Download as pdf or txt
You might also like
- Aqa A Level Biology p1 QPDocument36 pagesAqa A Level Biology p1 QPJaden MistryNo ratings yet
- (Cambridge Manuals in Archaeology) R Lee Lyman-Vertebrate Taphonomy-Cambridge University Press (1994)Document549 pages(Cambridge Manuals in Archaeology) R Lee Lyman-Vertebrate Taphonomy-Cambridge University Press (1994)Danny Florest100% (3)
- CArolina S. AGRAvanteDocument37 pagesCArolina S. AGRAvanteEllain CaballeroNo ratings yet
- Physics: FlashbackDocument2 pagesPhysics: FlashbackWonderlapseNo ratings yet
- امتحانات الكترونيه PDFDocument10 pagesامتحانات الكترونيه PDFAli AhmedNo ratings yet
- Barracuda SantosDocument238 pagesBarracuda Santoscasadosparafusos.jsNo ratings yet
- 39760Document4 pages39760RUMBIDZAI MARAWANo ratings yet
- Turunkan Kolesterol Anda: Disarikan Dari Sumber Di Internet AWM ForeverDocument24 pagesTurunkan Kolesterol Anda: Disarikan Dari Sumber Di Internet AWM ForeverGias Maheyssa AmarullahNo ratings yet
- 6 RX 6 Rs 6 SRDocument4 pages6 RX 6 Rs 6 SRMark J AbarracosoNo ratings yet
- Introduction HandoutDocument3 pagesIntroduction Handoutathenalavega100% (1)
- Anatomic Sciences EDITDocument214 pagesAnatomic Sciences EDITreviewer.email001No ratings yet
- Fizika M 2015Document19 pagesFizika M 2015Dachi VartagavaNo ratings yet
- List ContactsDocument9 pagesList ContactsrobertthomaswhiteNo ratings yet
- Manual TsoDocument33 pagesManual TsoFrancisco de Assis Domingos PenhaNo ratings yet
- BS 4659 1989 Specification For Tool and Die SteelsDocument22 pagesBS 4659 1989 Specification For Tool and Die SteelsLeon MarcoNo ratings yet
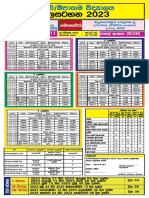
- Pasal Time Table MPV Banner 2023Document1 pagePasal Time Table MPV Banner 20233MANANo ratings yet
- Produktdatenblatt BIKUTEC V60Document1 pageProduktdatenblatt BIKUTEC V60stebeb800No ratings yet
- Intuitionistic Logic Constructive LogicDocument13 pagesIntuitionistic Logic Constructive Logic'Prasada WedatamaNo ratings yet
- 24 Z Pan PDFDocument7 pages24 Z Pan PDFhimamahanNo ratings yet
- قانون ضریبة الدخلDocument58 pagesقانون ضریبة الدخلJCPAJONo ratings yet
- T T T T: Scanned by CamscannerDocument24 pagesT T T T: Scanned by CamscannerTriveniTammuNo ratings yet
- Productivity RatesDocument2 pagesProductivity RatesAnonymous M6O8URiNo ratings yet
- Alsun Floordeck FD-1000Document4 pagesAlsun Floordeck FD-1000Teknik produksi wikonNo ratings yet
- and 55011 Conducted EmissionsDocument21 pagesand 55011 Conducted EmissionssnfulNo ratings yet
- قانون الضریبة العامة علی المبیعاتDocument88 pagesقانون الضریبة العامة علی المبیعاتJCPAJONo ratings yet
- Brosur Mini BankerDocument2 pagesBrosur Mini BankerRama Asmara TariganNo ratings yet
- PDF New Makalah Krisis Hipertensi CompressDocument22 pagesPDF New Makalah Krisis Hipertensi CompressLionel IboyNo ratings yet
- Compare Mineral WaterDocument1 pageCompare Mineral WaterDanang NCONo ratings yet
- Rotated 61000-4-11 Immunity To Ac Supply Dips Dropouts InterruptionsDocument13 pagesRotated 61000-4-11 Immunity To Ac Supply Dips Dropouts InterruptionsShawn DeolNo ratings yet
