Download as pdf or txt
You might also like
- Patient Admission FormDocument2 pagesPatient Admission Formelmore kaka0% (1)
- FAQs For Health FacilitiesDocument17 pagesFAQs For Health FacilitiesPhilhealth ISDH SinaitNo ratings yet
- 674 - 4- Focus 3. Teacher's Book - 2020, 2nd, 325p.pdf - Google ДискDocument1 page674 - 4- Focus 3. Teacher's Book - 2020, 2nd, 325p.pdf - Google ДискДиана ШерепаNo ratings yet
- Nigerian Law School Medical Centre Bwari-Abuja Hqs Lagos, Enugu, Kano, Yenegoa and Yola Campuses Student'S Personal DataDocument2 pagesNigerian Law School Medical Centre Bwari-Abuja Hqs Lagos, Enugu, Kano, Yenegoa and Yola Campuses Student'S Personal DataIroegbu Mang John100% (1)
- Assignment Submission Form: ISB PGPMAX: Strategic Profitability Management (SPM)Document10 pagesAssignment Submission Form: ISB PGPMAX: Strategic Profitability Management (SPM)seawoodsNo ratings yet
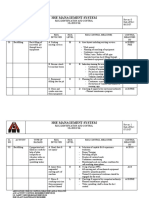
- A Risk Assessment For Interlock ExecuationDocument11 pagesA Risk Assessment For Interlock ExecuationZubair Khan100% (1)
- Medical CertificateDocument1 pageMedical CertificateRosario Perez OcamiaNo ratings yet
- Creating Miracles Everyday, Richard CarlsonDocument122 pagesCreating Miracles Everyday, Richard Carlsoncristian cerolimiteNo ratings yet
- A Clinical Pathway For Complete Immediate Denture TherapyDocument18 pagesA Clinical Pathway For Complete Immediate Denture TherapyPragya PandeyNo ratings yet
- EKONSULTA FormDocument13 pagesEKONSULTA FormJirhana Lindagan Karon-KampangNo ratings yet
- Republic of The Philippines Province of Rizal Medical-Dental Health ServicesDocument1 pageRepublic of The Philippines Province of Rizal Medical-Dental Health ServicesCes ReyesNo ratings yet
- Odisha Joint Entrance Examination: Online Document Verification CertificateDocument1 pageOdisha Joint Entrance Examination: Online Document Verification Certificatebibhuti bhusan routNo ratings yet
- Student Medical DeclarationDocument1 pageStudent Medical DeclarationDandreb Magnaye AliasNo ratings yet
- Hospital Health Information Management Manual, PrintableDocument88 pagesHospital Health Information Management Manual, PrintableMarie Bernadette AresNo ratings yet
- Request For School Clearance FormDocument1 pageRequest For School Clearance FormJam Uly GastyNo ratings yet
- Family Health Optima Insurance Plan NewDocument8 pagesFamily Health Optima Insurance Plan NewNeeraj NemaNo ratings yet
- School Form 10 Sf10 FormatDocument8 pagesSchool Form 10 Sf10 FormatARLENENo ratings yet
- Proposal @2022Document45 pagesProposal @2022Kidima100% (2)
- PMLS Narrative Report PDFDocument14 pagesPMLS Narrative Report PDFGilmar ManzanoNo ratings yet
- Bhagwant University, Ajmer: BURET - 2018 Application FormDocument3 pagesBhagwant University, Ajmer: BURET - 2018 Application FormVinod JagdaleNo ratings yet
- Student Profile FinalDocument4 pagesStudent Profile Finaljaythakar88870% (1)
- School Clinic Visit Form: Wakat National High School Wakat, Barobo, SDSDocument1 pageSchool Clinic Visit Form: Wakat National High School Wakat, Barobo, SDSAivee Tigol Judilla GulleNo ratings yet
- Students Feedback Form LaboratoryDocument2 pagesStudents Feedback Form LaboratoryRonald Candy LasatenNo ratings yet
- Payment Agreement PDFDocument1 pagePayment Agreement PDFLisa HalajkoNo ratings yet
- Diploma Engg Pre-QualifierDocument6 pagesDiploma Engg Pre-QualifierhoddceNo ratings yet
- Referral Form Jessa 2021Document1 pageReferral Form Jessa 2021Jessa MaeNo ratings yet
- Attendance Sheet For PRC CPD ActivityDocument2 pagesAttendance Sheet For PRC CPD ActivityFitz Jaminit100% (1)
