Download as pdf or txt
You might also like
- PmvbedsideevaluationDocument2 pagesPmvbedsideevaluationapi-114739487No ratings yet
- SB-930 MSDSDocument4 pagesSB-930 MSDSOana-Maria OlingherNo ratings yet
- 15 Alterations in OxygenationDocument61 pages15 Alterations in OxygenationBea Bianca CruzNo ratings yet
- CHAPTER 48 The Child With Alterations in Respiratory FunctionsDocument49 pagesCHAPTER 48 The Child With Alterations in Respiratory Functionselsaqum98No ratings yet
- Pneumonia: - It Is An Inflammation and Consolidation ofDocument44 pagesPneumonia: - It Is An Inflammation and Consolidation ofBinita ShakyaNo ratings yet
- Acute Conditions of The NeonatesDocument4 pagesAcute Conditions of The NeonatesShermina JalaniNo ratings yet
- Day 15 - NCM-109 Children With Alteration in Oxygenation (A)Document50 pagesDay 15 - NCM-109 Children With Alteration in Oxygenation (A)Sheena Patricia ArasulaNo ratings yet
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- Alterations in OxygenationDocument7 pagesAlterations in OxygenationDoña PiaNo ratings yet
- Respiratory Disorders 2.1Document70 pagesRespiratory Disorders 2.1Deenjane Nishi IgnacioNo ratings yet
- Nursing InterventionsDocument68 pagesNursing Interventionsash aliNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress SyndromedicksonsamboNo ratings yet
- BronchiolitisDocument30 pagesBronchiolitisTitusNo ratings yet
- The Child With Respiratory DysfunctionDocument91 pagesThe Child With Respiratory DysfunctionSerbanNo ratings yet
- MS RESPIbfrDocument13 pagesMS RESPIbfrEmeroot RootNo ratings yet
- WK 5 Pedi Resp - SH - SP 12Document34 pagesWK 5 Pedi Resp - SH - SP 12bibi bennyNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- Diseases of ThroatDocument39 pagesDiseases of Throatmaria jacobNo ratings yet
- Pedia Concepts 2:: From Respiratory Problems To HematologicDocument119 pagesPedia Concepts 2:: From Respiratory Problems To HematologicarudarbmeeNo ratings yet
- Case 1: Group 4Document26 pagesCase 1: Group 4John Joshua Lacson MedicineNo ratings yet
- Mwami Schools of Nursing and Midwifery: by Baldwin Hamoonga 5 Year Nursing Student (Ru) Topic: Small For Dates BabyDocument26 pagesMwami Schools of Nursing and Midwifery: by Baldwin Hamoonga 5 Year Nursing Student (Ru) Topic: Small For Dates BabyBaldwin Hamzcorp HamoongaNo ratings yet
- 3A Pneumonia With Annotations PDFDocument34 pages3A Pneumonia With Annotations PDFCathy ZapantaNo ratings yet
- Nursing Care of The Child With Respiratory DysfunctionDocument54 pagesNursing Care of The Child With Respiratory DysfunctionAlexis Coronado100% (1)
- Pediatric Asthma WordDocument4 pagesPediatric Asthma Wordraquel maniegoNo ratings yet
- Disclaimer: Christian Medical College Networked HospitalsDocument44 pagesDisclaimer: Christian Medical College Networked HospitalsJohn DorNo ratings yet
- Advance Clinical Nursing Presentation - SusanDocument40 pagesAdvance Clinical Nursing Presentation - SusanAbdul Hamid Al FarsiNo ratings yet
- Upper Respiratory Tract InfectionsDocument41 pagesUpper Respiratory Tract Infectionsmsichiliinnocent7No ratings yet
- 19 Nursing Care of A Child With Life Threatening ConditionsDocument31 pages19 Nursing Care of A Child With Life Threatening ConditionsBea Bianca CruzNo ratings yet
- PneumoniaDocument23 pagesPneumoniaAshagre MollaNo ratings yet
- Nursing Care of Children With Alterations in HealthDocument44 pagesNursing Care of Children With Alterations in HealthAmy Del Carmen50% (2)
- Pediatric Cough CMEDocument59 pagesPediatric Cough CMEkurutalaNo ratings yet
- Acute CareDocument50 pagesAcute CareFrancr ToledanoNo ratings yet
- Respiratory Distress SyndromeDocument69 pagesRespiratory Distress SyndromeAbraham ChiuNo ratings yet
- BRONCHOPNEUMONIADocument18 pagesBRONCHOPNEUMONIAMANEESH MANINo ratings yet