- Analysis of Molybdenite Bioleaching by Thiobacillus Ferrooxidans in The Absence of Iron (Ii)Document6 pagesAnalysis of Molybdenite Bioleaching by Thiobacillus Ferrooxidans in The Absence of Iron (Ii)kmirjaliliNo ratings yet
- MenuDocument1 pageMenudwi mutiaNo ratings yet
- Reactor: UDC 621.039.534.44:620.193o23Document5 pagesReactor: UDC 621.039.534.44:620.193o23sum74316No ratings yet
- Lao Phrasebook PDFDocument159 pagesLao Phrasebook PDFAmido Hernan Rios OvalleNo ratings yet
- The REG Procedure Model: MODEL1 Dependent Variable: y The REG Procedure Model: MODEL1 Dependent Variable: yDocument4 pagesThe REG Procedure Model: MODEL1 Dependent Variable: y The REG Procedure Model: MODEL1 Dependent Variable: yveechowNo ratings yet
- MAS P Math1 March2545Document10 pagesMAS P Math1 March2545rtafa qaNo ratings yet
- Aniı Isis PDocument42 pagesAniı Isis PNubia Alejandro HernandezNo ratings yet
- Control SystemsDocument39 pagesControl SystemsKrushnasamy SuramaniyanNo ratings yet
- Contribution Breakdown Graduation and JSDocument5 pagesContribution Breakdown Graduation and JSRussell SanicoNo ratings yet
- Labour Productivity and Rate AnalysisDocument6 pagesLabour Productivity and Rate AnalysisGanesh Un100% (1)
- A Practical Guide For EN 61000-3-3 and EN 61000-3-11 - Electromagnetic CompatibilityDocument15 pagesA Practical Guide For EN 61000-3-3 and EN 61000-3-11 - Electromagnetic CompatibilityanilNo ratings yet
- 3GS BrochureDocument3 pages3GS BrochureIsaac Joshua EscañoNo ratings yet
- Jeep WJ 2000Document220 pagesJeep WJ 2000djgibus0% (1)
- Indore Presentation - 23.02.15Document48 pagesIndore Presentation - 23.02.15arthiarulNo ratings yet
- Et Al. Macaca Fascicularis: 0 1 O0 200 3 O0 I I I 30Document1 pageEt Al. Macaca Fascicularis: 0 1 O0 200 3 O0 I I I 30AkicaNo ratings yet
- Labour OutputDocument9 pagesLabour Outputanand_parchureNo ratings yet
- TUGAS DATA MINING NadyaDocument7 pagesTUGAS DATA MINING Nadyahanny davNo ratings yet
- 1 EstrellitaDocument2 pages1 EstrellitaAgustín GonzálezNo ratings yet
- Bey A2 VocabEx Wsh2Document1 pageBey A2 VocabEx Wsh2Wayra BANo ratings yet
- Modifiwd Zoology MSC Vsu SyllabusDocument30 pagesModifiwd Zoology MSC Vsu SyllabusNarasimha MurthyNo ratings yet
- موجودی بازی خارجی 29 خردادDocument4 pagesموجودی بازی خارجی 29 خردادfardad shirinichNo ratings yet
- T 3 H M M K 7: TT T T T T T TDocument4 pagesT 3 H M M K 7: TT T T T T T Tmohdwajid2009No ratings yet
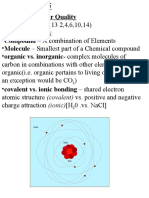
- Chapter 4 - Water Quality: ElectronDocument14 pagesChapter 4 - Water Quality: ElectronshrutiNo ratings yet
- Science Paper MT 1Document4 pagesScience Paper MT 1Rashmi MAAM 748No ratings yet
- Windsurfing: 1 Look, Find and Circle. Then Look and Find Other English Words You KnowDocument17 pagesWindsurfing: 1 Look, Find and Circle. Then Look and Find Other English Words You KnowJesús Box Soler100% (1)
- Machine DesignDocument463 pagesMachine DesignReymart Ebora100% (4)