- Senior High School Registration FormDocument1 pageSenior High School Registration FormBernard LuisagaNo ratings yet
- 2019 Medical Certificate1Document5 pages2019 Medical Certificate1lea bendijoNo ratings yet
- Pregnancy Test CertificateDocument1 pagePregnancy Test CertificateMae GallimbasNo ratings yet
- HealthPoint Registration EnglishDocument6 pagesHealthPoint Registration EnglishAnastasia KassaNo ratings yet
- Form 6 LEAVE DeoganiDocument2 pagesForm 6 LEAVE DeoganiDeogani GarguenaNo ratings yet
- Form No NTC 1-01 APPLICATION FOR RADIO OPERATOR EXAMINATIONDocument1 pageForm No NTC 1-01 APPLICATION FOR RADIO OPERATOR EXAMINATIONMa. Angela De GuzmanNo ratings yet
- Request For 1st Sem Grade-2019Document1 pageRequest For 1st Sem Grade-2019Rushid Jay Samortin SanconNo ratings yet
- School Health Examination CardDocument3 pagesSchool Health Examination Cardjrose fay amatNo ratings yet
- Shs Enrollment Form Sy 2022-2023Document2 pagesShs Enrollment Form Sy 2022-2023Sophia Erika Largo0% (1)
- Annex 3A JDVP List of Excluded Learners (Edited)Document1 pageAnnex 3A JDVP List of Excluded Learners (Edited)ジナNo ratings yet
- Health Declaration Form: Golden Gate Subd. Talon III, Las Piñas City / Tel. No. 8986-8763Document2 pagesHealth Declaration Form: Golden Gate Subd. Talon III, Las Piñas City / Tel. No. 8986-8763Jha Jha CaLvezNo ratings yet
- EstabPtMedHistory FILLABLEDocument3 pagesEstabPtMedHistory FILLABLEChristinah Tamby LewanikaNo ratings yet
- 2.physical E, HISTORY NCPDocument13 pages2.physical E, HISTORY NCPمريم حجيNo ratings yet
- HSU Pre-Enrollment Medical Record Form (FRESHMAN)Document4 pagesHSU Pre-Enrollment Medical Record Form (FRESHMAN)ChristnerNo ratings yet
- Student Health Services Form 2020Document2 pagesStudent Health Services Form 2020Asiaui HendersonNo ratings yet
- Natoza Medical Form For Grade 7 12Document3 pagesNatoza Medical Form For Grade 7 12Deonna AngelineNo ratings yet
- Net Health FormDocument9 pagesNet Health FormrogeliocszNo ratings yet
- New Patient Information FormDocument4 pagesNew Patient Information FormmajungNo ratings yet
- Student Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415Document4 pagesStudent Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415JohnNo ratings yet
- Medical History Form and Physicians Report For SHS and College StudentsDocument2 pagesMedical History Form and Physicians Report For SHS and College StudentsKimNo ratings yet
- Student Medical FormDocument6 pagesStudent Medical FormLOMAS MOTILALNo ratings yet
- PA 1 1 MergedDocument9 pagesPA 1 1 MergedMarc Mhel DalipeNo ratings yet
- Health DeclarationDocument2 pagesHealth Declarationrosabelromero09No ratings yet
- Physician Certification Form 080814Document5 pagesPhysician Certification Form 080814Jeff WilliamsNo ratings yet
- RCESS-HD by PICEDocument2 pagesRCESS-HD by PICEBea ReyesNo ratings yet
- UHS Pre-Enrolment Physical Examination Report Form (FILLABLE)Document2 pagesUHS Pre-Enrolment Physical Examination Report Form (FILLABLE)Guillermo PantuhanNo ratings yet
- (PSU-F-CLI-04) Student Health Record PDFDocument2 pages(PSU-F-CLI-04) Student Health Record PDFbhelle ValenciaNo ratings yet
- Health Declaration ANNEX CDocument2 pagesHealth Declaration ANNEX CJhaylourd BonggotNo ratings yet
- Health Declaration Form: University of The Philipines Visayas Health Service Unit Miagao, IloiloDocument2 pagesHealth Declaration Form: University of The Philipines Visayas Health Service Unit Miagao, IloiloMonique DianeNo ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- Med FormDocument3 pagesMed FormWsu CampusHousingNo ratings yet
- New Patient FormDocument5 pagesNew Patient Formgel.rmerNo ratings yet
