Download as pdf or txt
You might also like
- Rodney Jones v. Sean Combs - Lawsuit in New York Southern DistrictDocument79 pagesRodney Jones v. Sean Combs - Lawsuit in New York Southern DistrictWKYC.com100% (7)
- Fully Blooded Felons IndictmentDocument44 pagesFully Blooded Felons IndictmentWKYC.com100% (1)
- Akron Public Schools Transition ReportDocument68 pagesAkron Public Schools Transition ReportWKYC.comNo ratings yet
- STRS DocumentDocument14 pagesSTRS DocumentWKYC.comNo ratings yet
- Finnell Personnel ReportDocument13 pagesFinnell Personnel ReportWKYC.com100% (1)
- Zubair Brothers IndictmentDocument35 pagesZubair Brothers IndictmentWKYC.comNo ratings yet
- Air Pollution Exposure and Cardiometabolic RiskDocument13 pagesAir Pollution Exposure and Cardiometabolic RiskWKYC.comNo ratings yet
- Ohio Suicide Prevention Plan 2024-2026Document17 pagesOhio Suicide Prevention Plan 2024-2026WKYC.comNo ratings yet
- 22-08-21 - OSR - CO-SUPER CHAINA - Jee-Adv - GTA-24 (P-I) - SYLLABUS: Sec: OSR - IIT - CO-SC Date: 22-08-21 Time: 3HRS Max. Marks: 183Document19 pages22-08-21 - OSR - CO-SUPER CHAINA - Jee-Adv - GTA-24 (P-I) - SYLLABUS: Sec: OSR - IIT - CO-SC Date: 22-08-21 Time: 3HRS Max. Marks: 183SaviiNo ratings yet
- Argumentative Essay Medical MarijuanaDocument7 pagesArgumentative Essay Medical MarijuanaMaxim Dahan100% (1)
- Review of Related LiteratureDocument25 pagesReview of Related LiteratureKarlvin De CardoNo ratings yet
- Medical Cannabis: A Guide for Patients, Practitioners, and CaregiversFrom EverandMedical Cannabis: A Guide for Patients, Practitioners, and CaregiversRating: 5 out of 5 stars5/5 (1)
- CENTRAL ANALGETICS Analgesics Chemistry Pharmacology of Drugs Daniel Lednicer 1982Document236 pagesCENTRAL ANALGETICS Analgesics Chemistry Pharmacology of Drugs Daniel Lednicer 1982BASKAR.LNo ratings yet
- DR Jockers 30 Cancer Fighting SuperfoodsDocument96 pagesDR Jockers 30 Cancer Fighting SuperfoodsViolet Violet100% (1)
- Ending The US Government's War On MMJ ResearchDocument21 pagesEnding The US Government's War On MMJ ResearchMichael_Lee_RobertsNo ratings yet
- Running Head: Solving The Us Opioid Epidemic 1Document6 pagesRunning Head: Solving The Us Opioid Epidemic 1api-356639019No ratings yet
- Medical Marijuana: "Take A Deep Breath"Document26 pagesMedical Marijuana: "Take A Deep Breath"MarkNo ratings yet
- Alliah Causapin Research Chapter 2Document8 pagesAlliah Causapin Research Chapter 2Klein CausapinNo ratings yet
- Literature Review About DrugsDocument9 pagesLiterature Review About Drugsafmzslnxmqrjom100% (1)
- Cara PaperDocument11 pagesCara Paperapi-392400343No ratings yet
- 2 Pharma ModuleDocument227 pages2 Pharma ModuleCielina BatangNo ratings yet
- Composition 2 Final Research Paper - Madison EisnerDocument10 pagesComposition 2 Final Research Paper - Madison Eisnerapi-643978594No ratings yet
- Prescription Painkillers: History, Pharmacology, and TreatmentFrom EverandPrescription Painkillers: History, Pharmacology, and TreatmentNo ratings yet
- Vaccine Foia ComplaintDocument20 pagesVaccine Foia ComplaintAngel Capellan100% (1)
- Introduction Into Pharmacology 2029Document8 pagesIntroduction Into Pharmacology 2029mohammaddammagNo ratings yet
- Editorial: Chronic Noncancer Pain Management and Opioid Overdose: Time To Change Prescribing PracticesDocument3 pagesEditorial: Chronic Noncancer Pain Management and Opioid Overdose: Time To Change Prescribing PracticesErick Gomez LaraNo ratings yet
- PrimaryDocument3 pagesPrimaryapi-358143741No ratings yet
- Herbal Medicine Regulation in China, Germany, andUSDocument9 pagesHerbal Medicine Regulation in China, Germany, andUSNancy KawilarangNo ratings yet