- Managing Illness: BY: S. Tolentino, RNDocument170 pagesManaging Illness: BY: S. Tolentino, RNSabrina TolentinoNo ratings yet
- Diseases of Neonates in AnimalsDocument35 pagesDiseases of Neonates in AnimalshansmeetNo ratings yet
- PCAP Report - Mark ReyesDocument53 pagesPCAP Report - Mark ReyesMark ReyesNo ratings yet
- Sinusitis: Rhonda Lesniak Primary Care IIDocument33 pagesSinusitis: Rhonda Lesniak Primary Care IIshyamashaNo ratings yet
- Respiratory Emergencies: Eileen Humphreys PA-C, EMT-IDocument71 pagesRespiratory Emergencies: Eileen Humphreys PA-C, EMT-IChristian JaraNo ratings yet
- Chapter 22 RespiratoryDocument33 pagesChapter 22 RespiratoryJessNo ratings yet
- Bronchiolitis FdneDocument27 pagesBronchiolitis FdneRonit ChandNo ratings yet
- Non-Infectious Respiratory ProblemDocument66 pagesNon-Infectious Respiratory ProblemSven OrdanzaNo ratings yet
- Respiratory Illnesses in ChildrenDocument42 pagesRespiratory Illnesses in ChildrenJakeNo ratings yet
- Pleural Effusion: Presented By:-Gayathri Gopakumar BSC - Nursing 2 YearDocument30 pagesPleural Effusion: Presented By:-Gayathri Gopakumar BSC - Nursing 2 YearGAYATHRI GOPAKUMARNo ratings yet
- Respiratory Distress SyndromeDocument121 pagesRespiratory Distress Syndromeinno so qtNo ratings yet
- Cardiopulmonary Disorders in ChildrenDocument65 pagesCardiopulmonary Disorders in ChildrenJohn Paul MatillosaNo ratings yet
- Chapter 4 HTDocument52 pagesChapter 4 HTtesfamichael mengistuNo ratings yet
- MSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisDocument41 pagesMSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisYAMINIPRIYANNo ratings yet
- Preterm Its ProblemsDocument30 pagesPreterm Its ProblemsEnlighten usNo ratings yet
- Bronchiectasis: by DR Haris Gul Senior Registrar Rheumatology Fauji Foundation Hospital RawalpindiDocument32 pagesBronchiectasis: by DR Haris Gul Senior Registrar Rheumatology Fauji Foundation Hospital RawalpindiAamer NaeemNo ratings yet
- Woman With PneumoniaDocument9 pagesWoman With PneumoniaNohaira SADANGNo ratings yet
- Tonsillitis and Adenoiditis: Islamic University Nursing CollegeDocument15 pagesTonsillitis and Adenoiditis: Islamic University Nursing CollegeNinaNo ratings yet
- BronchiolitisDocument29 pagesBronchiolitisMalueth AnguiNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmamaggykariuki002No ratings yet
- Powerpoint Notes - Respiratory Disorders Respiratory DisordersDocument7 pagesPowerpoint Notes - Respiratory Disorders Respiratory DisordersKareen SisonNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Pedia Pulmo 2 10.18.16Document73 pagesPedia Pulmo 2 10.18.16Medisina101No ratings yet
- Laryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandLaryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 3.5 out of 5 stars3.5/5 (2)
- Social Responses and Personality DisordersDocument50 pagesSocial Responses and Personality DisordersAYTONA, JAMAICA F.No ratings yet
- University of Southern Philippines Foundation College of Health Sciences Department of NursingDocument4 pagesUniversity of Southern Philippines Foundation College of Health Sciences Department of NursingAYTONA, JAMAICA F.No ratings yet
- MSE FormatDocument3 pagesMSE FormatAYTONA, JAMAICA F.No ratings yet
- Emotional Responses Self Protective Behaviors RevisedDocument68 pagesEmotional Responses Self Protective Behaviors RevisedAYTONA, JAMAICA F.No ratings yet
- Module 2 - Dynamics of The Aging ProcessDocument111 pagesModule 2 - Dynamics of The Aging ProcessAYTONA, JAMAICA F.No ratings yet
- Module 3 - Assessment of The Health StatusDocument43 pagesModule 3 - Assessment of The Health StatusAYTONA, JAMAICA F.No ratings yet
- NGCM 112 Course OutlineDocument7 pagesNGCM 112 Course OutlineAYTONA, JAMAICA F.No ratings yet
- Care of Client With Respiratory System DisordersDocument17 pagesCare of Client With Respiratory System DisordersAYTONA, JAMAICA F.No ratings yet
