Download as docx, pdf, or txt
You might also like
- Nursing Care Plan FormatDocument1 pageNursing Care Plan FormatRose Camille Delos Santos DatuinNo ratings yet
- Nursing Care Plan (Clinical Portrait)Document2 pagesNursing Care Plan (Clinical Portrait)Dann Francis SarnilloNo ratings yet
- Clozapine Drug StudyDocument2 pagesClozapine Drug Studymilkv100% (8)
- Unusual Presentation of May-Thurner SyndromeDocument5 pagesUnusual Presentation of May-Thurner SyndromeJ. Ruben HermannNo ratings yet
- DR FormsDocument3 pagesDR FormsDianne LabisNo ratings yet
- DR Form BsuDocument1 pageDR Form BsumingcatNo ratings yet
- Ordr MemoDocument5 pagesOrdr MemoApril Rose Sebial GalvezNo ratings yet
- Handle DR 1Document1 pageHandle DR 1Llys MondejarNo ratings yet
- Updated Case Slip 2022Document6 pagesUpdated Case Slip 2022Jhennie Rose PalaganasNo ratings yet
- Assisisted 1Document1 pageAssisisted 1Llys MondejarNo ratings yet
- NURSING CARE PLAN TemplateDocument2 pagesNURSING CARE PLAN TemplateK.A.ANo ratings yet
- University of La Salette Major Cases: Bachelor St.,Dubinan East, Santiago CityDocument5 pagesUniversity of La Salette Major Cases: Bachelor St.,Dubinan East, Santiago Citynina grace joyNo ratings yet
- Redoble Medical Clinic Case NoDocument1 pageRedoble Medical Clinic Case Noapi-3836762No ratings yet
- Case Slip CPH ORDocument1 pageCase Slip CPH ORKisha PalmesNo ratings yet
- Obstetric Assessment ToolDocument5 pagesObstetric Assessment ToolDudil GoatNo ratings yet
- Surgical Delivery SlipDocument5 pagesSurgical Delivery SlipCkaye GansubinNo ratings yet
- Handle: Notre Dame of Midsayap College College of NursingDocument6 pagesHandle: Notre Dame of Midsayap College College of NursingLouisa CabañogNo ratings yet
- Christ The King College: 9014 Gingoog City Philippines Nursing ProgramDocument4 pagesChrist The King College: 9014 Gingoog City Philippines Nursing ProgramMelisande Rae CiruelaNo ratings yet
- Mouth Assess FormDocument3 pagesMouth Assess FormAngelo Dela CruzNo ratings yet
- Surgical SlipDocument1 pageSurgical SlipTeanu Jose Gabrillo TamayoNo ratings yet
- CS FORM 86 Medical CertificateDocument2 pagesCS FORM 86 Medical CertificateCatleah ZamoraNo ratings yet
- CaseloadDocument3 pagesCaseloadJayson Mherl GonzalesNo ratings yet
- Abdullah Medical Center & Maternity Home: Gynecological Ultrasound ExaminationDocument1 pageAbdullah Medical Center & Maternity Home: Gynecological Ultrasound ExaminationZain TabishNo ratings yet
- Med School-Hrs DR Par SignDocument1 pageMed School-Hrs DR Par Signapi-218407689No ratings yet
- 2018 WSRDocument1 page2018 WSR2ncnz6999mNo ratings yet
- STI - Oncall FormDocument1 pageSTI - Oncall Formdjanggo18No ratings yet
- Cord Care Case Slip - Lorma CollegesDocument1 pageCord Care Case Slip - Lorma CollegesJet BautistaNo ratings yet
- CS FORM 86 Medical Certificate 1Document2 pagesCS FORM 86 Medical Certificate 1BECHIEL ANGELIE CA�EDONo ratings yet
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- NCPDocument2 pagesNCPMikee BoomNo ratings yet
- SURGERY 1 Daily Monitoring SheetDocument1 pageSURGERY 1 Daily Monitoring SheetKrishna Faith P. DelaraNo ratings yet
