENTONo ratings yet
- The Death of Modern Hospital Towards A RestorativeDocument16 pagesThe Death of Modern Hospital Towards A Restorativeamir alamNo ratings yet
- Galvin - Maya - Spring 2021 - ThesisDocument82 pagesGalvin - Maya - Spring 2021 - ThesisDonia NaseerNo ratings yet
- Expansion of The University Hospital of The Santa Fe de Bogotá FoundationDocument15 pagesExpansion of The University Hospital of The Santa Fe de Bogotá FoundationdnmNo ratings yet
- Design ApproachDocument5 pagesDesign ApproachAseel QtaishatNo ratings yet
- Art in Health Care Buildings:: Marily Cintra, M.SCDocument8 pagesArt in Health Care Buildings:: Marily Cintra, M.SCkonyicska_kingaNo ratings yet
- SUSTAINABLE ARCHITECTURE IN MEXICO ShareDocument4 pagesSUSTAINABLE ARCHITECTURE IN MEXICO ShareGustavoNo ratings yet
- Therapeutic Landscape Design: Methods, Design Strategies and New Scientific ApproachesDocument131 pagesTherapeutic Landscape Design: Methods, Design Strategies and New Scientific ApproachesRahma Azani100% (1)
- Flexible Solutions For Small Spaces in Spatial Design TeachingDocument13 pagesFlexible Solutions For Small Spaces in Spatial Design TeachingAmeya ThanawalaNo ratings yet
- Flexible Housing The Role of Spatial Organization in Achieving Functional EfficiencyDocument13 pagesFlexible Housing The Role of Spatial Organization in Achieving Functional EfficiencySamar BelalNo ratings yet
- Hospital TrialDocument7 pagesHospital TrialScribdTranslationsNo ratings yet
- Making Architecture Visible To The Visually Impaired: Bergen University College, NorwayDocument10 pagesMaking Architecture Visible To The Visually Impaired: Bergen University College, NorwayDaniela VazquezNo ratings yet
- PEO JournalDocument1 pagePEO Journalcorememories10No ratings yet
- Toilet LoResDocument41 pagesToilet LoResSarahNo ratings yet
- ECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Document9 pagesECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Richard OrisakweNo ratings yet
- A71 ChristiansenDocument4 pagesA71 ChristiansenShruti MankarNo ratings yet
- Healthy ArchitectureDocument72 pagesHealthy ArchitectureHarshit GuptaNo ratings yet
- Part 2Document10 pagesPart 2KeishaNo ratings yet
- 96 101 ISrael NagoreDocument6 pages96 101 ISrael NagoreDavid Mesa CedilloNo ratings yet
- Chapter 1-3Document15 pagesChapter 1-3Decca Lyn SalvadorNo ratings yet
- Constantino Design 3 Research Not Yet FinalDocument11 pagesConstantino Design 3 Research Not Yet FinalDhei ConstantinoNo ratings yet
- Carrillo-Hermosilla, Del Río, Könnölä - 2010 - Diversity of Eco-Innovations Reflections From Selected Case Studies-AnnotatedDocument25 pagesCarrillo-Hermosilla, Del Río, Könnölä - 2010 - Diversity of Eco-Innovations Reflections From Selected Case Studies-AnnotatedRicardo PucinelliNo ratings yet
- 1.1.3 Statement of The ProblemDocument4 pages1.1.3 Statement of The ProblemObispado Trophy MakerNo ratings yet
- Children's Cancer and Transplant Hospital: A Micro Town Within A BubbleDocument111 pagesChildren's Cancer and Transplant Hospital: A Micro Town Within A BubbleANUPAMA CNo ratings yet
- Design BriefDocument7 pagesDesign BriefOrianaFernandezNo ratings yet
- Design Patterns and Living ArchitectureDocument32 pagesDesign Patterns and Living ArchitectureMiguel Córdova RamirezNo ratings yet
- Alexandria Health CentreDocument5 pagesAlexandria Health CentrednmNo ratings yet
- ARM 402-Module1Document11 pagesARM 402-Module1camillefaith.gonzagaNo ratings yet
- Resumo Alargado RaquelRibeiroDocument10 pagesResumo Alargado RaquelRibeiroHossam Abo SeadaNo ratings yet
