Download as pdf or txt
You might also like
- Property 2 Notes&BriefsDocument48 pagesProperty 2 Notes&BriefsHaifaNo ratings yet
- Ann Rea - Discovery JournalDocument47 pagesAnn Rea - Discovery JournalKarolis KauneckasNo ratings yet
- AUBF - Chapter 1Document7 pagesAUBF - Chapter 1Kristin SoquilloNo ratings yet
- Sofitel Philippine Plaza Manila Cultural Orientations FrameworkDocument3 pagesSofitel Philippine Plaza Manila Cultural Orientations FrameworkApril Jane EvangelistaNo ratings yet
- 01 Lecture Human OrganismDocument26 pages01 Lecture Human Organismalyssa_marie_keNo ratings yet
- Cardiovascular System Heart ReviewerDocument8 pagesCardiovascular System Heart ReviewerImmanuel Cris PalasigueNo ratings yet
- Pcol QSDocument17 pagesPcol QSFaye Kashmier Embestro NamoroNo ratings yet
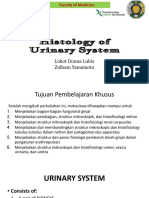
- Histology of Urinary SystemDocument36 pagesHistology of Urinary Systemdiraf100% (2)
- Urinary SystemDocument9 pagesUrinary SystemRaven LacsonNo ratings yet
- Urinary Tract ReciewDocument5 pagesUrinary Tract ReciewRobert LotzerNo ratings yet
- Anatomy and Physiology With Pathophysiology TransesDocument10 pagesAnatomy and Physiology With Pathophysiology Transeshezekiah minNo ratings yet
- ConnectivetissuepptDocument20 pagesConnectivetissuepptChicco De AngelisNo ratings yet
- Unit - 4-3 - Blood and Tissue NematodesDocument130 pagesUnit - 4-3 - Blood and Tissue NematodesDembalu NuguseNo ratings yet
- MTHISTO100 Lesson 2 Excretory SystemDocument9 pagesMTHISTO100 Lesson 2 Excretory SystemJaeri HuangNo ratings yet
- 1.overview of The Microbial World, Origins andDocument50 pages1.overview of The Microbial World, Origins andSamuel BandaNo ratings yet
- Tissue TableDocument4 pagesTissue TableMarcie BooneNo ratings yet
- ANPH-M2-CU9. Respiratory SystemDocument8 pagesANPH-M2-CU9. Respiratory SystemMary Grace Mapula100% (1)
- Analysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)Document11 pagesAnalysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)jeffreyNo ratings yet
- Electrical Properties of The HeartDocument25 pagesElectrical Properties of The HeartSherwan R Shal100% (3)
- Microbiology Lecture 1 - Structure, Classification and MorphologyDocument4 pagesMicrobiology Lecture 1 - Structure, Classification and MorphologyAldwin BagtasNo ratings yet
- Connective TissuesDocument5 pagesConnective Tissuesraphael100% (1)
- Physiology of The Digestive System (GIT) : The Gastrointestinal System Carries Out The Following ActivitiesDocument53 pagesPhysiology of The Digestive System (GIT) : The Gastrointestinal System Carries Out The Following ActivitiesBelay MulugetaNo ratings yet
- Venipuncture Complications and Preexamination Variables: RequistionsDocument19 pagesVenipuncture Complications and Preexamination Variables: RequistionsAngel Cascayan Delos SantosNo ratings yet
- Connective Tissues: Rochelle M. Delos Santos Ii-A1 Bs-BiologyDocument54 pagesConnective Tissues: Rochelle M. Delos Santos Ii-A1 Bs-BiologyJordan Ramos100% (1)
- REV Micro HSB RemedsDocument16 pagesREV Micro HSB RemedsPatricia HariramaniNo ratings yet
- Histology of Urinary SystemDocument53 pagesHistology of Urinary SystemA1205Angelica GloryNo ratings yet
- Group 3 - ParasitologyDocument8 pagesGroup 3 - Parasitologyjulo_05No ratings yet
- LipidsDocument12 pagesLipidsOsannah Irish InsongNo ratings yet
- Anaphy Practice TestsDocument6 pagesAnaphy Practice TestsHenie Louise HinanayNo ratings yet
- Bacte Lec - Prelim ExamDocument84 pagesBacte Lec - Prelim ExamDanielle Anne LambanNo ratings yet
- Course Outline FUNCORE 102 General Zoology 1st Sem 2022-2023Document5 pagesCourse Outline FUNCORE 102 General Zoology 1st Sem 2022-2023Gracia NicolaiNo ratings yet