- T" Ii M', N, I I Tlilltll: Isothermal Treatment OF AlloyDocument3 pagesT" Ii M', N, I I Tlilltll: Isothermal Treatment OF AlloySinhro018No ratings yet
- Redspot Physics 1000 MCQsDocument258 pagesRedspot Physics 1000 MCQsAndrew NyanhowoNo ratings yet
- Jadavp Ur Univ Ersit Y Dec Ent Ralized V Acant S E at Mat Rix (Se at S Offered According T O Wbjee-2 019 Rank)Document1 pageJadavp Ur Univ Ersit Y Dec Ent Ralized V Acant S E at Mat Rix (Se at S Offered According T O Wbjee-2 019 Rank)Lakkhi ShawNo ratings yet
- AndDocument1 pageAndzyrussiNo ratings yet
- 2024 - 03 - 00 Globa LaviatorDocument78 pages2024 - 03 - 00 Globa Laviator9g694mq27fNo ratings yet
- Problem Set in Boyle: 1 L G WHDocument1 pageProblem Set in Boyle: 1 L G WHKENT 45No ratings yet
- LESSON 01 ANSWER SHEET - Caballero, Ellain C.Document2 pagesLESSON 01 ANSWER SHEET - Caballero, Ellain C.Ellain CaballeroNo ratings yet
- Peste KaDocument1 pagePeste KaEllain CaballeroNo ratings yet
- Lesson 01 Answer SheetDocument2 pagesLesson 01 Answer SheetEllain CaballeroNo ratings yet
- HeragestDocument1 pageHeragestEllain CaballeroNo ratings yet
- PravazDocument1 pagePravazEllain CaballeroNo ratings yet
- ZeptrigenDocument1 pageZeptrigenEllain CaballeroNo ratings yet
- FunxionDocument1 pageFunxionEllain CaballeroNo ratings yet
- ZoldemDocument1 pageZoldemEllain CaballeroNo ratings yet
- Solmux Adult Suspension PILDocument1 pageSolmux Adult Suspension PILEllain CaballeroNo ratings yet
- SoniphenDocument1 pageSoniphenEllain CaballeroNo ratings yet
- Plogrel 799Document1 pagePlogrel 799Ellain CaballeroNo ratings yet
- LovorinDocument1 pageLovorinEllain CaballeroNo ratings yet
- Rythma IVDocument1 pageRythma IVEllain CaballeroNo ratings yet
- Montra 966Document1 pageMontra 966Ellain CaballeroNo ratings yet
- Bill of RightsDocument37 pagesBill of RightsEllain CaballeroNo ratings yet
- Zenith TabletDocument1 pageZenith TabletEllain CaballeroNo ratings yet
- MeropDocument1 pageMeropEllain CaballeroNo ratings yet
- Zyra Front PageDocument3 pagesZyra Front PageEllain CaballeroNo ratings yet
- Lesson 1 Elements and Principles of Visual Arts PDFDocument14 pagesLesson 1 Elements and Principles of Visual Arts PDFEllain CaballeroNo ratings yet
- Ginisang Sitaw at Kalabasa - 45: Kaldereta - 50Document1 pageGinisang Sitaw at Kalabasa - 45: Kaldereta - 50Ellain CaballeroNo ratings yet
- Acute Viral Gastroenteritis in Adults - UpToDateDocument14 pagesAcute Viral Gastroenteritis in Adults - UpToDatedaniso12No ratings yet
- Healthcare Associated InfectionDocument11 pagesHealthcare Associated InfectionPankajNo ratings yet
- eMRCS Microbiology 19 QuestionsDocument7 pageseMRCS Microbiology 19 QuestionsSaad KhanNo ratings yet
- Complete Bacteriology Notes From Levinson by Medical Study CenterDocument13 pagesComplete Bacteriology Notes From Levinson by Medical Study CenterUsama HameedNo ratings yet
- Infection Prevention and Control Prsactices 1570477491 PDFDocument29 pagesInfection Prevention and Control Prsactices 1570477491 PDFLarr SumalpongNo ratings yet