- Module 4 - Health Promotion and WellnessDocument55 pagesModule 4 - Health Promotion and WellnessAYTONA, JAMAICA F.No ratings yet
- Concept of Health & IllnessDocument26 pagesConcept of Health & IllnessAYTONA, JAMAICA F.No ratings yet
- Fluids and Electrolytes & Acid-Base BalanceDocument108 pagesFluids and Electrolytes & Acid-Base BalanceAYTONA, JAMAICA F.No ratings yet
- Hematologic DxsDocument34 pagesHematologic DxsAYTONA, JAMAICA F.No ratings yet
- Care For Clients Undergoing SurgeryDocument165 pagesCare For Clients Undergoing SurgeryAYTONA, JAMAICA F.No ratings yet
- University of Southern Philippines Foundation College of Health Sciences Department of Nursing Worksheet Title: LEOPOLD'S MANEUVERDocument2 pagesUniversity of Southern Philippines Foundation College of Health Sciences Department of Nursing Worksheet Title: LEOPOLD'S MANEUVERAYTONA, JAMAICA F.No ratings yet
- Inhaled NITRIC OXIDEDocument2 pagesInhaled NITRIC OXIDECHIERBEENo ratings yet
- Seizure ChecklistDocument3 pagesSeizure ChecklistBALIWANG, MARCOS JR. G.No ratings yet
- Position PaperDocument5 pagesPosition PaperMa JoelleNo ratings yet
- Respiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemDocument31 pagesRespiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemJay VillasotoNo ratings yet
- Confined-Space Rescue Plan 2Document17 pagesConfined-Space Rescue Plan 2patrick ruwona100% (2)
- AGE Weight (KG) Tracheal Tube ET Depth (CM at Lips) Suction Catheter (F) Laryngoscope Blade Mask Size Oral Airway Laryngeal Mask AirwayDocument2 pagesAGE Weight (KG) Tracheal Tube ET Depth (CM at Lips) Suction Catheter (F) Laryngoscope Blade Mask Size Oral Airway Laryngeal Mask AirwaySteven Okta ChandraNo ratings yet
- 코로나19 예방을 위한 응시자 준수사항 안내문 (영어 - English)Document2 pages코로나19 예방을 위한 응시자 준수사항 안내문 (영어 - English)ДарьяNo ratings yet
- Acid Base BalanceDocument69 pagesAcid Base BalanceAli AttarNo ratings yet
- CardioDocument10 pagesCardioMar OrdanzaNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument8 pagesSafety Data Sheet: 1. IdentificationJulián Herrera RestrepoNo ratings yet
- Jurnal Kep Anak PneumoniaDocument10 pagesJurnal Kep Anak PneumoniaDina AryaniNo ratings yet
- EReferralDocument31 pagesEReferralAung Phyo ThetNo ratings yet
- #2. Respiratory SymptomsDocument43 pages#2. Respiratory SymptomsDr-i BarreNo ratings yet
- CPT ChecklistDocument3 pagesCPT ChecklistMa. Angelica Alyssa RachoNo ratings yet
- Neonatal Ventilator EN NV8 V1.3Document4 pagesNeonatal Ventilator EN NV8 V1.3Surta DevianaNo ratings yet
- Assisting in Ventilator Care ProcedureDocument13 pagesAssisting in Ventilator Care ProcedureSAYMABANU100% (1)
- Upper Airway Obstruction CYP 0-16 3.0Document9 pagesUpper Airway Obstruction CYP 0-16 3.0sessaNo ratings yet
- 2LO2Document3 pages2LO2Tan SinCosNo ratings yet
- Grade 9 Module WK 1-2Document8 pagesGrade 9 Module WK 1-2Llena Grace GloryNo ratings yet
- Prosedur WSD (Water Seal Drainage)Document44 pagesProsedur WSD (Water Seal Drainage)White GooseNo ratings yet
- Diabetic Ketoacidosis DKA Acute Management ABCDEDocument10 pagesDiabetic Ketoacidosis DKA Acute Management ABCDESSNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Sotfonic SotfonicNo ratings yet
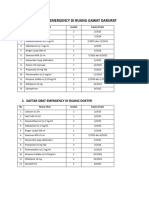
- Daftar Obat Emergency Di Ruang IgdDocument2 pagesDaftar Obat Emergency Di Ruang IgdTesa Yuli DenisaNo ratings yet
- GSRe BrochureDocument10 pagesGSRe Brochures98460No ratings yet
- EN prisma-VENT 30 40 50 68131gDocument60 pagesEN prisma-VENT 30 40 50 68131ghosp PeNo ratings yet
- What Is A LobectomyDocument6 pagesWhat Is A LobectomyMaria Carmela TormesNo ratings yet
- Lecture 2Document18 pagesLecture 2zainab ElsayedNo ratings yet
- 7biology VII Biology SECLO 2023-24 LP SecondaryDocument7 pages7biology VII Biology SECLO 2023-24 LP SecondaryGideon CavidaNo ratings yet