- 6 Ra 1517Document56 pages6 Ra 1517Jay Andrea Vea Dayuday-IsraelNo ratings yet
- Special Senses NotesDocument3 pagesSpecial Senses NotesChelsa LeyritanaNo ratings yet
- Accurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andDocument4 pagesAccurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andManulat VicaiiNo ratings yet
- Transes Anaphy LEC (Activity 5 HISTOLOGY)Document6 pagesTranses Anaphy LEC (Activity 5 HISTOLOGY)Reign Saplaco100% (1)
- PMLS2 LEC - Circulatory SystemDocument4 pagesPMLS2 LEC - Circulatory SystemCorinne Bautista RenivaNo ratings yet
- Para Lec ReviewerDocument18 pagesPara Lec ReviewerRudolph MendozaNo ratings yet
- Compilation Medsurg PrelimsDocument29 pagesCompilation Medsurg PrelimsEunice CuñadaNo ratings yet
- PMLS Lesson 9 Gelig PDFDocument6 pagesPMLS Lesson 9 Gelig PDFCaren Acabal100% (1)
- Prothrombin Time (Protime) : Activity #9Document20 pagesProthrombin Time (Protime) : Activity #9Kei Ef SiNo ratings yet
- HTMLE SEMINAR NOTES DOC. ORTEGA - CompressedDocument35 pagesHTMLE SEMINAR NOTES DOC. ORTEGA - CompressedNISSI JUNE T. UNGABNo ratings yet
- Aubf BrunzelDocument42 pagesAubf Brunzelabigail lausNo ratings yet
- (Transes) Human Histology - 13 Lymphoid SystemDocument17 pages(Transes) Human Histology - 13 Lymphoid SystemReina CastronuevoNo ratings yet
- Microbiology MCQS: BacteriaDocument13 pagesMicrobiology MCQS: BacteriaIqbal HussainNo ratings yet
- (Transes) Human Histology - 14 Respiratory SystemDocument17 pages(Transes) Human Histology - 14 Respiratory SystemReina CastronuevoNo ratings yet
- Psthe 1Document111 pagesPsthe 1Angelica RicoNo ratings yet
- Histology Model ADocument7 pagesHistology Model AOzgan SüleymanNo ratings yet
- 1 IntroDocument5 pages1 IntroJeanjayannseptoeman100% (1)
- DehydrationDocument56 pagesDehydrationSkylarNo ratings yet
- Physiology: Block 1Document3 pagesPhysiology: Block 1Mavic VillanuevaNo ratings yet
- MLS - HISTOLOGY Lec - M2-UNIT1 (Epithelia and Glands)Document22 pagesMLS - HISTOLOGY Lec - M2-UNIT1 (Epithelia and Glands)ataraNo ratings yet
- Anatomy and Physiology,: Lecture OutlineDocument46 pagesAnatomy and Physiology,: Lecture OutlineRhona AngelaNo ratings yet
- Group 4 - General Pathology, Logic and Cytologic TechniquesDocument11 pagesGroup 4 - General Pathology, Logic and Cytologic Techniquesjulo_05No ratings yet
- Virtual Microscopy Histology Manual: University of Alabama at Birmingham School of MedicineDocument6 pagesVirtual Microscopy Histology Manual: University of Alabama at Birmingham School of Medicinelucky mbaselaNo ratings yet
- Connective TissueDocument7 pagesConnective TissueSheena Pasion100% (1)
- Hemoglobin DeterminationDocument1 pageHemoglobin DeterminationLecture NotesNo ratings yet
- Micro paraDocument7 pagesMicro paraAj MillanNo ratings yet
- Chemical Examination of Fecal SpecimenDocument4 pagesChemical Examination of Fecal SpecimenLois DanielleNo ratings yet
- SASDocument4 pagesSASNicole Ken AgdanaNo ratings yet
- Cestodes 2020Document10 pagesCestodes 2020CDNo ratings yet
- ANPH 111 (Anatomy and Physiology) : Bachelor of Science in NursingDocument11 pagesANPH 111 (Anatomy and Physiology) : Bachelor of Science in NursingMary Grace MapulaNo ratings yet
- Urinary System - Histology March 2023Document123 pagesUrinary System - Histology March 2023bschaliyath.mnlNo ratings yet
- 03 Anatomy of The Kidney and Nephron - SiDocument3 pages03 Anatomy of The Kidney and Nephron - SiGerarld Immanuel KairupanNo ratings yet
- Side Effects of VaccineDocument2 pagesSide Effects of VaccinegabbybibobuNo ratings yet
- Misinformations On Covid-19Document2 pagesMisinformations On Covid-19gabbybibobuNo ratings yet
- BioethicsDocument11 pagesBioethicsgabbybibobuNo ratings yet