- Collection and Transportation of Microbiology SpecimensDocument4 pagesCollection and Transportation of Microbiology SpecimensanupreetNo ratings yet
- Etiology: 1.urinary RetentionDocument38 pagesEtiology: 1.urinary RetentionAbdurre YNo ratings yet
- Management of Acute Chemotherapy-Related Diarrhea - UpToDateDocument19 pagesManagement of Acute Chemotherapy-Related Diarrhea - UpToDateMarius PapuricaNo ratings yet
- Esomeprazole Tablets GranulesDocument57 pagesEsomeprazole Tablets GranulesMohammed shamiul ShahidNo ratings yet
- Micro - Systemic Bacteriology Questions PDFDocument79 pagesMicro - Systemic Bacteriology Questions PDFShashipriya AgressNo ratings yet
- NMC CBT Mock Test 2Document13 pagesNMC CBT Mock Test 2Charles Osiako100% (3)
- PDF Share Prescribing Information: Mechanism of ActionDocument3 pagesPDF Share Prescribing Information: Mechanism of Actionmehul da aviatorNo ratings yet
- Mtap-Bacte-Ratio-11-19-22 2Document9 pagesMtap-Bacte-Ratio-11-19-22 2lansangan.regine.coeliNo ratings yet
- 2013 AAFP Acute Diarrhea PDFDocument11 pages2013 AAFP Acute Diarrhea PDFJoseph AndradeNo ratings yet
- Xenex Effectiveness Summary Studies PDFDocument4 pagesXenex Effectiveness Summary Studies PDFREDENLAKE LTDNo ratings yet
- Pharmacological and Parenteral TherapiesDocument99 pagesPharmacological and Parenteral TherapieslNo ratings yet
- Assessing With EliminationDocument79 pagesAssessing With EliminationhalayehiahNo ratings yet
- Clindamycin 1Document21 pagesClindamycin 1ksachchuNo ratings yet
- Nutrition Pathway For Clostridium Difficile Infection (CDI) Colitis in Long-Term CareDocument4 pagesNutrition Pathway For Clostridium Difficile Infection (CDI) Colitis in Long-Term CareDavide CezarNo ratings yet
- Gastroenteritis: Saima Alam AfridiDocument23 pagesGastroenteritis: Saima Alam AfridiMahnoor ParvezNo ratings yet
- History of Hospital-Acquired InfectionsDocument16 pagesHistory of Hospital-Acquired InfectionsRasha MuhammadNo ratings yet
- Lec4 TransDocument23 pagesLec4 TransErika PatarayNo ratings yet
- Chapter 43 - Miscellaneous Bacterial Infections of GITDocument52 pagesChapter 43 - Miscellaneous Bacterial Infections of GITpooja pandeyNo ratings yet
- Symptoms of ColitisDocument5 pagesSymptoms of ColitisChatrina TandiloloNo ratings yet
- Ciprofloxacin TAB MonographDocument56 pagesCiprofloxacin TAB MonographSelvi RahmatiaNo ratings yet
- UW Infectious Diseases + Microbiology Educational Objectives PDFDocument75 pagesUW Infectious Diseases + Microbiology Educational Objectives PDFDrbee10No ratings yet
- The Gram-Positive Bacilli of Medical Importance: Group 5Document148 pagesThe Gram-Positive Bacilli of Medical Importance: Group 5Tolentino, Ma. LykaNo ratings yet
- Jase Medical Antibiotic GuideDocument33 pagesJase Medical Antibiotic GuideelectronicoscaldasNo ratings yet
- Ranicef Tablets Cefdinir Tablets 300MG FidsonDocument13 pagesRanicef Tablets Cefdinir Tablets 300MG FidsonWright JohnNo ratings yet