- Or and DR New FormDocument8 pagesOr and DR New FormAlfred BucabucaNo ratings yet
- Referral Form-1Document1 pageReferral Form-1harie82No ratings yet
- NurcingDocument2 pagesNurcingJessica MedinaNo ratings yet
- KARDEXDocument4 pagesKARDEXJemuel DalanaNo ratings yet
- FORM 86 Annual Health RecordsDocument1 pageFORM 86 Annual Health RecordsCHARMAINE GRACE BALUTANNo ratings yet
- new-REINSTATEMENT-FORMDocument1 pagenew-REINSTATEMENT-FORMDesiree Rosete Beringa-CaasiNo ratings yet
- Caseload Caseslip For DR and OR UpdatedDocument5 pagesCaseload Caseslip For DR and OR UpdatedCarissa Mae Tapec EstradaNo ratings yet
- NCP FormatDocument2 pagesNCP Formatraul_bsuNo ratings yet
- Clinical PathwayyDocument1 pageClinical PathwayyGEN COLLANTESNo ratings yet
- Record of Newborn CareDocument1 pageRecord of Newborn CareMarie Antionette MondragonNo ratings yet
- Two Way Health Referral FormDocument1 pageTwo Way Health Referral FormKristine TanNo ratings yet
- Self Declaration FormDocument1 pageSelf Declaration FormAvritti MishraNo ratings yet
- Toddler Assessment GuideDocument1 pageToddler Assessment GuidepetalcorinaltheaNo ratings yet
- KARDEXDocument4 pagesKARDEXDaniel GalitzineNo ratings yet
- CHS Case NotebookDocument33 pagesCHS Case NotebookrigasanaorayNo ratings yet
- REFERRALDocument1 pageREFERRALNether MonsterNo ratings yet
- STI - Minor/majorcase FormDocument2 pagesSTI - Minor/majorcase Formsticdo_nursing2011No ratings yet
- Geriatrics AssesmentbysedgeDocument4 pagesGeriatrics Assesmentbysedgephysio115No ratings yet
- Circulating Case Slip: Name of Student Student NumberDocument12 pagesCirculating Case Slip: Name of Student Student NumberEugenio Roque Casaclang De Leon IiiNo ratings yet
- Csu, Stanislaus Mental Health Nursing Plan of Care: Date Lab Test Patient Value Normal Value Nursing ImplicationsDocument1 pageCsu, Stanislaus Mental Health Nursing Plan of Care: Date Lab Test Patient Value Normal Value Nursing ImplicationsCarlaNo ratings yet
- Medical Evaluation Form For PAPsDocument4 pagesMedical Evaluation Form For PAPsPrint Media Printing pressNo ratings yet
- Assessment Guide ToddlerDocument2 pagesAssessment Guide ToddlerOla Anna GamutinNo ratings yet
- PRC Form HTUDocument5 pagesPRC Form HTUEduardNo ratings yet
- DrugDocument40 pagesDrugNiflheimr ExcelsiNo ratings yet
- PRC Form of New Curri (Odc Form 1a)Document5 pagesPRC Form of New Curri (Odc Form 1a)Angeline Fajardo de LeonNo ratings yet
- Newborn Screening Continuity Clinic Initial Consult Form Ncr/MimaropaDocument3 pagesNewborn Screening Continuity Clinic Initial Consult Form Ncr/Mimaropajacqueline licupNo ratings yet
- Medical Certificate TemplateDocument1 pageMedical Certificate TemplateBarbyjean Boiser Demetita100% (1)
- Medical Certificate TemplateDocument1 pageMedical Certificate TemplateAnonymous HNHtkiGRjINo ratings yet
- Medical Certificate TemplateDocument1 pageMedical Certificate TemplateAnonymous HNHtkiGRjINo ratings yet
- Matapos Maitatag Ang Kalayaan NG Pilipinas Noong 1946Document4 pagesMatapos Maitatag Ang Kalayaan NG Pilipinas Noong 1946Dianne LabisNo ratings yet