- The DEA Position On MarijuanaDocument63 pagesThe DEA Position On MarijuanaBrian HarrisNo ratings yet
- Co-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug InteractionsDocument19 pagesCo-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug Interactionsadern-07huepfendNo ratings yet
- Mainly in The Main Drug Consumer, The United States, There Won't EvenDocument5 pagesMainly in The Main Drug Consumer, The United States, There Won't EvenRonik MalikNo ratings yet
- AB345 - Fentanyl Test Strips Infosheet - Dr. Stephanie Woodard - DHHSDocument2 pagesAB345 - Fentanyl Test Strips Infosheet - Dr. Stephanie Woodard - DHHSsaraes88No ratings yet
- Senate Hearing, 108TH Congress - Prescription Drug Abuse and Diversion: The Role of Prescription Drug Monitoring ProgramsDocument61 pagesSenate Hearing, 108TH Congress - Prescription Drug Abuse and Diversion: The Role of Prescription Drug Monitoring ProgramsScribd Government DocsNo ratings yet
- Individual Assignment 1Document8 pagesIndividual Assignment 110PAMP2Dionisio, Ira Joy D.No ratings yet
- Article-Aman Kumar Singh-GNLU-8.12.2020Document12 pagesArticle-Aman Kumar Singh-GNLU-8.12.2020VeronicaNo ratings yet
- Final Annotated BibliographyDocument11 pagesFinal Annotated Bibliographyapi-358143741No ratings yet
- Perspective Herb - Drug Interactions: Challenges and Opportunities For Improved PredictionsDocument17 pagesPerspective Herb - Drug Interactions: Challenges and Opportunities For Improved PredictionsGaby ValenzuelaNo ratings yet
- Article AnalysisDocument7 pagesArticle Analysisapi-602219685No ratings yet
- Research Paper On Medical CannabisDocument8 pagesResearch Paper On Medical Cannabisegyr68dw100% (1)
- FDA Comment Filed 8-31-20 Device PatentsDocument6 pagesFDA Comment Filed 8-31-20 Device PatentsCaleb HollowayNo ratings yet
- Ten (10) Medicinal Plants Approved byDocument15 pagesTen (10) Medicinal Plants Approved byMichael UrrutiaNo ratings yet
- Prescription Drug Prices: Background InformationDocument3 pagesPrescription Drug Prices: Background InformationAmitShettyNo ratings yet
- Individual Assignment 1Document6 pagesIndividual Assignment 1Che InopiaNo ratings yet
- Prescription Drugs Thesis StatementDocument8 pagesPrescription Drugs Thesis StatementMartha Brown100% (2)
- 4 5908977475685188520 PDFDocument660 pages4 5908977475685188520 PDFsolin27No ratings yet
- PharmacologyDocument88 pagesPharmacologyالدنيا ساعة فاجعلها طاعة100% (2)
- Gayoso Position PaperDocument8 pagesGayoso Position PaperJayvee GayosoNo ratings yet
- From Idea To MarketDocument6 pagesFrom Idea To MarketvictorccNo ratings yet
- The CSA and FederalismDocument3 pagesThe CSA and FederalismAlyssa LynnNo ratings yet
- Medical Marijuana Thesis StatementDocument8 pagesMedical Marijuana Thesis Statementangieleeportland100% (2)
- 2014 DEA: Four Decades of Impeding and Rejecting ScienceDocument16 pages2014 DEA: Four Decades of Impeding and Rejecting ScienceJames CampbellNo ratings yet
- The Legalization of Medical Marijuana in The PhilippinesDocument15 pagesThe Legalization of Medical Marijuana in The PhilippinesWazzo SantillanNo ratings yet
- Marijuana Research Paper Thesis StatementDocument7 pagesMarijuana Research Paper Thesis Statementgw11pm8h100% (1)
- Opioid CrisisDocument5 pagesOpioid CrisisLorine IchingwaNo ratings yet
- Personalized Medicine: The Promise of Pharmacogenomics Nancy ReinholdDocument9 pagesPersonalized Medicine: The Promise of Pharmacogenomics Nancy Reinholdnan-toddNo ratings yet
- Substance Use DisorderDocument13 pagesSubstance Use Disorderapi-591817398No ratings yet
- Medical Marijuana PowerpointDocument71 pagesMedical Marijuana PowerpointPagulayan Natividad Aljan100% (1)
- Drug Abuse Dissertation ResearchDocument5 pagesDrug Abuse Dissertation ResearchBuyCheapPapersOnlineOmaha100% (1)