- Ndicott Ollege: Ealth OrmDocument4 pagesNdicott Ollege: Ealth Ormramon_huescaNo ratings yet
- Case History FormDocument5 pagesCase History FormbhawmaNo ratings yet
- Health History FormDocument4 pagesHealth History Formganesh chowdaryNo ratings yet
- Up Form No2Document2 pagesUp Form No2Mitch Elle InfanteNo ratings yet
- Family Case ReportDocument7 pagesFamily Case ReportMOHANTA, deviprasadNo ratings yet
- PA Tool Revised 2019 111Document24 pagesPA Tool Revised 2019 111Markus BuliganNo ratings yet
- Risk Assessment of BackfillingDocument2 pagesRisk Assessment of BackfillingPrasanta ParidaNo ratings yet
- CHN FinalDocument41 pagesCHN FinalKeziah Marie Chua Santa-AnaNo ratings yet
- Maintenance Manual CH420-01 - MM - S223.516.en-03Document196 pagesMaintenance Manual CH420-01 - MM - S223.516.en-03Benjamin MurphyNo ratings yet
- Alamillo Vs Cleene Maritime PPDocument27 pagesAlamillo Vs Cleene Maritime PPHeart LeroNo ratings yet
- Cast Partial Denture With Attachment Boon To PreveDocument7 pagesCast Partial Denture With Attachment Boon To PreveMamta SentaNo ratings yet
- Methods: Ian Zelko BS, Zach Zylstra BSDocument1 pageMethods: Ian Zelko BS, Zach Zylstra BSIan ZelkoNo ratings yet
- 100 Items QuestionsDocument22 pages100 Items Questionsdianneako100% (1)
- Health Technology Assessment (HTA) GuidelineDocument163 pagesHealth Technology Assessment (HTA) Guidelinebella friscaamaliaNo ratings yet
- Richard Kradin - The Placebo Response and The Power of Unconscious Healing-Routledge (2008) PDFDocument296 pagesRichard Kradin - The Placebo Response and The Power of Unconscious Healing-Routledge (2008) PDFCamelia Teodora BuneaNo ratings yet
- Elaine Cristine de Azevedo Arruda - Povoa - CVDocument1 pageElaine Cristine de Azevedo Arruda - Povoa - CVElaine ArrudaNo ratings yet
- 365 Days of Self Care BLANK 1Document9 pages365 Days of Self Care BLANK 1alioliver9No ratings yet
- TEC-030100.2-MET-DoR-003-MAT-TDS-BASF-Concresive 1414Document3 pagesTEC-030100.2-MET-DoR-003-MAT-TDS-BASF-Concresive 1414Eli MatucadNo ratings yet
- Eyewitness Testimony.Document6 pagesEyewitness Testimony.anorus97No ratings yet
- 11 Key Areas of Responsibilities of NursingDocument2 pages11 Key Areas of Responsibilities of NursingHilario. Hayascent.Reign.M.No ratings yet
- Maintenance of Records and ReportsDocument81 pagesMaintenance of Records and ReportsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- Atenolol Oral Suspension 2mg/mLDocument1 pageAtenolol Oral Suspension 2mg/mLChemistixNo ratings yet
- Tooth Implant Supported Prosthesis: A Literature ReviewDocument8 pagesTooth Implant Supported Prosthesis: A Literature ReviewTung Thanh NguyenNo ratings yet
- ResumeDocument2 pagesResumeapi-503876999No ratings yet
- DYP Induction BookletDocument24 pagesDYP Induction BookletdypcopakurdipuneNo ratings yet
- Technical Data Sheet Jazeera Epo-Rich Primer JI-61005: DescriptionDocument3 pagesTechnical Data Sheet Jazeera Epo-Rich Primer JI-61005: DescriptionSyedFarhanNo ratings yet
- Adult Cognitive AssessmentDocument15 pagesAdult Cognitive AssessmentClaudia Delia Foltun0% (2)
- Narayan Hrudalaya Case Study AnalysisDocument5 pagesNarayan Hrudalaya Case Study Analysisdarshak kansagraNo ratings yet
- Assessment Tool SITXINV002 Maint Perishable ItemsDocument36 pagesAssessment Tool SITXINV002 Maint Perishable ItemsAnnu SarochNo ratings yet
- "Cooper Pharmaceutical" Case Submission: Submitted For Sales and Distribution Management - MKT 6009 byDocument5 pages"Cooper Pharmaceutical" Case Submission: Submitted For Sales and Distribution Management - MKT 6009 byshubhamsd3No ratings yet
- 10 Diagnosa Terbesar BPJSDocument2 pages10 Diagnosa Terbesar BPJSMutemjNo ratings yet