- Reproductive SystemDocument11 pagesReproductive SystemgabbybibobuNo ratings yet
- S4-4 Damping Paper TakedaDocument26 pagesS4-4 Damping Paper TakedaRonald Omar García RojasNo ratings yet
- NSSBCHM Activity 16 LabDocument4 pagesNSSBCHM Activity 16 Labsad asdNo ratings yet
- This Question Has Been Answered: Find Study ResourcesDocument1 pageThis Question Has Been Answered: Find Study ResourcesAllana MierNo ratings yet
- Historical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaDocument15 pagesHistorical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaSonjce Marceva100% (2)
- Group Medical Insurance - 2020-21Document2 pagesGroup Medical Insurance - 2020-21Vilaz VijiNo ratings yet
- U5 - Ultrasonic InspectionDocument83 pagesU5 - Ultrasonic InspectionSuraj B SNo ratings yet
- Drilling Assignment 1Document20 pagesDrilling Assignment 1Charles Adefemi OmowoleNo ratings yet
- Brief Background and OverviewDocument2 pagesBrief Background and OverviewCamille MarieNo ratings yet
- Abstract Book INAACCDocument83 pagesAbstract Book INAACCrodtobingNo ratings yet
- Initial Investment Invested: Basic Steps: A L + C Expanded Form: A L + C - (D) + R / I - (E)Document9 pagesInitial Investment Invested: Basic Steps: A L + C Expanded Form: A L + C - (D) + R / I - (E)Charlize Adriele C. Comprado3210183No ratings yet
- 9286 Ds Opsycom PFPDocument2 pages9286 Ds Opsycom PFPamir11601No ratings yet
- Anil Laul BharaniDocument30 pagesAnil Laul BharaniBharani MadamanchiNo ratings yet
- ENGG 325 - Electric Circuits and Systems Midterm ExaminationDocument9 pagesENGG 325 - Electric Circuits and Systems Midterm ExaminationTaha EtemNo ratings yet
- Lymphoproliferative DisordersDocument36 pagesLymphoproliferative DisordersBrett FieldsNo ratings yet
- Steam TurbineDocument16 pagesSteam TurbineVinayakNo ratings yet
- Proposal Writing-Final PresentationDocument16 pagesProposal Writing-Final PresentationPhirum KuntheaNo ratings yet
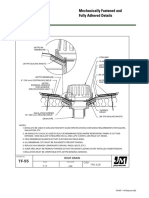
- JM Mechanically Fastened and Adhered Details UltraGard TPO Roof Drain New Construction Detail Drawing B18270Document1 pageJM Mechanically Fastened and Adhered Details UltraGard TPO Roof Drain New Construction Detail Drawing B18270michael jan tubongbanuaNo ratings yet
- Exadata and Database Machine Administration Workshop PDFDocument316 pagesExadata and Database Machine Administration Workshop PDFusman newtonNo ratings yet
- A CLFILE Is A ANSI Standard Generic Output File For ToolDocument2 pagesA CLFILE Is A ANSI Standard Generic Output File For ToolFadetwoNo ratings yet
- All India Companies Directory - Database - List (.XLSX Excel Format) 11th EditionDocument2 pagesAll India Companies Directory - Database - List (.XLSX Excel Format) 11th EditionAVNo ratings yet
- (Oral Ana) Molars Gen CharacteristicsDocument24 pages(Oral Ana) Molars Gen CharacteristicsVT Superticioso Facto - TampusNo ratings yet
- Allama Iqbal Open University, Islamabad (Department of Business Administration) WarningDocument5 pagesAllama Iqbal Open University, Islamabad (Department of Business Administration) WarningRana Tauqeer HaiderNo ratings yet
- Symbiosis PresentationDocument7 pagesSymbiosis Presentationmisterbrowner@yahoo.com100% (1)
- MicroZed-3.3 Operators Manual SW v9.00Document64 pagesMicroZed-3.3 Operators Manual SW v9.00Emeka Pius Oramunwa100% (1)
- Final - Thesis Quantum Study Silicon NanowiresDocument154 pagesFinal - Thesis Quantum Study Silicon NanowiresChandra Bhal SinghNo ratings yet
- Chain Surveying Obstacles PPT DownloadDocument24 pagesChain Surveying Obstacles PPT DownloadKreesthu Reddy100% (1)
- PDF PMP Exam Quick Reference GuideDocument8 pagesPDF PMP Exam Quick Reference GuideNantha KumarNo ratings yet