- 22 基于患者自传的几个建筑设计独立住宅、附属住宅和公寓Document17 pages22 基于患者自传的几个建筑设计独立住宅、附属住宅和公寓Xiner DongNo ratings yet
- (Youd Want An Energy From A Building) - User Experience of Healing Environment in A Maggies Cancer Caring CentreDocument10 pages(Youd Want An Energy From A Building) - User Experience of Healing Environment in A Maggies Cancer Caring CentremiNo ratings yet
- Principles and Examples of Design of Rehabilitation Centers in Russia and AbroadDocument6 pagesPrinciples and Examples of Design of Rehabilitation Centers in Russia and Abroadkratika gargNo ratings yet
- Modular, Sustainable and Customized: Projects For The Contemporary DwellingDocument11 pagesModular, Sustainable and Customized: Projects For The Contemporary DwellingPATEL MIHIKANo ratings yet
- 1.1.3 Statement of The ProblemDocument4 pages1.1.3 Statement of The ProblemObispado Trophy MakerNo ratings yet
- Literature Review in Home Care: Bushra Bashir, Michelle Chabrol, Christophe CauxDocument11 pagesLiterature Review in Home Care: Bushra Bashir, Michelle Chabrol, Christophe CauxCel CuttyNo ratings yet
- Case Study Carlos HospitalDocument7 pagesCase Study Carlos HospitalAnimesh AgrawalNo ratings yet
- The Elements of A Caring EnvironmentDocument6 pagesThe Elements of A Caring EnvironmentAhmad UmarNo ratings yet
- 6 1 ObaidatDocument10 pages6 1 Obaidatarki tekturaNo ratings yet
- AGED-CARE FACILITY ResearchDocument26 pagesAGED-CARE FACILITY ResearchVictoria VillanuevaNo ratings yet
- Biomimicry in Structural Designs of BuildingsDocument17 pagesBiomimicry in Structural Designs of BuildingsAllen Sapinoso AlejoNo ratings yet
- How Architectural Design Affords Experiences of Freedom in Residential Care for Older People. 建筑设计如何为老年人提供养老院的自由体验Document25 pagesHow Architectural Design Affords Experiences of Freedom in Residential Care for Older People. 建筑设计如何为老年人提供养老院的自由体验siqi zhanNo ratings yet
- Industrial Symbiosis for the Circular Economy: Operational Experiences, Best Practices and Obstacles to a Collaborative Business ApproachFrom EverandIndustrial Symbiosis for the Circular Economy: Operational Experiences, Best Practices and Obstacles to a Collaborative Business ApproachRoberta SalomoneNo ratings yet
- The Covert Life of Hospital ArchitectureFrom EverandThe Covert Life of Hospital ArchitectureJulie ZookNo ratings yet
- CV - Asjad AbdulWahabDocument1 pageCV - Asjad AbdulWahabjay jayNo ratings yet
- Business Plan Assignment (BP) - Group4Document21 pagesBusiness Plan Assignment (BP) - Group4jay jayNo ratings yet
- Haobin Fu College of Art and Design, Nanyang Institute of Technology, Nanyang, 473000, ChinaDocument7 pagesHaobin Fu College of Art and Design, Nanyang Institute of Technology, Nanyang, 473000, Chinajay jayNo ratings yet
- Application of AI Technology in Interior DesignDocument6 pagesApplication of AI Technology in Interior Designjay jayNo ratings yet
- Black and White Minimalist Commercial Real Estate Architecture PresentationDocument13 pagesBlack and White Minimalist Commercial Real Estate Architecture Presentationjay jayNo ratings yet
- Study Plan Bachelor of Interior DesignDocument3 pagesStudy Plan Bachelor of Interior Designjay jayNo ratings yet
- Matrikx Cto Data SheetDocument2 pagesMatrikx Cto Data Sheetjay jayNo ratings yet
- Family Care ClinicDocument23 pagesFamily Care Clinicjay jayNo ratings yet
- Sarasatr,+17 +Sajid+I+Awal+210-223Document14 pagesSarasatr,+17 +Sajid+I+Awal+210-223jay jayNo ratings yet
- NatlsocDocument9 pagesNatlsocjay jayNo ratings yet
- 2006 Publicand Private Spacein Urban AreasDocument12 pages2006 Publicand Private Spacein Urban Areasjay jayNo ratings yet