- Ready To Go LyricsdocxDocument1 pageReady To Go LyricsdocxDianne Labis100% (2)
- Essential Intrapartum and Newborn CareDocument7 pagesEssential Intrapartum and Newborn CareDianne LabisNo ratings yet
- LFD Blank FormDocument2 pagesLFD Blank FormDianne LabisNo ratings yet
- CHN Journal PrelimDocument2 pagesCHN Journal PrelimDianne LabisNo ratings yet
- Family ProfileDocument5 pagesFamily ProfileDianne LabisNo ratings yet
- NGT VillarealDocument5 pagesNGT VillarealDianne LabisNo ratings yet
- Leopolds Maneuver - LabisDocument2 pagesLeopolds Maneuver - LabisDianne LabisNo ratings yet
- Ivf NiceDocument22 pagesIvf NiceDianne LabisNo ratings yet
- Essential Newborn CareDocument3 pagesEssential Newborn CareDianne LabisNo ratings yet
- Conduct of Normal LaborDocument1 pageConduct of Normal LaborDianne LabisNo ratings yet
- Essential Intrapartum and Newborn CareDocument6 pagesEssential Intrapartum and Newborn CareDianne LabisNo ratings yet
- Fernando Final G&DDocument9 pagesFernando Final G&DDianne LabisNo ratings yet
- STS Learning Activity PackageDocument38 pagesSTS Learning Activity PackageDianne LabisNo ratings yet
- Assisting in Intravenous Infusion NewDocument52 pagesAssisting in Intravenous Infusion NewDianne LabisNo ratings yet
- DR FormsDocument3 pagesDR FormsDianne LabisNo ratings yet
- A&B-WPS OfficeDocument9 pagesA&B-WPS OfficeDianne LabisNo ratings yet
- CATHETERIZATION VillarealDocument6 pagesCATHETERIZATION VillarealDianne LabisNo ratings yet
- Conduct-Of-Normal-Labor - LABISDocument2 pagesConduct-Of-Normal-Labor - LABISDianne LabisNo ratings yet
- ADRGROWTHANDEVELOPMENTDocument9 pagesADRGROWTHANDEVELOPMENTDianne LabisNo ratings yet
- Assisting in Intravenous Infusion NewDocument52 pagesAssisting in Intravenous Infusion NewDianne LabisNo ratings yet
- Assisting Iv InfusionDocument3 pagesAssisting Iv InfusionDianne LabisNo ratings yet
- Letter For My Future SelfDocument1 pageLetter For My Future SelfDianne LabisNo ratings yet
- History Contributions: Richly Glenn Bagongon Bsit 2ADocument37 pagesHistory Contributions: Richly Glenn Bagongon Bsit 2ADianne LabisNo ratings yet
- BshrehrthhrtDocument2 pagesBshrehrthhrtDianne LabisNo ratings yet
- Swimming Is An Individual or Team Racing Sport That Requires The Use of OneDocument1 pageSwimming Is An Individual or Team Racing Sport That Requires The Use of OneDianne LabisNo ratings yet
- Sts Scanned BookDocument190 pagesSts Scanned BookDianne LabisNo ratings yet
- Artapp 1Document40 pagesArtapp 1Dianne LabisNo ratings yet
- The Basic Process of Gene Therapy Erica GDocument2 pagesThe Basic Process of Gene Therapy Erica GDianne LabisNo ratings yet
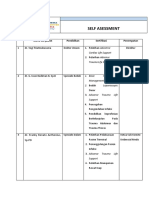
- Self Asessment: Nama Karyawan Pendidikan Sertifikasi PenempatanDocument8 pagesSelf Asessment: Nama Karyawan Pendidikan Sertifikasi PenempatanRora Dhe OlalaNo ratings yet
- International Journal of Health Care Quality Assurance: Article InformationDocument11 pagesInternational Journal of Health Care Quality Assurance: Article InformationSabin LalNo ratings yet
- C.V. Dr. VipinDocument10 pagesC.V. Dr. VipinVipin Arora0% (1)