- DeathbyMedicine March09bf2faloonDocument93 pagesDeathbyMedicine March09bf2faloonKwini YaoNo ratings yet
- Marijuana Toxicity Heavy Metal Exposure Through Statesponsored Accessto La Fee Verte 2167 7689 1000202Document10 pagesMarijuana Toxicity Heavy Metal Exposure Through Statesponsored Accessto La Fee Verte 2167 7689 1000202crononimeNo ratings yet
- Medical Cannabis Legalization. Legal Research. LM3 1Document6 pagesMedical Cannabis Legalization. Legal Research. LM3 1Kyle MercadoNo ratings yet
- Ch01 Introduction To DrugsDocument9 pagesCh01 Introduction To DrugsAina M. InidalNo ratings yet
- Outline FentanylDocument11 pagesOutline FentanylKarwa EspinozaNo ratings yet
- 28 CoordinatingcannabisdataDocument3 pages28 CoordinatingcannabisdataAlfredo MorenoNo ratings yet
- Chsaa State - Session 1Document13 pagesChsaa State - Session 1Ihita KataruNo ratings yet
- Position Paper On Marijuana As MedicineDocument4 pagesPosition Paper On Marijuana As Medicinenetmail2307100% (1)
- Marijuanaandlaw FinalDocument11 pagesMarijuanaandlaw Finalapi-283892872No ratings yet
- Drug Shortages: The Problem of Inadequate ProfitsDocument61 pagesDrug Shortages: The Problem of Inadequate ProfitsMona SalehNo ratings yet
- Juneteenth Objection Letter To Akron Mayor Shammas MalikDocument1 pageJuneteenth Objection Letter To Akron Mayor Shammas MalikWKYC.comNo ratings yet
- City of East Cleveland letter to Ohio Gov. Mike DeWineDocument1 pageCity of East Cleveland letter to Ohio Gov. Mike DeWineWKYC.comNo ratings yet
- Termination - Nicholas CastoDocument6 pagesTermination - Nicholas CastoWKYC.comNo ratings yet
- Extreme Heat SafetyDocument2 pagesExtreme Heat SafetyWKYC.comNo ratings yet
- Siegel and Shuster Tribute Plaza Presentation To Cleveland Planning CommissionDocument29 pagesSiegel and Shuster Tribute Plaza Presentation To Cleveland Planning CommissionWKYC.comNo ratings yet
- Clay Norris Federal Criminal ComplaintDocument11 pagesClay Norris Federal Criminal ComplaintWKYC.comNo ratings yet
- 14th Seminannual ReportDocument59 pages14th Seminannual ReportWews WebStaffNo ratings yet
- Statement On Akron Police Shooting From Okolo Law FirmDocument1 pageStatement On Akron Police Shooting From Okolo Law FirmWKYC.comNo ratings yet
- City of Cleveland Notice of Termination - Jakimah R. DyeDocument4 pagesCity of Cleveland Notice of Termination - Jakimah R. DyeWKYC.comNo ratings yet
- University Hospitals State of Research Address 2024Document62 pagesUniversity Hospitals State of Research Address 2024WKYC.comNo ratings yet
- Murray Resignation LetterDocument1 pageMurray Resignation LetterWKYC.comNo ratings yet
- The Rev. Raymond P. Guiao Letter On Frank CanfieldDocument3 pagesThe Rev. Raymond P. Guiao Letter On Frank CanfieldWKYC.comNo ratings yet
- University SquareDocument13 pagesUniversity SquareWKYC.comNo ratings yet
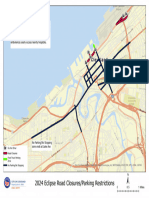
- Solar Eclipse Road ClosuresDocument1 pageSolar Eclipse Road ClosuresWKYC.comNo ratings yet
- GCDOA Services Rack Card FINAL 2024Document2 pagesGCDOA Services Rack Card FINAL 2024WKYC.comNo ratings yet
- Cedar Point DecisionDocument15 pagesCedar Point DecisionWKYC.comNo ratings yet
- K.D. Howard Resignation Letter To Mayor Justin BibbDocument1 pageK.D. Howard Resignation Letter To Mayor Justin BibbWKYC.comNo ratings yet
- CIFF48 Program LineupDocument68 pagesCIFF48 Program LineupWKYC.com0% (1)
- CIFF48 Program LineupDocument68 pagesCIFF48 Program LineupWKYC.com0% (1)
- School Bus Report FinalDocument13 pagesSchool Bus Report FinalWews WebStaffNo ratings yet
- From MaureenDocument1 pageFrom MaureenWKYC.comNo ratings yet
- From MaureenDocument1 pageFrom MaureenWKYC.comNo ratings yet