- 0733464815574094.full 2 2Document24 pages0733464815574094.full 2 2jay jayNo ratings yet
- Submitted ManuscriptDocument26 pagesSubmitted Manuscriptjay jayNo ratings yet
- Document 1Document3 pagesDocument 1jay jayNo ratings yet
- Advocate LutheranDocument4 pagesAdvocate Lutheranjay jayNo ratings yet
- Aktiviti Latihan Terapi AirDocument2 pagesAktiviti Latihan Terapi Airas-suhairiNo ratings yet
- Biology Contents - RPSC FSO by Food TecKnowDocument35 pagesBiology Contents - RPSC FSO by Food TecKnowRahul JainNo ratings yet
- Managment of Trauma Patient in ERDocument46 pagesManagment of Trauma Patient in ERtofanNo ratings yet
- Advocacy Letter-Amy JohnsDocument2 pagesAdvocacy Letter-Amy Johnsapi-239145075No ratings yet
- EPI Lecture Note April 2005, YemaneDocument132 pagesEPI Lecture Note April 2005, YemaneGetahun TekleNo ratings yet
- Pre-NEET Pediatrics Taruna MehraDocument181 pagesPre-NEET Pediatrics Taruna MehraNick Amonsull Phanuwat0% (1)
- My LogDocument229 pagesMy Logsowpij290laslNo ratings yet
- Hollow Organ InjuryDocument47 pagesHollow Organ InjuryreginaNo ratings yet
- Significance of Gulika: by Dr. Suresh Chandra Mishra, IndiaDocument10 pagesSignificance of Gulika: by Dr. Suresh Chandra Mishra, IndiaAnonymous jGdHMEODVmNo ratings yet
- 2022 - Acute Kidney Injury and Critical Care NephrologyDocument123 pages2022 - Acute Kidney Injury and Critical Care NephrologyEdson MarquesNo ratings yet
- Lab Report Exp 2 - Kidney Function & Physiology (Group 4)Document10 pagesLab Report Exp 2 - Kidney Function & Physiology (Group 4)FARHAH BATRISYIA ABDUL RAHIMNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryInternos YopalNo ratings yet
- Group 2 Case Study MergedDocument12 pagesGroup 2 Case Study MergedKobe Bryan GermoNo ratings yet
- Assignment of Pathology 401: Submitted byDocument5 pagesAssignment of Pathology 401: Submitted byaymen gulzarNo ratings yet
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- Natural Aromatase InhibitorsDocument69 pagesNatural Aromatase InhibitorsIme Muško OsječkoNo ratings yet
- Sociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilDocument8 pagesSociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilInternational Medical PublisherNo ratings yet
- Operating RoomDocument9 pagesOperating RoomMarie Ashley CasiaNo ratings yet
- An Update On Oral Human Papillomavirus Infection: Review ArticleDocument7 pagesAn Update On Oral Human Papillomavirus Infection: Review ArticlebungagladysNo ratings yet
- Cole Crops and Other Brassicas: Organic Production: AttraDocument20 pagesCole Crops and Other Brassicas: Organic Production: AttraRebecca SheaNo ratings yet
- Origin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesDocument11 pagesOrigin of The Pantaneiro Horse in Brazil: Additional Keywords Palabras Clave AdicionalesmmbasquesNo ratings yet
- Renal PediatricDocument48 pagesRenal PediatricEslam R. Almassri100% (1)
- Health Talk ExcerciseDocument5 pagesHealth Talk ExcerciseNyalen Hakom100% (1)
- Case Report 3 MukokelDocument3 pagesCase Report 3 MukokelWidychii GadiestchhetyaNo ratings yet
- Anthonela - Terán SebastiánDocument5 pagesAnthonela - Terán SebastiánJuleyssiNo ratings yet
- DissociativeidentitydisorderDocument8 pagesDissociativeidentitydisorderapi-355984916No ratings yet
- Chordal Preservation TechniquesDocument8 pagesChordal Preservation TechniquesKunwar Sidharth SaurabhNo ratings yet
- Chronic Myeloid LeukemiaDocument26 pagesChronic Myeloid LeukemiaasaleemnaNo ratings yet
- Septic Arthritis AssignmentDocument14 pagesSeptic Arthritis AssignmentDEO NDAYISABANo ratings yet