- Vice Chancellor DR NTR University of Health Sciences VijayawadaDocument3 pagesVice Chancellor DR NTR University of Health Sciences Vijayawadabrunda maneepuriNo ratings yet
- JADA Ethical and Legal Issues in NutritionDocument10 pagesJADA Ethical and Legal Issues in NutritionDawn ThunderNo ratings yet
- VET RESUME 4pgs (KALAHI DUMATTIC BIWIT)Document4 pagesVET RESUME 4pgs (KALAHI DUMATTIC BIWIT)Sicat Mark BantiyanNo ratings yet
- Application Form Birthing HomeDocument5 pagesApplication Form Birthing HomeKian AlfrzNo ratings yet
- List of Candidates Applied For MBBS-BDS Course-2012Document39 pagesList of Candidates Applied For MBBS-BDS Course-2012Elcita Rose AntoNo ratings yet
- Referral Slip BlueDocument2 pagesReferral Slip BlueGerald TalledoNo ratings yet
- JOB RESPONSIBILITIES OF CHOs AT HWCsDocument4 pagesJOB RESPONSIBILITIES OF CHOs AT HWCsMallappa OdomaneNo ratings yet
- Good-Pharmacy-Practice Certificate of Achievement DvyjlbbDocument2 pagesGood-Pharmacy-Practice Certificate of Achievement Dvyjlbbparwana formuliNo ratings yet
- Trust Doctor in Joint Reconstruction and Sarcoma Job Description Trust ProfileDocument9 pagesTrust Doctor in Joint Reconstruction and Sarcoma Job Description Trust ProfileDaniyal AzmatNo ratings yet
- Retailer ListDocument8 pagesRetailer ListRahul SakateNo ratings yet
- IPC Program of WorksDocument5 pagesIPC Program of WorksElmira MalaboNo ratings yet
- Anna Faust Resume 2021Document2 pagesAnna Faust Resume 2021api-581442452No ratings yet
- Business Ethics FinalDocument11 pagesBusiness Ethics FinalRubi MahatoNo ratings yet
- CHN PRELIM Quiz 1 (2011)Document5 pagesCHN PRELIM Quiz 1 (2011)Amiel Francisco ReyesNo ratings yet
- BSN ResumeDocument7 pagesBSN Resumed0t1f1wujap3100% (2)
- Endovascular Aortic Aneurysm Repair (EVAR)Document5 pagesEndovascular Aortic Aneurysm Repair (EVAR)D FNo ratings yet
- 2022 Article 2042Document21 pages2022 Article 2042Yulita Fitria sariNo ratings yet
- TraumaDocument16 pagesTraumaAnzala KhanNo ratings yet
- AL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteDocument2 pagesAL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteJazzmine C. RubricoNo ratings yet
- Manulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enDocument14 pagesManulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enSara AdelNo ratings yet
- Role of Digital Therapeutics and The Changing Future of HealthcareDocument7 pagesRole of Digital Therapeutics and The Changing Future of HealthcareDavy DaveNo ratings yet
- MEDICAL RECORD 2020 (Pre Employment)Document18 pagesMEDICAL RECORD 2020 (Pre Employment)Jb TiscubNo ratings yet
- Chapter-4 PHPDocument9 pagesChapter-4 PHPgamingw470No ratings yet
- (Reduced) 24th BaSS PREFINAL Program 2019Document36 pages(Reduced) 24th BaSS PREFINAL Program 2019Vera Radojkova NikolovskaNo ratings yet
- The State of The County Address 2015Document153 pagesThe State of The County Address 2015api-245299850No ratings yet
- Nhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaDocument1 pageNhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaPazNo ratings yet