- Mcqs of BioremediationDocument2 pagesMcqs of Bioremediationzubaira zaffar100% (3)
- Quantitative: Analytical Chemistry (Qualitative and Chemistry)Document13 pagesQuantitative: Analytical Chemistry (Qualitative and Chemistry)Rizza OlivaNo ratings yet
- Released Procedures ReleasedProcedures 3614Document5 pagesReleased Procedures ReleasedProcedures 3614Vũ ĐứcNo ratings yet
- Experiment 1 Differences Between Organic and Inorganic CompoundsDocument3 pagesExperiment 1 Differences Between Organic and Inorganic CompoundsTinaa IamNo ratings yet
- 07 Piping BOQDocument54 pages07 Piping BOQHRK65No ratings yet
- 2017 - UV-Vis Analysis - Spectrophotometric Determination of Fe in Drinking Water PDFDocument5 pages2017 - UV-Vis Analysis - Spectrophotometric Determination of Fe in Drinking Water PDFCleiton Tavares PessoaNo ratings yet
- J. Biol. Chem. 1944 Greenberg 679 82Document5 pagesJ. Biol. Chem. 1944 Greenberg 679 82waraney palitNo ratings yet
- Module 9 PPTX For BoshDocument56 pagesModule 9 PPTX For BoshAdam MendozaNo ratings yet
- Qualitative Analysis of Some IonsDocument42 pagesQualitative Analysis of Some IonsShaina Mae ContilloNo ratings yet
- Nippon Vinilex 2000 PDFDocument7 pagesNippon Vinilex 2000 PDFRezka RamindaNo ratings yet
- 10 - Solution Stoichiometry Practice Questions With KEYDocument2 pages10 - Solution Stoichiometry Practice Questions With KEYJenny YoonNo ratings yet
- Cellactive - Hydro: The Apple-Fresh MoisturiserDocument19 pagesCellactive - Hydro: The Apple-Fresh MoisturiserRada PjanovicNo ratings yet
- High-Performance Photocatalytic Membranes For Water PurificationDocument20 pagesHigh-Performance Photocatalytic Membranes For Water PurificationMihaiNo ratings yet
- Newete2016 1 PDFDocument14 pagesNewete2016 1 PDFJesus Sanchez SolanoNo ratings yet
- A222 CoenzymesDocument4 pagesA222 Coenzymesramloghun veerNo ratings yet
- Sos 511 Lecture Note Power PointDocument97 pagesSos 511 Lecture Note Power Pointthemostwanted052No ratings yet
- Technical Handbook of Stainless Steel - 2003Document45 pagesTechnical Handbook of Stainless Steel - 2003يحيى عياش100% (1)
- BYK Intro - DispersionDocument3 pagesBYK Intro - DispersionQuimicosgenericosgaffaro GaffaroNo ratings yet
- Maintenance Products 1. Wear Abrasion Resistant Products: Salient FeaturesDocument12 pagesMaintenance Products 1. Wear Abrasion Resistant Products: Salient FeaturesjohnNo ratings yet
- Kito SanDocument5 pagesKito Sanmonica lestaryNo ratings yet
- Comparison of Stability of Cetirizine Dihydrochloride in Solid and Liquid Dosage Forms by HPLC Analytical MethodDocument9 pagesComparison of Stability of Cetirizine Dihydrochloride in Solid and Liquid Dosage Forms by HPLC Analytical MethodpryankaNo ratings yet
- 13 - 17.09.2020 - Webinar EPSC PS FundamentalsDocument33 pages13 - 17.09.2020 - Webinar EPSC PS FundamentalsRizkyNo ratings yet
- HACCP Model For Poultry SlaughterDocument19 pagesHACCP Model For Poultry Slaughterrimuru samaNo ratings yet
- Effect of Ceria Particle-Size Distribution and Pressure Interactions in Chemo-Mechanical Polishing (CMP) of Dielectric MaterialsDocument8 pagesEffect of Ceria Particle-Size Distribution and Pressure Interactions in Chemo-Mechanical Polishing (CMP) of Dielectric MaterialsAverage JoeNo ratings yet
- Material Data Sheet AluminioDocument14 pagesMaterial Data Sheet AluminioDavid CanticusNo ratings yet
- Chemclad SC PDFDocument2 pagesChemclad SC PDFskNo ratings yet
- Question Bank Atomic Structure: An Atom Uncharged ?Document13 pagesQuestion Bank Atomic Structure: An Atom Uncharged ?Tanay GuptaNo ratings yet
- Technical Data Manual: Vitodens 100-WDocument32 pagesTechnical Data Manual: Vitodens 100-WRed SquerrelNo ratings yet